
Abstract
Pseudoaneurysm is an extraluminal collection of blood with a turbulent flow that communicates with flowing arterial blood through a defect in the arterial wall. Uterine artery pseudoaneurysm (UAP) is considered a rare case that occurs in 2–3/1,000 deliveries. A 33-year-old pregnant woman was admitted for a planned caesarian section. After a successful delivery, the patient experienced a postpartum vaginal bleeding 3 days later. Sonography revealed a suspected right UAP, and the diagnosis was confirmed by angiography. The defect was treated by uterine artery embolization.
A pseudoaneurysm is defined as an extraluminal collection of blood with a turbulent flow that communicates with flowing arterial blood through a defect in the arterial wall. 1 Some authors have reported that a uterine artery pseudoaneurysm (UAP) occurs in 2–3/1,000 deliveries. 2 This condition has many causes, such as cesarean section, myomectomy, vaginal delivery, and hysterectomy. 3 Ciebiera et al 4 suggested that the UAP should be adequately treated because it is a potentially life-threatening lesion. Previous studies have shown that UAP can be diagnosed with gray-scale ultrasonography (U/S) and color Doppler, while diagnostic confirmation is made with computed tomography (CT). 5 Angiography is also useful in confirming a diagnosis of UAP, which was the process used to confirm the U/S diagnosis of UAP in this case report.
Case Report
In October 2019, a 33-year-old pregnant woman was admitted to the antenatal care unit at a Sudanese obstetric hospital for a planned caesarian section. After a successful delivery, the patient experienced postpartum vaginal bleeding 3 days after the caesarian section. Her hemoglobin was very low, with severe anemia and hypotension. Four units of red blood cells, crystalloids, and antibiotics were used to stabilize her situation. The U/S examination showed a hypoechoic area in the uterine cervical region. Color Doppler demonstrated a focal dilated right uterine artery, which measured 1.9 cm, and the blood flow pattern in the lesion area was a to-and-fro pattern (Figure 1; Video 1), indicating an arterial pseudoaneurysm. These findings led to the suspicion of a UAP, as a diagnosis for the patient. Angiography was conducted to confirm the diagnosis. The angiographic procedure was conducted by inserting a catheter through the right femoral artery, and the angiogram images showed a focal dilatation of the right uterine artery (Figures 2 A and B), which is a typical feature of a UAP. The condition was treated by transarterial catheter embolization using metallic coils. The patient had an uneventful recovery.
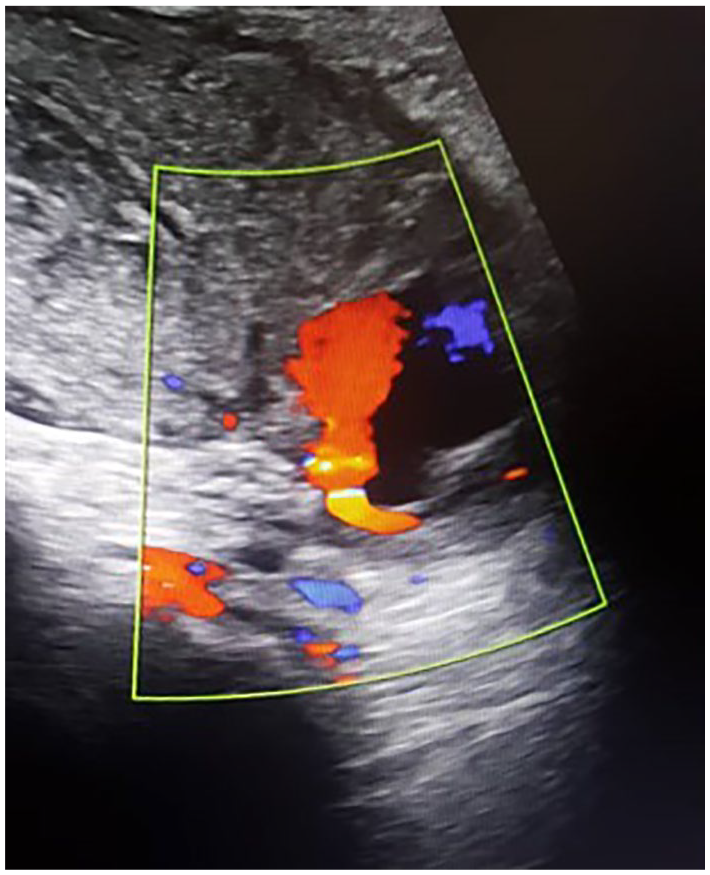
Color Doppler demonstrating right uterine artery pseudoaneurysm with a characteristic blood flow pattern (yin-yang pattern).
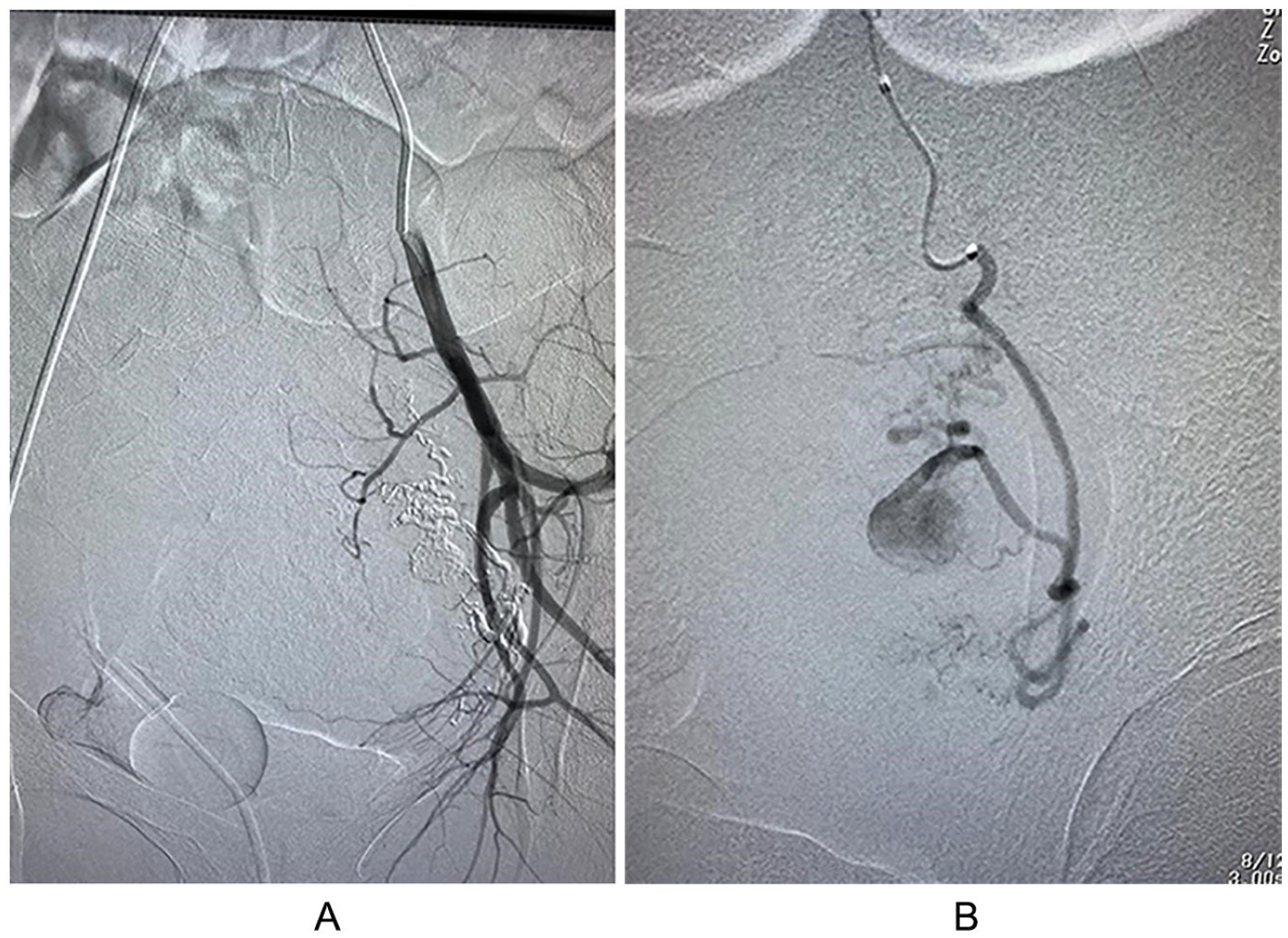
Angiographic confirmation of the right uterine artery pseudoaneurysm.
Discussion
The uterine artery arises from the internal iliac artery and travels caudally and anteriorly to reach the uterus just above the uterine cervical junction (Figure 3). It ascends to the border of the uterus, where its branches anastomose with the ovarian artery. 6 The uterine arteries (right and left) are the main blood vessels that supply blood to the uterus. They give off branches that supply different portions of the uterus and play an important role in maintaining blood supply during physiological processes, such as the altering of the endometrium during the menstrual cycle and growth of the uterus during pregnancy. 7
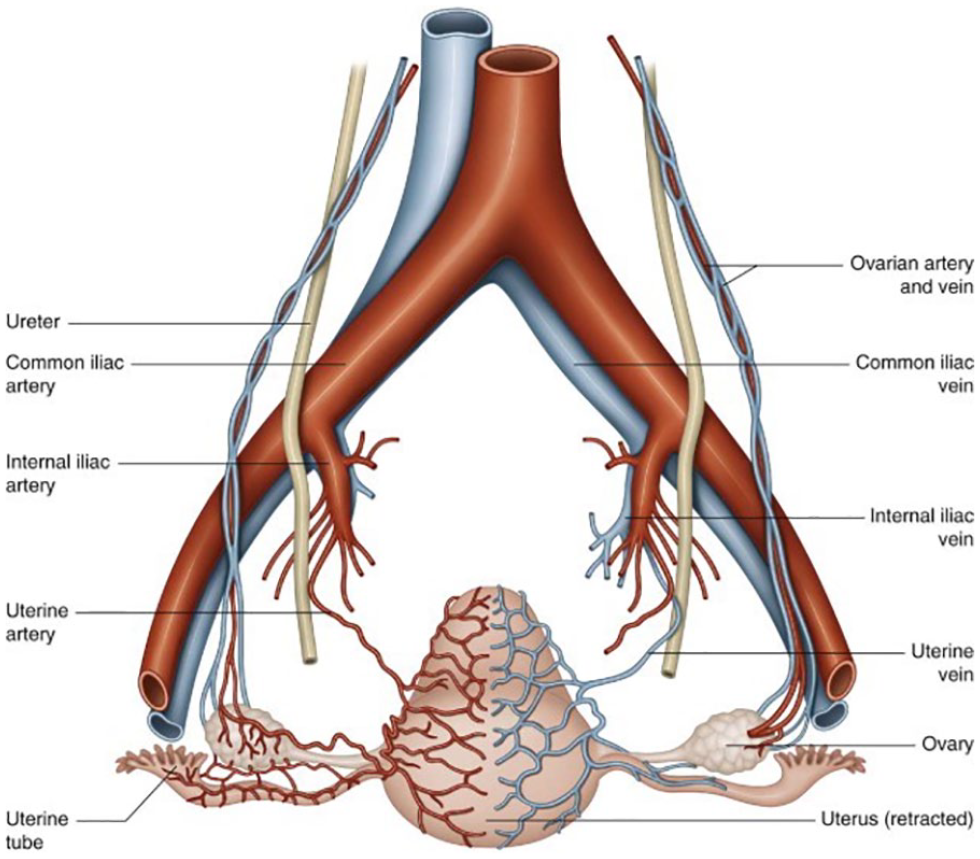
Anatomical diagram of the uterine arteries. 6
The normal artery wall contains three layers: the tunica intima, the tunica media, and the tunica adventitia. 8 The development of a pseudoaneurysm is due to an extraluminal blood collection that has a turbulent communication through an arterial wall defect. 1 The absence of a three-layered arterial wall lining in a pseudoaneurysm differentiates it from a true aneurysm. A UAP may be asymptomatic but usually presents with secondary postpartum hemorrhage (PPH) or delayed vaginal bleeding. 9
Some authors have indicated that UAP is a rare and potentially life-threatening lesion. 4 They described its mechanism as blood flowing into periarterial tissues after a wall defect. This creates a perfused sac, which communicates with the artery lumen. If the blood is fully covered by the adventitia or the surrounding tissues, a pseudoaneurysm is formed. Blood fills the sac during systole and flows away during diastole. Dar et al 5 stated that UAP usually develops after invasive procedures such as cesarean section, myomectomy, dilatation, and curettage.
Regarding the diagnosis of UAP, Chaudhry and Chaudhry 7 reported that uterine artery aneurysm should be among the differential diagnoses that are considered in pregnant women who present with pelvic and vaginal masses, vague bladder symptoms, or radiating pelvic pain. Some authors have reported that a UAP usually presents with vaginal bleeding, and its diagnosis includes a gray-scale U/S and color Doppler. 9 They added that, on duplex color Doppler, pseudoaneurysms appear as a saccular arterial out pouch or an abnormal dilatation of an artery, with surrounding hematoma. Karmous et al 10 have suggested that pseudoaneurysm has a characteristic sonographic appearance consisting of a pulsating anechoic or hypoechoic well-defined cystic structure with or without associated pelvic hematoma or free fluid. In the neck of the pseudoaneurysm, the “yin-yang” pattern may be potentially identified on duplex Doppler because the arterial blood flows like a jet (forward flow) into the aneurysm cavity during systole, then reverses (backward flow) into the original artery during diastole. The findings were similar to what had been seen in the currently reported case (Figure 1; Video 1).
Ciebiera et al 4 stated that the diagnosis of UAP can be obtained by color and spectral Doppler sonography and confirmed by angiography. Karmous et al 10 reported two cases of UAP; they used color Doppler in their diagnosis and conducted angiography as part of the treatment procedure for the first case. They treated the second case with based only on color Doppler imaging findings. In the current case study, standard procedures were followed for diagnosis and treatment. Also, the color Doppler findings were confirmed with angiography. Yeniel et al 11 reported a case of a 28-year-old patient who had a UAP. In this case, they failed to detect the UAP, which may have been due to depending only on gray-scale U/S and Doppler as their diagnostic method. In this case, the UAP was detected after an emergency laparotomy. Angiography is a useful imaging method for confirming the diagnosis; for the current patient, an angiographic procedure was performed to confirm the U/S diagnosis. A catheter was inserted through the right femoral artery, and the angiogram images showed a focal dilatation of the right uterine artery. The findings showed a typical feature of a UAP (Figures 2 A and B).
Digiacinto et al 12 concluded that follow-up CT is used to confirm the diagnosis identified on the sonogram. They stated that while CT is useful in identifying and diagnosing UAP, percutaneous angiography is considered the gold standard to diagnose a pseudoaneurysm and plays a role in the treatment as well. The differential diagnosis of UAPs includes acquired and congenital arteriovenous malformations, consisting of a web of mixed arteries and veins.
Regarding the treatment of UAP, there are different options in clinical applications. Some authors have shown that clinical treatments of UAP include transcatheter arterial embolization, uterine artery ligation, ultrasound-guided thrombin injection, and hysterectomy. 12 Kwon et al 13 mentioned that uterine artery embolization (UAE) using N-butyl-2-cyanoacrylate is safe and effective in patients with PPH who show evidence of extravasation or pseudoaneurysm. The current patient was treated with UAE; 4-A transfemoral with 2-F microcatheter selective angiographic catheters were used to perform the procedure. Stainless steel coils were used to occlude the pseudoaneurysm permanently.
Takahashi et al 14 studied three cases of UAP resulting from vacuum delivery, vacuum delivery with placental removal, and dilatation. They made the diagnosis for these three cases using color Doppler and found that all three patients recovered spontaneously, without UAE. The current case study disagrees with this hypothesis because the aforementioned case series indicated that all three patients experienced slight bleeding. They also did not confirm the case series diagnoses with angiography. Gurses et al 15 studied a case of a 21-year-old with UAP, which was easily diagnosed with duplex Doppler and treated with embolization. This conclusion supports the current case study report. Soyer et al 16 provided a similar conclusion; they reviewed seven case studies and showed that transcatheter arterial embolization is an effective and secure technique for the treatment of severe postpartum hemorrhage due to uterine or vaginal artery pseudoaneurysm.
Conclusion
Gray-scale U/S, color Doppler, and angiography were useful methods for diagnosing this UAP. The UAE was the optimum treatment for this patient. UAP should be carefully diagnosed through multiple diagnostic methods and should be adequately treated.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.