
Abstract
Introduction:
Uterine fibroids are the commonest benign tumors of the reproductive tract in women of childbearing age. They are usually asymptomatic but can cause menorrhagia. Treatments include myomectomy and uterine artery embolization (UAE). The latter is a relatively new procedure, therefore of special interest.
Objectives:
We conducted a systematic review and meta-analysis of all published studies to provide a comprehensive outlook on the effectiveness of UAE by comparing its outcomes to those of myomectomy. Electronic databases (PubMed and Cochrane Central) were systematically searched from January 2000 to March 2022 for published randomized control trials, observational studies, and meta-analyses that compared UAE to myomectomy for at least one of the pre-specified outcomes, namely re-intervention rates, length of hospital stay, and complications.
Methods:
We shortlisted nine studies for the final analysis. For continuous outcomes, results from random-effects meta-analysis were presented as mean differences (MDs) and corresponding 95% confidence intervals (CIs). Risk ratios (RRs) for dichotomous outcomes were pooled using a random-effects model.
Results:
The final analysis consisted of nine studies. Factors like re-intervention, hospitalization, and complications, each with its unique follow-up duration were assessed. Pooled analysis demonstrated significant results for greater re-intervention rates with UAE as compared to myomectomy (RR: 2.16, 95% CI: (1.27–3.66), p-value 0.004, heterogeneity I2 = 85%). UAE holds a greater but statistically insignificant risk for major complications (RR: 0.62, 95% CI: (0.29–1.33), p-value 0.22, heterogeneity I2 = 0%) and myomectomy shows a statistically insignificant greater risk for minor complications (RR: 1.72, 95% CI: (0.92–3.22), p-value 0.09, heterogeneity I2 = 0%). UAE had a shorter but statistically insignificant duration of hospital stay (MD: −1.12, 95% CI: (−2.50 to 0.27), p-value 0.11, heterogeneity I2 = 96%) (p-value for subgroup differences = 0.005).
Conclusion:
Our meta-analysis of approximately 196,595 patients demonstrates that myomectomy results in a significant reduction in re-intervention rate compared to UAE.
Introduction
Uterine fibroids (leiomyomas or myomas) are benign tumors that generally occur during childbearing years. 1 The proliferation of myometrium leads to the development of fibroid nodules which differ in location, size, or number. 2 These growths are notably seen in three distinct locations within and around the uterus: submucosal (within the uterine cavity), intramural (within the muscular layer), and subserosal (outside the uterus). Fibroids are regarded to be estrogen-dependent tumors; there is evidence to suggest that leiomyomas tend to overexpress certain estrogen and progesterone receptors when compared with normal myometrium activity. 3 Fibroids can either present as an asymptomatic incidental finding on imaging or could present symptomatically in 70% of women by age 50. 3 Clinical symptoms that arise in fibroid patients include menstrual interferences (menorrhagia, metrorrhagia, intermenstrual bleeding, and dysmenorrhea), disruption of surrounding structures (bowel and bladder) leading to pressure symptoms (bowel disturbances, and increased urinary infrequency), and pelvic pain. 3 An apparent correlation of fibroids is also seen with pregnancy and infertility. 1
Uterine artery embolization (UAE) is a favorable treatment option for uterine fibroids (leiomyomas or leiomyomata) removal worldwide; it is a secure and practical method for women past child-bearing age and those who wish to undergo minimally invasive uterine preserving treatment. Women of childbearing age are eligible; however, they must receive a consultation before implementation. 4 The procedure involves sedating the patient using local anesthetics. An interventional radiologist injects a minute plastic or gelatin particle into the arteries supplying the fibroid mass using a catheter. The particle blocks off the artery supplying the fibroid mass, which subsequently results in its eradication. 5 In comparison, a myomectomy is a surgical option for women with symptomatic fibroids; it can either be performed as a conventional laparotomy (mini-laparotomy) or a minimal access technique (hysterectomy and laparoscopy). 6
UAE is typically preferred over myomectomy as it has a shorter hospital stay and faster recovery rate7,8 but has an increased possibility of re-intervention 9 which can be troublesome for most patients. However, myomectomy is more beneficial in improving patients’ quality of life; this equally is a favorable long-term asset in the lives of fibroid patients. 10 Nonetheless, it is undetermined whether the benefits of UAE outweigh the slower recovery time and higher cost associated with myomectomy. Hence, we conducted a meta-analysis to compare the effectiveness and safety of myomectomy and UAE in treating symptomatic uterine fibroids.
Moreover, UAE is a promising treatment option for uterine fibroids; it is essential to underscore the need for extra counseling, particularly for women of childbearing age. Unlike myomectomy, which is a surgical procedure that preserves the uterus and may allow for further pregnancies, UAE involves blocking the artery that supplies the fibroid, leading to shrinkage and potential expulsion. This can raise significant concerns for women who wish to still conceive. Women of childbearing age have specific concerns related to fertility, pregnancy, and the preservation of their reproductive options, UAE is an intervention that can have an impact on fertility and pregnancy outcomes. Hence, it is important that women considering the UAE receive thorough counseling about the potential implications of the procedure on their reproductive health. Counseling should encompass the following topics: fertility preservation, pregnancy risk, fibroid recurrence, and alternative treatment options.
Furthermore, the article provides a significant contribution to the literature in the aspects listed below. Firstly, it systematically compares the two common treatment options myomectomy and UAE. This comparison is vital in helping clinicians and patients make informed decisions about which treatment option is suitable to pursue. This study uses a large sample size making it one of the largest meta-analyses in this field; this enhances the reliability and statistical power of the findings. The article evaluates multiple critical outcomes, including re-intervention rates, complications, and duration of hospital stay. The outcomes are of great interest to both hospital care providers and patients when considering treatment options. Furthermore, the discussion highlights research gaps, such as the need to consider factors like age, body mass index (BMI), fibroid characteristics, and menopausal status in future studies. This directs researchers toward potential areas for further investigation.
Methods
Data sources and strategies
We performed this meta-analysis following Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 11 This meta-analysis is reported following the PRISMA guidelines. The study was not registered in PROSPERO as the design and methodology were finalized before we were aware of the registration requirement; however, we will ensure that all relevant data is reported to maintain transparency. This meta-analysis only included data from previously published studies; therefore, ethical approval was deemed unnecessary.
Study selection
Two authors (FK and HWA) independently performed an electronic search of PubMed and Cochrane Central using an extensive search strategy that involved all possible abbreviations and names of leiomyomas and interventions along with MeSH Terms and Boolean operators “AND” and “OR.” The search strategy is included in Supplemental Table 1. This search strategy yielded 357 results. The timeline was kept from January 2000 till March 2022.
The inclusion criteria for our meta-analysis were (a) published randomized clinical trials (RCTs), and observational studies; (b) UAE and myomectomy as comparators (c) reported at least one of the following outcomes of re-intervention, anemia, quality of life, fertility, hospital stay, ovarian reserves, and complications. Re-intervention rates were defined as the incidence of any procedure done after the primary UAE or myomectomy on the patient. Complications included early and late post-procedural as well as minor and major complications. Major complications were defined as any life-threatening event or any intervention required to prevent permanent impairment or damage, and death. 13 Minor complications were the events that occurred after myomectomy or UAE and were labeled as such in the included studies since they did not meet the criteria for major complications. Certain outcomes were removed because the data was too complex to be pooled into Review Manager, a software for Cochrane reviews. Studies that did not include relevant outcomes were excluded. Studies with insufficient data or ongoing clinical trials, single-arm studies, case reports, case series, editorials, narrative reviews, and commentaries were excluded. Finalized outcomes included re-intervention, complications, and duration of hospital stay. Any disagreement between the two independent reviewers (FK and HWA) about the selection of studies was resolved by consultation with a senior investigator (AE).
Eventually, we shortlisted nine studies that had the same target population, that is, women with uterine leiomyomas, UAE as intervention, with myomectomy being the comparator/control group and re-intervention, duration of hospital stay, and complications as outcomes.
Data extraction and quality assessment of studies
The two independent reviewers (FK and HWA) cross-verified the studies and then manually removed duplicates. The full texts of the remaining articles were then scrutinized to extract the outcomes mentioned above and their mean difference (MD), standard deviation, and raw data. Moreover, the references in each study were also manually screened to ensure no relevant studies were missed during the electronic search. We used the Newcastle–Ottawa scale for the quality assessment of observational studies across six domains (selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias) 21 and the Cochrane Collaboration risk of bias tool for RCTs, 22 the results of which are reported in Supplemental Figures 1 and 2(a) and (b), respectively.
Summarizing PRISMA flow chart
As shown in Figure 1, our initial search yielded 357 results, after the removal of duplicates 138 studies were taken ahead for further screening. In total, 135 studies were screened out of which 103 were excluded. Thirty-two full-text articles were assessed for eligibility, of which 7 full-text articles were excluded because of reasons such as articles did not include the required outcomes, did not include UAE as an intervention, or did not compare outcomes of myomectomy with UAE. Twenty-five studies were taken for qualitative synthesis of which 9 studies were included in the meta-analysis.
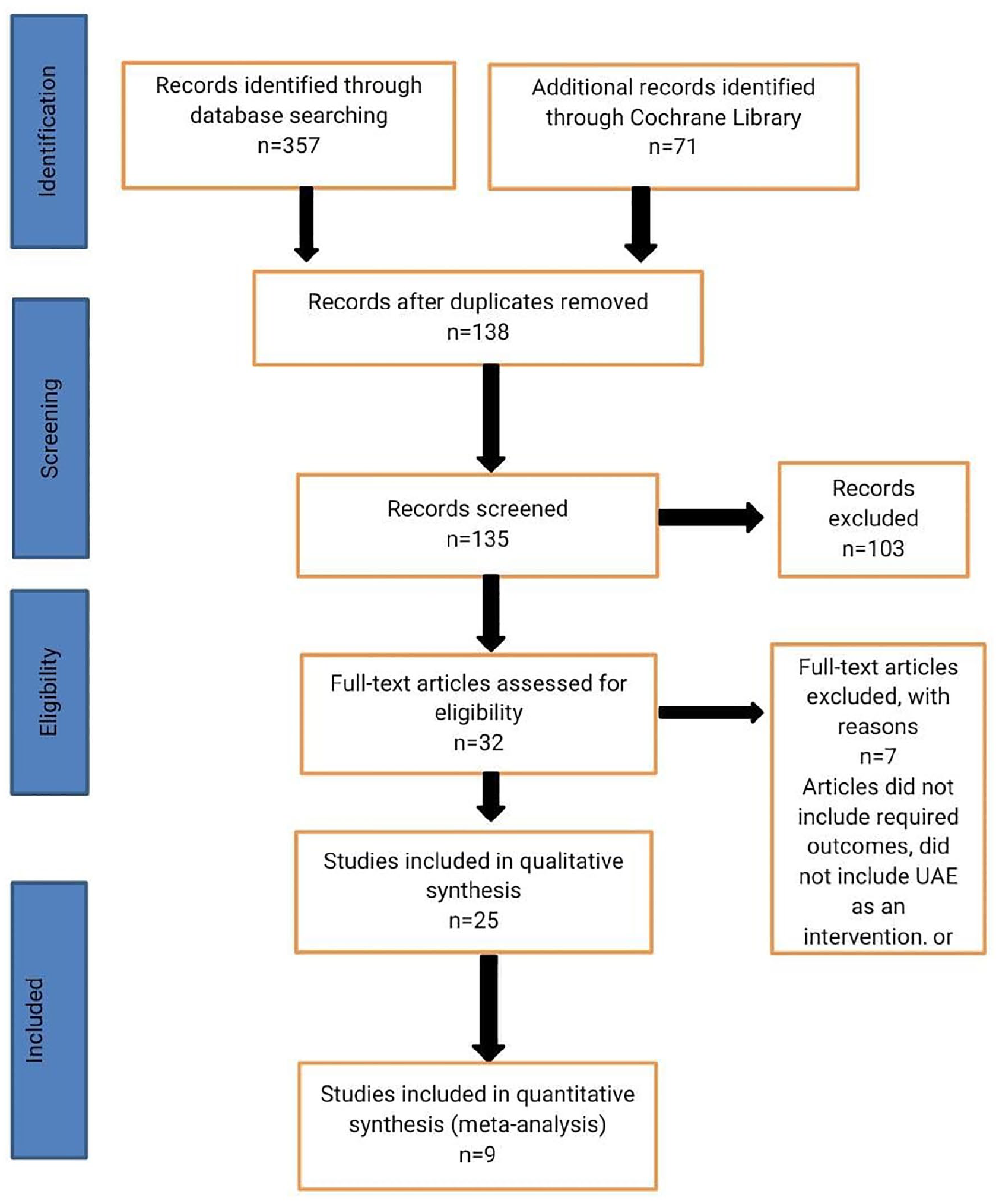
PRISMA flow diagram.
Statistical analysis
Statistical analysis was done using Review Manager version 5.4. These outcomes were then stratified into two subgroups based on study type (RCT or observational) and the Chi-square test was performed to evaluate the differences between the subgroups. In addition, heterogeneity in effect sizes was assessed using Higgin’s I2 statistics where the I2 value of greater than 50% was considered significant. For continuous outcomes, settings were adjusted to random effects as the analysis method, while for dichotomous data, settings were adjusted to risk ratio (RR) as the effect measure, and Mantel–Haenszel as the statistical method. Forest plots were generated for each outcome. p-value <0.05 was considered significant for all the analyses. 6
Results
After exclusions, nine studies (five studies were randomized control trial and four were observational studies) with approximately 196,595 patients were included in the final analysis, the characteristics of which are shown in Table 1. Some studies had different types of myomectomies performed on the patients; open, laparoscopic, laparoscopic-assisted, and hysteroscopic myomectomies. Other studies also had different abdominal incisions for myomectomy like previous abdominal incisions, and transverse suprapubic incisions.
Characteristics of included studies.

N/R, not reported; OS, observational study; QoL, quality of life; RCT, randomized controlled trial.
Table 1 shows that out of the 4 observational studies, that of Broder et al. 12 , which was conducted in the United States and Germany, reported quantitative data, and abdominal myomectomy was performed in 81 patients. The outcomes observed were re-intervention, no improvement/worsening of symptoms, clinical failure very dissatisfied with therapy. The follow-up period for Broder et al. 12 was 36 months. The study of Ohgi et al. 15 was also an observational study conducted in Japan and reported quantitative raw data. Laparoscopic myomectomy and laparoscopic-assisted myomectomy were done in 163 patients. The outcomes included nausea or vomiting, necessity for painkillers, general fatigue, continuous discharge, fever, period of hospital stay, period until resuming normal daily life, period until beginning work, period until beginning to drive a car, ride a bicycle, or exercise. The follow-up time was 6 months. Furthermore, the study of Borah, 17 done in the United States, reported data in standard deviation. It did not report any type of myomectomy performed on patients. The outcomes reported from a population of 135,522 were re-intervention, adverse reproductive outcomes, long-term adverse consequences of hysterectomy including fracture risk, pelvic organ prolapse, cardiovascular disease risk, and risk of dementia. The follow-up for this study was 5 years. Lastly, that of Davis et al., 18 conducted in the United States presented data in terms of standard deviation. Open abdominal, laparoscopic, or hysteroscopic myomectomy was performed in 35,631 patients. The outcomes included in the study were re-intervention, re-intervention rates after myomectomy, endometrial ablation, and UAE for patients with uterine fibroids. The follow-up was reported to be for 12 months.
Table 1 further displays the five randomized controlled trials, of which the first study reviewed was that of Edwards et al. 13 conducted in the United Kingdom and included a total of 157 patients on whom abdominal myomectomy was performed. It stated data in terms of standard deviations and outcomes observed were re-intervention, quality of life, pain, median hospital stays, symptom score, the median time until the patient could resume all recorded usual activities, minor complications, major adverse events, treatment failures, use of resources, pregnancy. The follow-up time was noted to be 18 months. Secondly, Mara et al. 14 reported data in terms of standard deviation from the Czech Republic including a total of 121 patients in which 42 laparoscopic and 21 open myomectomies were performed. Follow-up time was 30 months to observe the outcomes including re-intervention, quality of life, average length of hospitalization, and postoperative recovery time. In addition to this, Manyonda et al. 16 stated quantitative data which included a population of 150 patients from the United Kingdom. It reported a transverse suprapubic incision for myomectomy with a follow-up time of 5 years and the outcomes that were included were re-intervention, quality of life, short hospitalization stays (2–6 days), 1-year post-re-intervention of QoL scores for both groups (myomectomy and UAE), few major complications, higher re-intervention rate. Another study of Manyonda done in 2020, reported data in terms of standard deviation and 95% confidence interval (CI). It was done in the United Kingdom and included a total of 254 patients on whom open abdominal, laparoscopic, or hysteroscopic myomectomy was performed. The follow-up time was 2 years to report the outcomes including quality of life, pre-operative, and perioperative complications. Lastly, Wang et al., 20 stating quantitative raw data, was included which was conducted in the United States and reported outcomes, such as quality of life, hospital stay duration, and cost from a patient population of 24,516. No type of myomectomy was included in this. The follow-up time for this study was 100 days.
Outcomes
Re-intervention
As shown in Figure 2, data for re-intervention, reported by seven studies, yielded significant results, establishing that UAE was associated with a greater rate of re-intervention than myomectomy (RR: 2.16, 95% CI: (1.27–3.66), p-value 0.004, heterogeneity I2 = 85%) (p-value for subgroup differences = 0.005).

Outcome: re-intervention.
Duration of hospital stay
As shown in Figure 3, data for the duration of hospital stay was provided by three studies. UAE was associated with a shorter duration of hospital stay compared with myomectomy (MD: −1.12, 95% CI: (−2.50 to 0.27), p-value 0.11, heterogeneity I2 = 96%) (p-value for subgroup differences = 0.005); however, results were non-significant.

Outcome: hospital stay.
Major complications
As shown in Figure 4, the overall procedure’s major complications were evaluated by two studies. UAE holds a greater risk of major complications as compared to myomectomy (RR: 0.62, 95% CI: (0.29–1.33), p-value 0.22, heterogeneity I2 = 0%); however, results were reportedly non-significant.

Outcome: major complications.
Minor complications
Overall procedure minor complications were evaluated by two studies as shown in Figure 5. Myomectomy was associated with a greater risk of minor complications as compared to UAE (RR: 1.72, 95% CI: (0.92–3.22), p-value 0.09, heterogeneity I2 = 0%); however, results were reportedly non-significant.

Outcome: minor complications.
Discussion
In our meta-analysis of approximately 196,595 patients, we found significant results suggesting a positive association between UAE and re-intervention, compared with myomectomy. Pooled results for procedural complications and duration of hospital stay were reportedly non-significant.
In the prior meta-analyses, Borah et al. 17 and Davis et al. 18 assessed re-intervention rates and demonstrated a higher observed rate of re-intervention in UAE patients compared with myomectomy patients as shown by the findings of our meta-analysis. Manyonda et al. 16 reported a higher incidence of major complications, such as pulmonary embolism, ileus, pneumonia, hemorrhage, repeat laparotomy, Escherichia coli sepsis, small bowel obstruction, laparotomy, and adhesiolysis within the myomectomy group, with a rate of 8%, as compared to a lower rate of major complications (2.9%) such as pelvic sepsis requiring IV antibiotics, fibroid expulsion, and extraction in the UAE group at the 1-year follow-up. Additionally, their study revealed a greater occurrence of minor complications (13.2%) in the UAE group, including post-embolization syndrome, groin hematoma, and urticaria due to contrast. In comparison, the myomectomy group had a lower rate of minor complications (10.9%), such as urinary tract infections. Similarly, Edwards et al. 13 observed a higher rate of major complications in the myomectomy group and a higher rate of minor complications in the UAE group. In contrast, our study found an elevated risk of major complications associated with UAE and minor complications associated with myomectomy. This may be due to a difference in the population size, or the duration of follow-up therefore Edwards et al. 13 having a follow-up of 18 months and Mayonda et al. 16 having a follow-up of 5 years, when pooled together may generate a different result.
Consistent with previous studies by Wang et al., 20 Ohgi et al., 15 and Manyonda et al., 19 we found a shorter duration of hospital stay among women undergoing UAE.
Despite multiple studies stating that UAE is an efficacious minimally invasive treatment for uterine myomas, it’s still not utilized to the same degree as hysterectomy due to the lack of awareness of the long-term advantages of UAE as compared with hysterectomy or myomectomy. 20 Furthermore, in UAE the uterus is conserved and there is no need for general anesthesia for patients along with low rates of major complications. 20 Though the results were non-significant, our study demonstrated a numerically shorter hospital stay in UAE and longer in myomectomy which might slow down a patient’s recovery rate. Spending more time in the hospital increases their exposure to many hospital-acquired infections and complications. A study concluded that those patients having longer hospital stays experienced these complications more than the patients who did not. 20 In addition to this, longer hospital stays affect the efficacy of hospital care by increasing the cost. Re-intervention rate is a very significant element that patients and doctors take into consideration while selecting the treatment option. 18 Therefore, due to a higher rate of re-intervention associated with UAE, doctors should consider the treatment approach with caution. In the future, studies should assess the effect of obesity on the outcomes of UAE and myomectomy. Moreover, factors including nulliparity, women undergoing menopause, lifestyle (diet, caffeine, alcohol, smoking, physical activity), and genetic predisposition should also be considered.
The results of our study were found to be highly heterogeneous with duration of hospital stay and re-intervention reporting heterogeneity of greater than 50%. We performed subgroup analysis according to the type of study design for re-intervention rate and duration of hospital stay and found that heterogeneity was primarily associated with the inclusion of observational studies, including prospective and retrospective cohort studies. We should also keep in mind differences in the definition of complications and the length of time the complications were recorded. Other causes of heterogeneity may be the difference in characteristics such as age, BMI, and more importantly the number and location of the uterine fibroids which are not quoted by all the studies.
Our study had certain limitations. The rate of failure and development of complications in certain individuals undergoing UAE might be higher because of unfavorable anatomies like the difference in anastomoses to the ovarian artery and the number of uterine arteries present. Only a limited number of previous studies have made a clear differentiation between major and minor complications within both the UAE and myomectomy groups. This distinction holds significant value for clinicians and patients who rely on the literature because merely lumping all complications together and providing a single complication rate is not suitable. It is important to recognize that not all complications carry the same weight, so it is more meaningful to categorize them as major or minor.
We recognize that many factors, such as age, BMI, fibroid location, number of fibroids, and menopausal status, can affect outcomes like re-intervention. However, further sub-analysis of this factor was not possible due to the lack of relevant information in the user studies. Another limitation of our study is that enough articles could not be quoted for certain outcomes like quality of life, due to a lack of papers that met our selection criteria. There is also a lack of data on outcomes such as ovarian reserves, follicle-stimulating hormone levels, uterine volumes, etc. which prevents our study from making serious gynecological implications.
Conclusion
In summary, after conducting an extensive meta-analysis involving a substantial sample size of approximately 196,595 patients, our findings indicate that myomectomy proved to be the superior treatment option when compared to UAE for addressing uterine fibroids. Specifically, the key takeaway from our analysis is the substantial reduction in re-intervention rates associated with myomectomy, underlining its efficacy and appropriateness as the primary choice of treatment for this condition.
However, it is important to acknowledge that the comparison between UAE and myomectomy yielded less definitive results when it came to assessing potential complications and the duration of hospital stays. These particular aspects of the treatments remain inconclusive in our analysis, signifying that more research may be needed to ascertain the comparative advantages or disadvantages in these areas.
In light of these findings, it becomes evident that the medical community should continue to carefully weigh the pros and cons of each treatment method, taking into consideration not only re-intervention rates but also potential complications and hospitalization durations when making informed decisions about the most appropriate approach to managing uterine fibroids.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241236141 – Supplemental material for Uterine artery embolization versus myomectomy: a systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121241236141 for Uterine artery embolization versus myomectomy: a systematic review and meta-analysis by Kaneez Fatima, Haya Waseem Ansari, Arooba Ejaz, Furqanullah Khalid, Aimen Naz, Ayesha Waqar, Adeela Sarfaraz Khan, Sana Godil, Muhammad Zain Ayub, Muhammad Azaan Tariq, Yumna Salman and Hassaan Ahmed Shah in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241236141 – Supplemental material for Uterine artery embolization versus myomectomy: a systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121241236141 for Uterine artery embolization versus myomectomy: a systematic review and meta-analysis by Kaneez Fatima, Haya Waseem Ansari, Arooba Ejaz, Furqanullah Khalid, Aimen Naz, Ayesha Waqar, Adeela Sarfaraz Khan, Sana Godil, Muhammad Zain Ayub, Muhammad Azaan Tariq, Yumna Salman and Hassaan Ahmed Shah in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge Dr Shariq Usman for proofreading activity. The authors would like to acknowledge the Research Council of Pakistan (RCOP) for their support along all aspects of conducting this study.
Author contributions
KF and AE have given substantial contributions to the conception or the design of the article, and HWA, FK, and AN to the acquisition, analysis, and interpretation of the data. All authors have participated in drafting the article, and AE revised it critically. All authors read and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.