
Abstract
This case report demonstrates an unusual, vascularized solid mass in the right upper abdomen of a female patient ultimately identified as a uterine leiomyoma (fibroid). The patient’s past medical history was significant, having had a prior uterine artery embolization (UAE) procedure for symptomatic uterine fibroids.
Uterine artery embolization (UAE) was first used in the early 1990s for the treatment and relief of bleeding following cesarean section. It was observed that a significant number of fibroids decreased in size and related symptoms were relieved.1,2 Today, UAE provides a common nonsurgical option for the treatment of symptomatic uterine fibroids.3–8
Case Study
A woman in her mid-50s presented for an abdominal sonogram to investigate right upper quadrant and right flank pain. A sonographic examination was performed with a Toshiba Nemio system (Tustin, California) using a standard 6-MHz annular array transducer. The examination showed an 8.7-cm ovoid solid mass with scattered internal calcifications just inferior to the right kidney (Figures 1, 2). There did not appear to be any connection with the liver or kidney. Inspection of the mass with power and color Doppler revealed some internal vascular flow (Figure 3). The mass was nontender to palpation. The patient noted that in the past, she had been told that she had an abdominal mass called a fibroid. Further examination of the pelvis demonstrated an enlarged, heterogeneous uterus with multiple calcified fibroids (Figure 4).
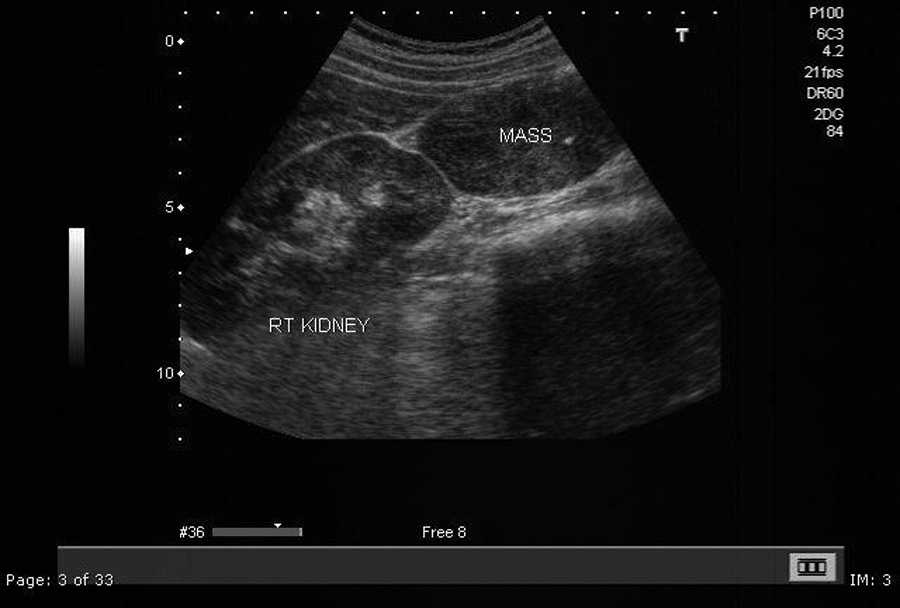
A longitudinal image demonstrates a mass just beneath the right kidney and liver.

On a long-axis image, the abdominal mass measures 8.7 cm.
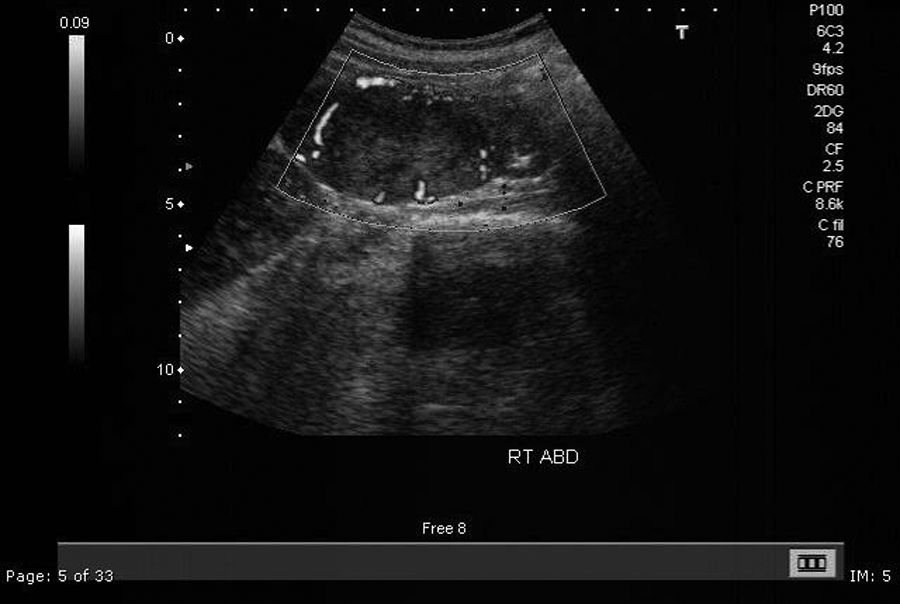
Power Doppler imaging demonstrates internal vascular flow.
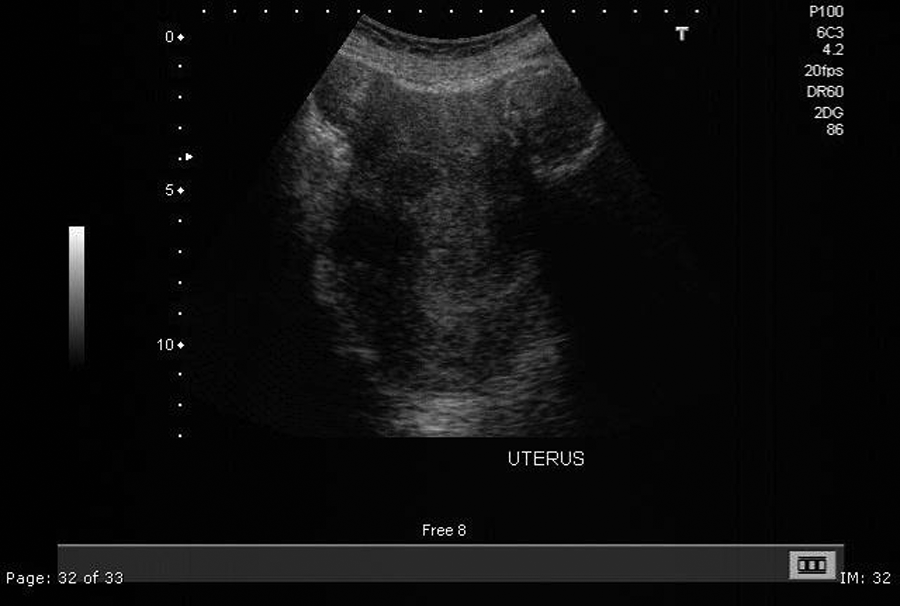
A transverse sonogram of the pelvis demonstrating an enlarged uterus with multiple calcified fibroids.
The patient’s medical history included diagnosis in 2006 of a left breast cancer by mammography and later confirmed by needle biopsy. Staging preoperative breast magnetic resonance imaging (MRI) and abdominal/pelvic computed tomography (CT) were performed. The breast MRI demonstrated a 2.8-cm heterogeneously enhancing mass with spiculated margins, consistent with the known breast carcinoma (Figure 5). The CT scan showed a solid mass adjacent to the inferior aspect of the right lobe of the liver (Figure 6). The mass appeared separate from the liver and right kidney and caused an extrinsic mass effect on the ascending colon. It was unclear at that time whether the mass was peritoneal or retroperitoneal. The remaining abdominal structures appeared normal.
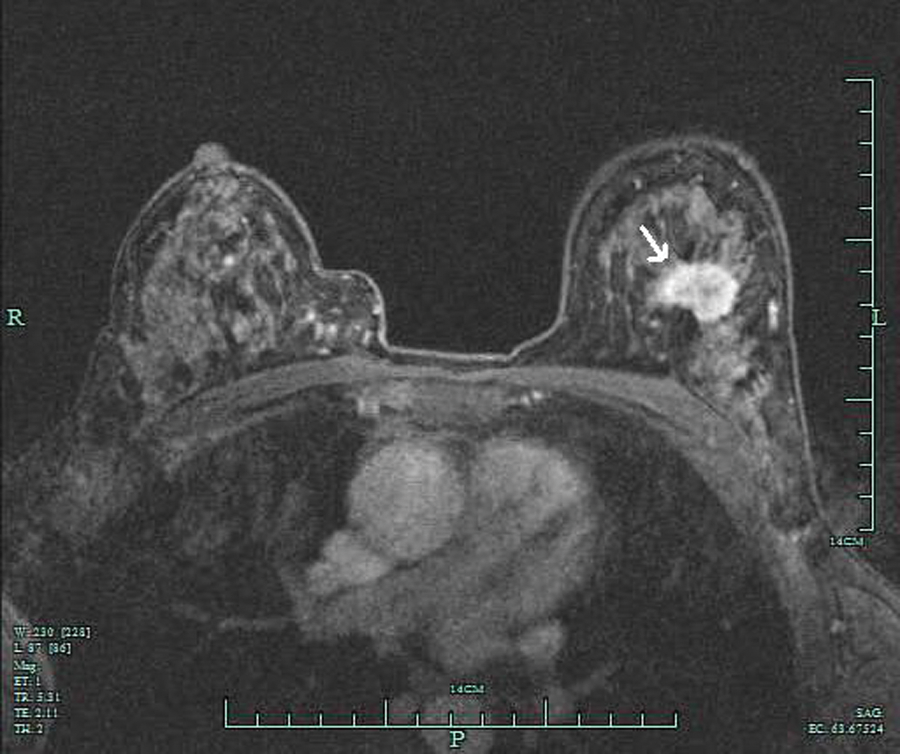
Breast magnetic resonance image of the patient’s left breast carcinoma.

Coronal computed tomography reconstruction demonstrating the abdominal mass just inferior to the liver and right kidney.
Etiology of the mass was unknown; however, a desmoid tumor was considered. CT imaging of the pelvis demonstrated an enlarged uterus with multiple calcified fibroids (Figure 7). Given the patient’s diagnosis of breast cancer, the mass was biopsied, and histopathologic evaluation identified the mass as a uterine leiomyoma (fibroid). Because the mass did not appear to be related to her current medical condition, her breast cancer was treated with lumpectomy, radiation therapy, and tamoxifen therapy. No further imaging or follow-up of the abdominal mass was recommended. Of note, two years prior to the breast cancer diagnosis, the patient had undergone a UAE for dysfunctional uterine bleeding due to multiple, large uterine fibroids. Her post-UAE course was eventful with severe pain and bleeding. Over a six-month period, her pain and bleeding eventually subsided.
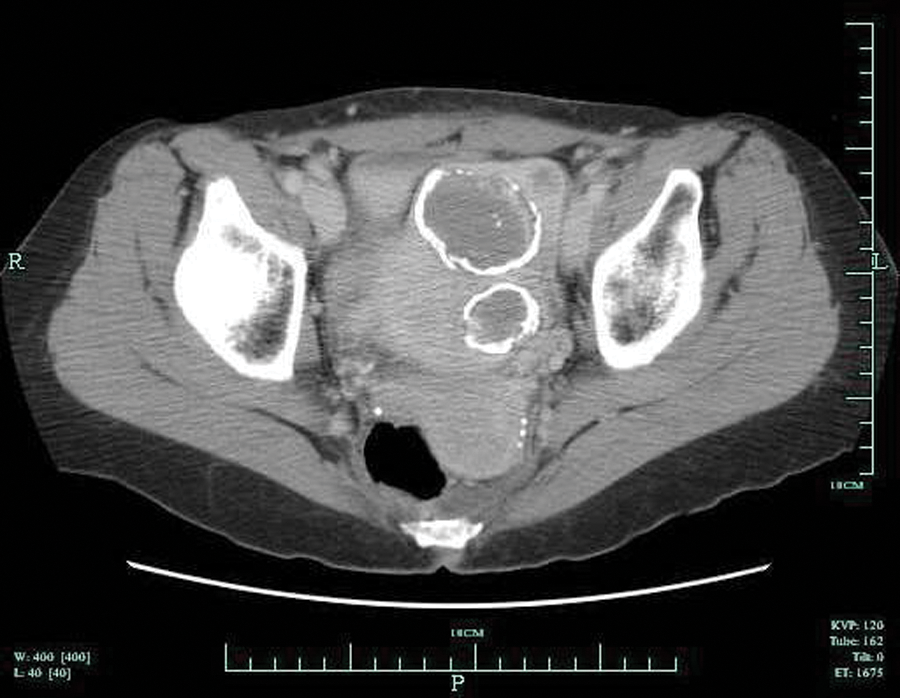
Transverse computed tomography image demonstrating the calcified uterine fibroids.
Comparison of the sonographic examination (Figure 2) and the prior abdominal CT (Figure 6) showed no significant changes in the size or characteristics of the fibroid. At the time of the current sonography examination, there was no reported recurrence of the breast cancer.
Discussion
Uterine leiomyomas (fibroids) are benign tumors that originate from the smooth muscle of the myometrium and the accompanying connective tissue of the uterus. They are the most common benign tumors in females and typically found during the middle and later reproductive years. As many as one in five women have fibroids during their childbearing years, and by age 50, up to 50% of women will have developed fibroids. They are rare in women younger than age 20 and are more common in African Americans than whites.9,10 The cause of uterine fibroids is unknown; however, growth of the leiomyomas is linked with estrogen and progesterone. Symptoms depend on the location and size of the fibroids. Important symptoms include abnormal gynecologic bleeding, heavy or painful menses, abdominal discomfort or bloating, back ache, urinary frequency or retention, and, in some cases, infertility. There may also be pain during intercourse, depending on the location of the fibroid. During pregnancy, the mass may cause a miscarriage, bleeding, premature labor, or interference with the position of the fetus. 11
UAE, also called uterine fibroid embolization, was first performed as a means to control bleeding following cesarean section. In the early 1990s, Dr J. H. Ravina, a gynecologist in Paris, France, noticed shrinkage of fibroids in patients who had undergone emergency uterine artery embolization for acute bleeding. On the basis of his observation, he asked interventional radiologists to embolize fibroids prior to myomectomy to reduce bleeding during surgery. They discovered that uterine artery embolization alone could relieve the symptoms of fibroids.1,2 As a result, a program in which UAE became an option for the treatment of fibroids began in Paris. The first such program in the United States started in 2006 at the University of California at Los Angeles. 12 Since then, UAE has grown into a common nonsurgical option for the treatment of symptomatic uterine fibroids.3–8
UAE involves making a small incision and guiding a catheter through the femoral artery in the groin to one of the uterine arteries; arteriography provides a map of the blood supply to the uterus and fibroids. Tiny plastic particles, about the size of sand grains, of tris-acryl gelatin or polyvinyl alcohol are injected through the catheter and lodge in the smaller arteries that branch out to the fibroids and choke off the blood supply. They remain permanently in the uterine arteries. With the blood supply cut off, most fibroids decrease in size over the course of 6 to 12 months. Eighty-five percent of women can experience significant reduction or complete resolution of their fibroid-related symptoms. UAE is, however, not without risk. There is a 1% chance of injury to the uterus, potentially leading to hysterectomy. Other risks include damage to the femoral artery, infection, pain, early onset of menopause, bleeding and passage of necrotic fibroid tissue, and fertility issues.
Besides this case study, there is only one article in the literature describing detachment of a uterine fibroid as a complication of UAE. 8 In this case, the detached fibroid mobilized and reattached in the mesentery, causing a small bowel obstruction. In our case, the fibroid was asymptomatic and found incidentally.
Conclusion
A vascularized abdominal fibroid, separate from the uterus, is rare. In this case, it appears that as a consequence of UAE, an entire, embolized uterine fibroid became necrotic and separated from the uterus. UAE presents a unique circumstance where exophytic or pedunculated fibroids would be the most likely candidates for detachment. Once free from the uterus, fibroids could move freely within the peritoneum, potentially reestablishing vascular flow from the blood vessel–rich mesentery.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.