
Abstract
This review explores the classification and evaluation of suspicious renal lesions across several radiologic imaging modalities. Diagnostic medical sonography (DMS), computed tomography (CT), magnetic resonance imaging (MRI), and contrast-enhanced ultrasound (CEUS) are the primary modalities used to investigate questionable lesions found within the kidneys. Renal masses may range from completely benign to malignant. They are classified based on many different features and characteristics. These lesions may be simple cystic, complex cystic, or solid in nature. Masses may also exhibit varying degrees of vascularity, septations, and calcifications. The discussed imaging modalities have varying strengths, limitations, and implications for use. Imaging techniques may be used independently or in conjunction to best diagnose and treat a patient with a suspicious renal mass. The aim of this review was to describe the diagnostic value of the imaging modalities (DMS, CT, MRI, and CEUS) and their role in the evaluation of suspicious renal lesions.
A patient presenting with an indeterminate renal mass requires further intervention to ensure the best outcome for the patient, including appropriate care and follow-up. Lesions of the kidney are a common pathological finding in medical imaging practice. Most of these lesions are incidental findings discovered while patients are being imaged for other medical reasons. Imaging modalities used to investigate these renal lesions include diagnostic medical sonography (DMS), computed tomography (CT), magnetic resonance imaging (MRI), and contrast-enhanced ultrasonography (CEUS). Each modality has differing strengths, limitations, and benefits for use in imaging the kidneys. Most renal lesions are simple cortical cysts and do not require additional investigation; however, some often require further inquiry and either continued follow-up or treatment. Renal lesions may range from completely benign to malignant neoplasms. Both benign and malignant masses may be either cystic or solid in nature, so careful, thorough investigation is extremely important. The main goal of these imaging modalities is to produce the best outcome for patients by correctly characterizing these lesions to make a confident, accurate diagnosis and treatment plan.
American College of Radiology Appropriateness Criteria
An indeterminate renal lesion is one that cannot be definitively diagnosed as either benign or malignant at the time of discovery. The American College of Radiology (ACR) Appropriateness Criteria are a set of guidelines that are evidence based and reviewed every 3 years by an expert panel that reviews the current literature to rate the appropriateness of medical imaging and intervention techniques. 1 These guidelines rate imaging methods on a scale between 1 and 9, with 1 to 3 considered usually inappropriate techniques, 4 to 6 possibly appropriate techniques, and 7 to 9 as usually appropriate imaging techniques. 1 For patients with normal renal function, these guidelines rated DMS as an 8. 1 MRI abdomen with and without contrast was also ranked as an 8. 1 CT abdomen with and without contrast was ranked the highest at a 9. 1 For patients with renal insufficiency and other contraindications to intravenous contrast, DMS was ranked the highest at an 8. 1 MRI abdomen without contrast was rated 7, renal biopsy was rated 6, and a CT abdomen without contrast was rated 5. 1
According to these guidelines, CT was rated the highest, closely followed by MRI and DMS for patients with normal kidney function. In patients with impaired renal function or other contraindications for intravenous (IV) contrast, DMS was rated the best imaging modality for interrogation of indeterminate renal lesions. It is important to note that these guidelines were last published in 2015, and therefore their literature review was most likely performed in 2014. This review provides published information that is more recent, from 2016 to 2018. New published evidence has the potential to influence a reranking of these imaging modality choices.
Incidence
The discovery of lesions within the kidney is not uncommon, and most are incidentally found while imaging for other medical indications. Pathologic discoveries are common across all imaging modalities. Renal pathologies can be found incidentally in approximately 13% to 27% of all patients using radiologic imaging techniques. 2 Renal anomalies are more common in the male population, with a ratio of 2:1 over females. 2 Also, the age of the patient positively correlates with the incidence of lesion formation. Renal lesions are discovered in about 20% of patients who are 50 years of age or older and in 50% of all postmortem autopsies. 2 In most of these patients, these masses are benign, simple cysts. The most common renal abnormality is the simple cyst. Simple cysts have an estimated incidence of 50% in individuals older than age 50 years and an incidence of 60% in those older than age 60 years. 3 The formation of simple cysts is a normal part of the aging process. When a lesion features characteristics other than a simple cyst, the finding requires further evaluation.
Renal Cell Carcinoma
The most serious pathological finding of the kidney is renal cell carcinoma (RCC). RCC is the most common primary neoplasm of the kidneys and most commonly occurs in males over 50 years of age. This cancer shows an incidence rate of 3% of all malignant neoplasms and is one of the most common tumors of the urinary tract system. 4 RCC is often asymptomatic and an incidental discovery during imaging. Approximately 6% of all kidney lesions that do not present with clinical signs or symptoms are cystic RCCs. 4 Treatment for RCC may include full or partial nephrectomy. Appropriate workup of suspicious renal lesions is very important to rule out this very serious and detrimental pathologic process.
Classification
Simple cysts typically do not require further inquiry or treatment, as these are typically benign. However, when renal lesions are solid or complicated by debris, infection, calcifications, or hemorrhage, these require closer evaluation. Complicated cysts must be further examined for the possibility that they are forms of cystic malignancy.
Cystic renal lesions may range from simple, complex, infectious cystic renal disease to multifocal cystic renal disease. Cystic renal diseases may be categorized as focal, multifocal, or infectious. Examples of cystic renal tumors include cystic RCC, multilocular cystic nephroma, and mixed epithelial and stromal tumors (MESTs). 3 Multifocal cystic renal lesions are classified as either acquired or heritable. Acquired cysts include cystic kidney disease, lithium-induced nephrotoxicity, glomerulocystic kidney disease, multicystic dysplastic kidney, and localized cystic renal disease. 5 Heritable diseases include tuberous sclerosis, von Hippel-Lindau disease, and autosomal dominant polycystic kidney disease. 5
Finally, renal lesions may be solid in nature. These are most worrisome for malignancy. It is crucial for a radiologist to be able to distinguish between these varied types of kidney lesions to make the most accurate diagnosis for the patient.
Bosniak Classification System
Globally, radiologists and urologists using the Bosniak system to classify cystic renal lesions. The system was first described in 1986 and has continued to be modified and updated through the years. 6 The Bosniak classification system is useful for categorizing but does not place great emphasis on underlying pathophysiology. 6 The system is based on CT findings and has now been adopted to other imaging modalities.
The features of a cystic mass can place it into one of five categories (I, II, IIF, III, and IV). Categories I and II are simple to mildly complicated. They are benign, requiring no additional follow-up. 6 Category IIF cysts are moderately complex and require follow-up imaging to prove benignity. 6 Category III lesions have more suspicious features such as thickened septa or walls with associated enhancement. 6 Classification of lesions between categories IIF and III can be difficult, requiring thorough investigation, and can vary by institution. 6 Category IV lesions are easier to diagnosis because they are usually an obvious cystic neoplasm and require surgical intervention. 6 The Bosniak system does not consider size in the likelihood for malignancy. However, typically, the smaller the lesion, the increased likelihood that the lesion is benign. 6
Imaging Modalities
Diagnostic Medical Sonography
DMS is a commonly used imaging modality for the evaluation of the kidneys. With DMS, renal cysts appear as well circumscribed, fluid-filled, anechoic, rounded structures. Basic gray-scale DMS is an excellent screening method to detect renal lesions and helpful to triage renal lesions that will require further investigation with other modalities. Gray-scale DMS is the most common initial imaging modality used for the classification of renal lesions. It is sufficient in distinguishing between solid and cystic structures and very useful in distinguishing simple cysts from more complex or solid lesions. DMS is helpful in distinguishing cysts from hypovascular solid tumors seen on CT. 7 DMS also shows septations better in complex lesions as opposed to CT.
The use of color Doppler (CD) and power Doppler (PD) provides important information on perfusion. 8 CD and PD modes are used to evaluate vascularity within normal anatomy and pathology. Increased vascularity within renal lesions is more indicative of malignancy.
There are strengths and weaknesses associated with DMS. Strengths of this modality include that it is widely available, noninvasive, and cost-effective for the patient and lacks contrast agent and radiation exposure. DMS is frequently used for screenings, abdominal surveys, and long-term follow-up evaluation. Despite its strengths, DMS alone is often not capable of fully characterizing complex and solid renal masses. More questionable lesions require further interrogation through the use of other modalities. DMS may be less sensitive than CT and MRI. Solid and cystic tumors found using DMS often require further evaluation using either CT or MRI. Gray-scale DMS is the imaging method of choice for the diagnosis of simple cysts (Bosniak I) (Figure 1) and minimally complicated cysts (Bosniak II). 4 However, Bosniak IIF to IV lesions are most commonly evaluated using a contrast-enhanced (CE)–CT or MRI approach. 4
Bosniak I cyst that is depicted with contrast-enhanced ultrasound.
Computed Tomography
CT is an extremely common imaging modality used to investigate renal lesions. CT is considered the first-line imaging technique in characterizing renal masses, while CE-CT is recommended for a more detailed investigation of unclear lesions. On CT, simple renal cysts present as homogeneous in appearance, have simple fluid attenuation of less than 20 HU, feature hairline thin smooth walls or an imperceptible wall, and have no enhancement following contrast administration. 9 When a mass has a mean attenuation value greater than 20 HU on unenhanced or CE-CT, it does not meet the criteria to be diagnosed as a benign simple cyst. 9
CE-CT is commonly used to evaluate Bosniak IIF to IV renal lesions 2 (Figures 2 and 3). Multidetector CT (MDCT) is the preferred technique because of low cost, wide availability, shorter acquisition time, and excellent spatial resolution. 10 Dual-energy CT (DECT) has been found useful for discerning between benign and solid cystic lesions over 1.5 cm in size, presenting as hyperdense on single-phase postcontrast CT. 11 Newly emerging, computed tomography perfusion (CTp) is an examination that allows a quantitative evaluation of tissue perfusion through consecutive scans acquired while contrast media are injected. 12 This technique shows promising, improved results in the characterization of renal lesions. 12
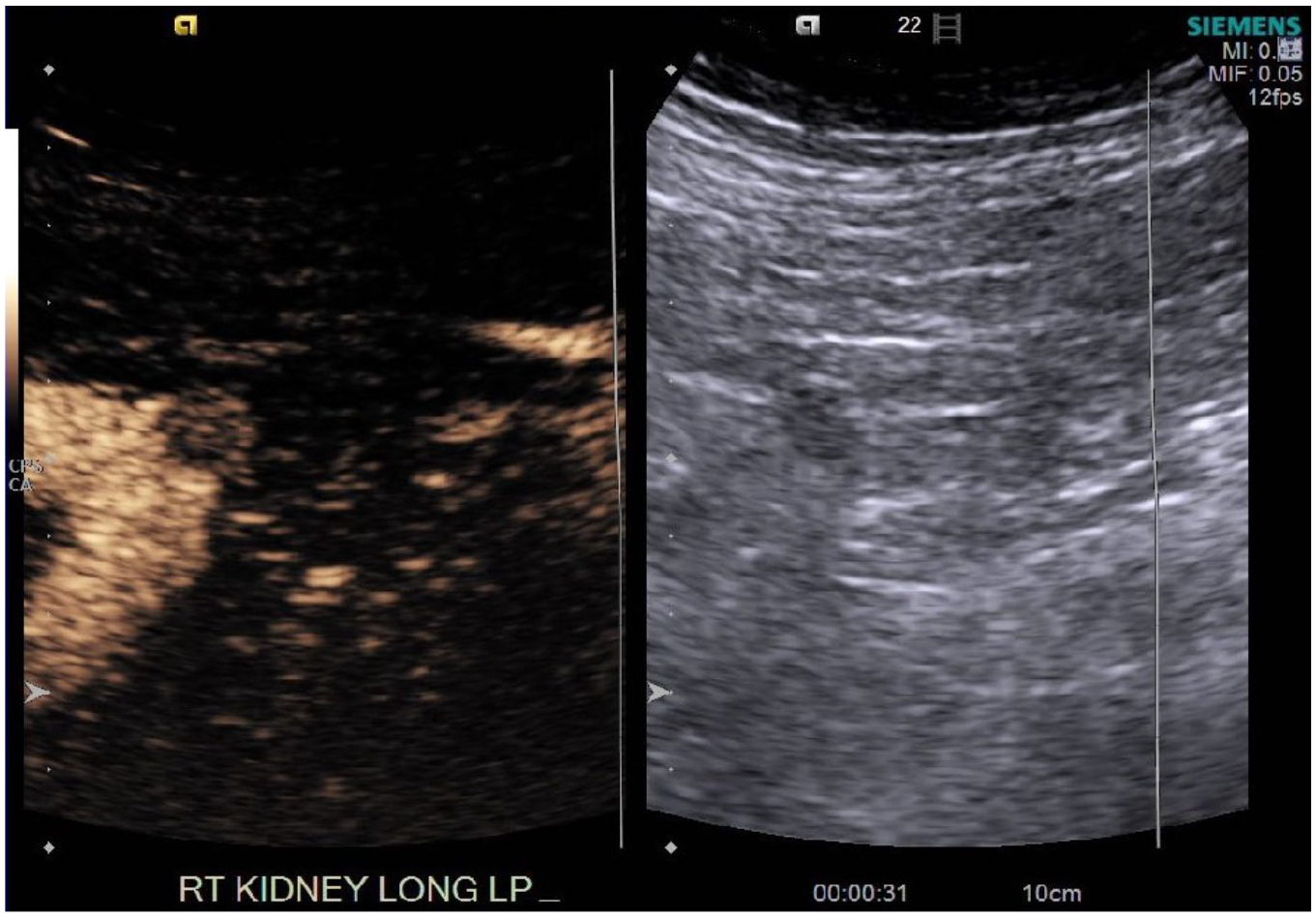
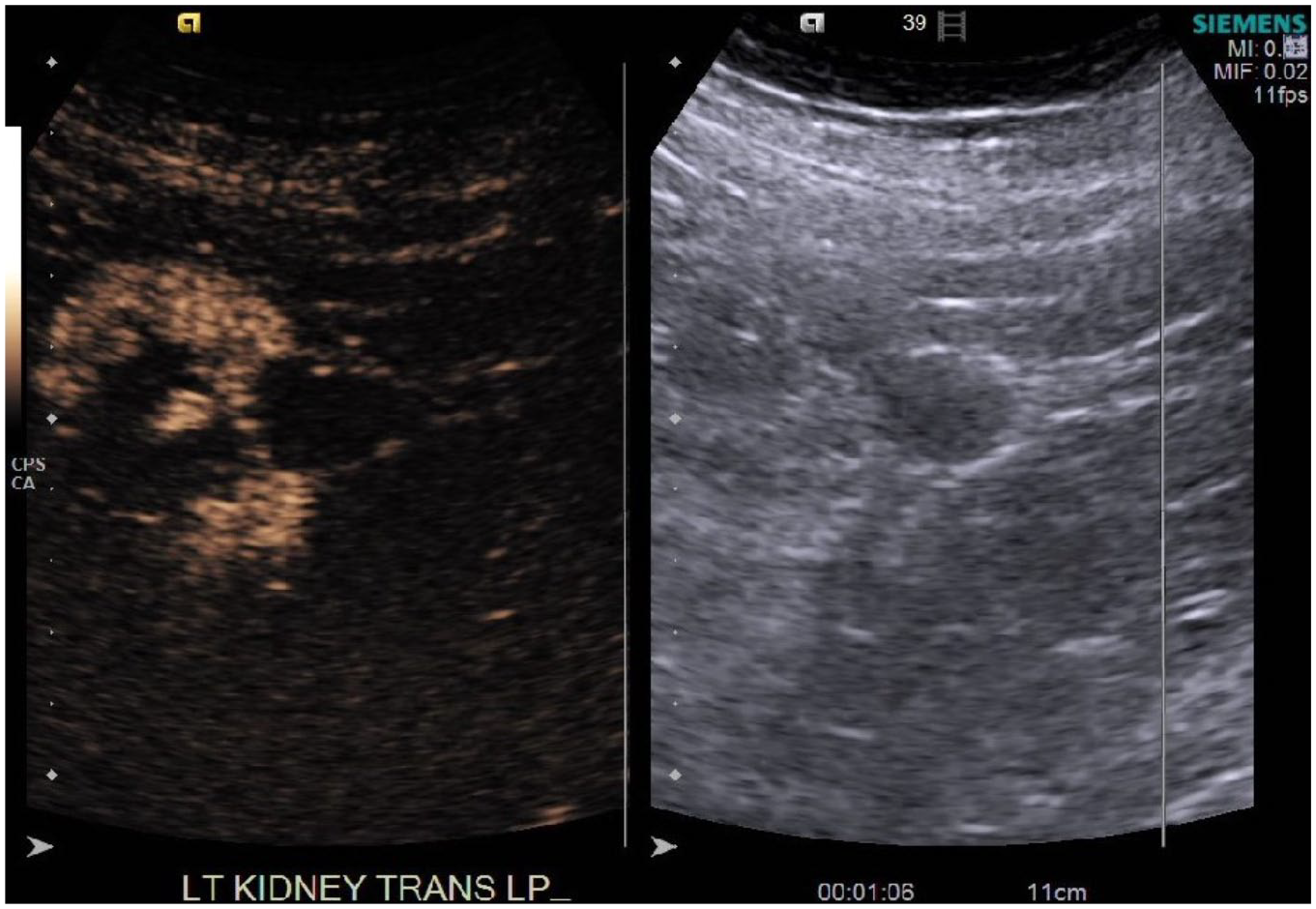
Right renal lower pole mass captured with contrast-enhanced ultrasound that could represent renal cell carcinoma.
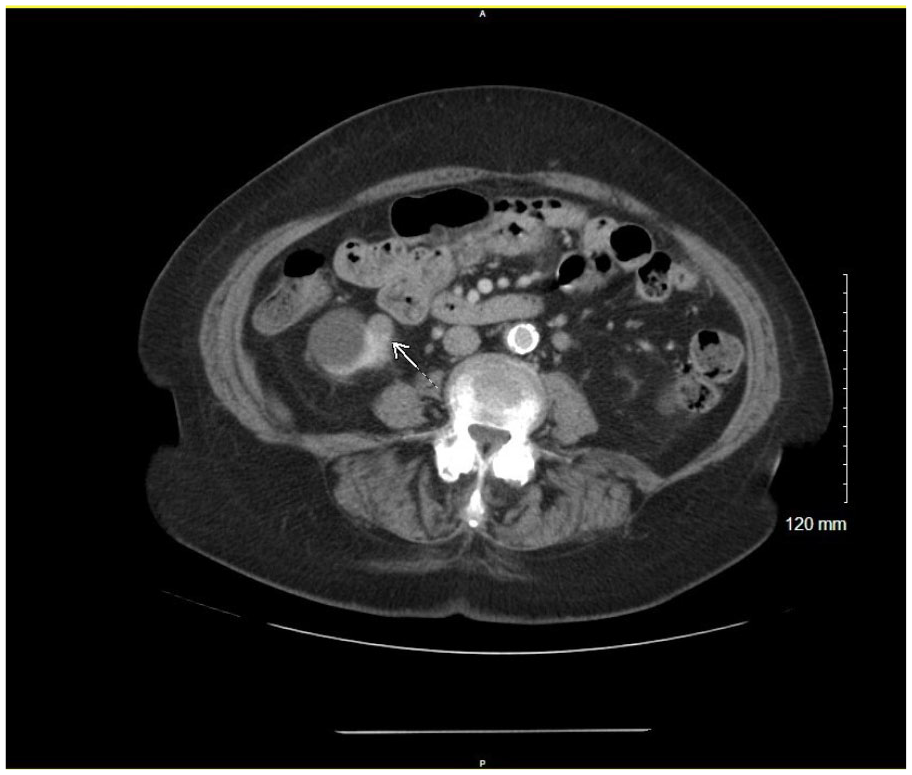
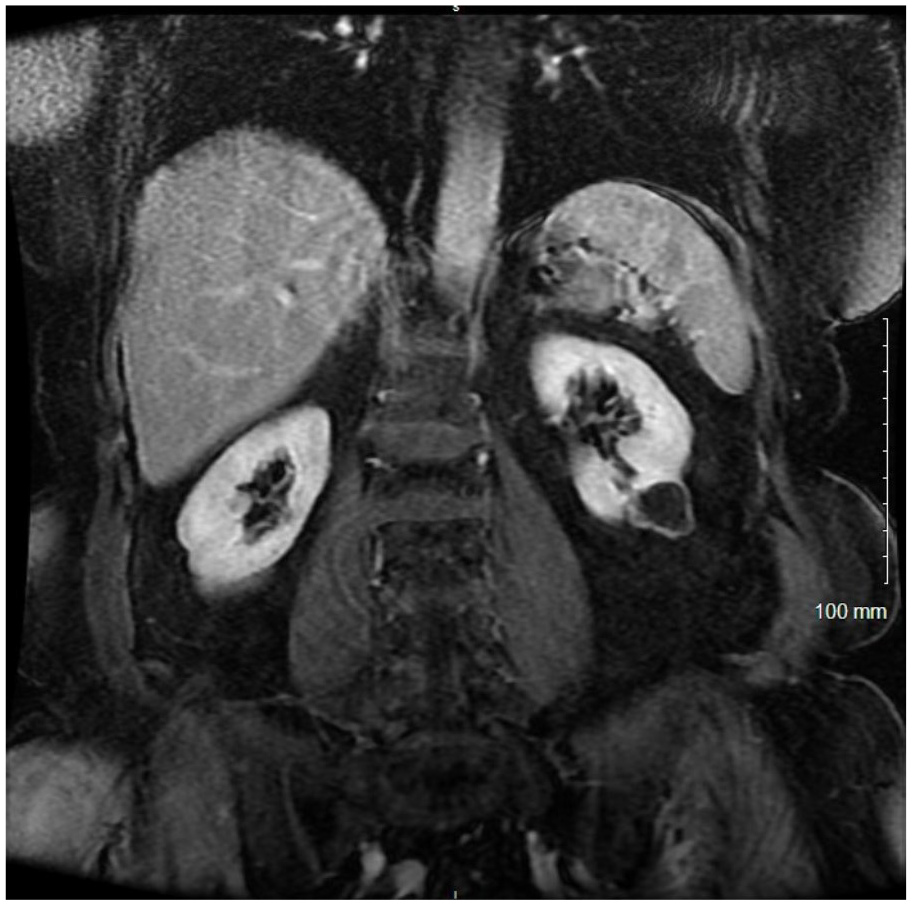
The same right renal lower pole renal mass on contrast-enhanced computed tomography.
There are strengths and weaknesses to this imaging modality. CT is more detailed and sensitive than sonography for evaluation of masses. It is often sufficient in the characterization of questionable renal lesions; however, it has a higher cost than the sonographic approach and does expose the patient to ionizing radiation. Also, CE-CT is not safe for patients with renal insufficiency. Most patients presenting with questionable renal lesions also experience renal insufficiency, hindering CT from being the imaging choice for interrogating these patients.
Magnetic Resonance Imaging
MRI is a very helpful imaging modality in the characterization of questionable renal lesions. This imaging technique offers the best soft tissue contrast resolution with excellent demonstration of contrast enhancement. 10 MRI offers high contrast resolution, shows detailed characteristics of soft tissues, and provides triplanar images. 13 It is very useful for those who are not candidates for CT, such as in patients with an allergy to iodine or who are pregnant.
MRI is commonly used to evaluate Bosniak IIF to IV renal lesions 4 (Figures 4–6). It is useful for renal masses with borderline enhancement on CT. 7 This modality is an effective technique for characterizing renal lesions deemed too small to characterize by CT. 14 Subcentimeter, hypodense renal lesions are difficult to categorize on CT alone because they are susceptible to volume averaging and pseudoenhancement. 14 MRI is considered effective in characterizing lesions as small as 15 mm. 14
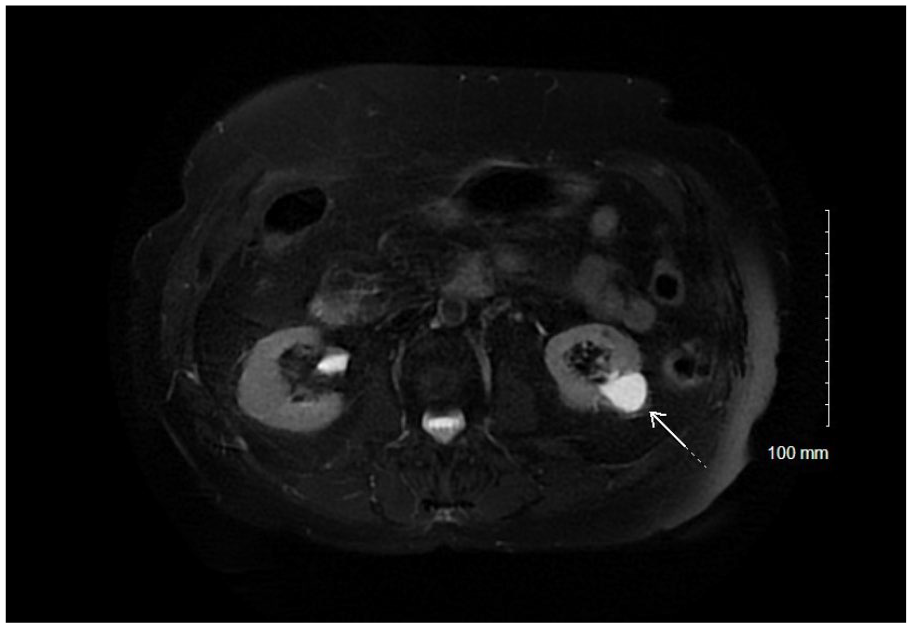
Bosniak III cystic mass on lower pole of left kidney, on magnetic resonance imaging without contrast media.
The same renal mass imaged with magnetic resonance imaging and contrast media.
The same lower pole renal lesion demonstrated with contrast-enhanced ultrasound.
Diffusion-weighted imaging (DWI) MRI can be an effective method for distinguishing between benign and malignant renal lesions of solid or cystic nature. 13 DWI is a fast, noninvasive method that does not use a contrast agent. This technique is based on the movement of water molecules across tissues. DWI and the apparent diffusion coefficient (ADC) may provide additional diagnostic information compared with that obtained by conventional MRI alone. 13 The role of DWI MRI as a biomarker for the investigation of benign or malignant renal masses, subtypes of RCC, and histological grades is under evaluation. 7
There are several strengths and limitations to the use of MRI. MRI can be effective in the characterization of renal lesions when DMS and CT imaging methods are not sufficient. It is more effective than other modalities at visualizing soft tissue structures and characterizing very small lesions. MRI offers excellent imaging for the patient without ionizing radiation and is therefore safe for pregnant patients. A limitation is that MRI is very expensive for patients.
Contrast-Enhanced Ultrasound
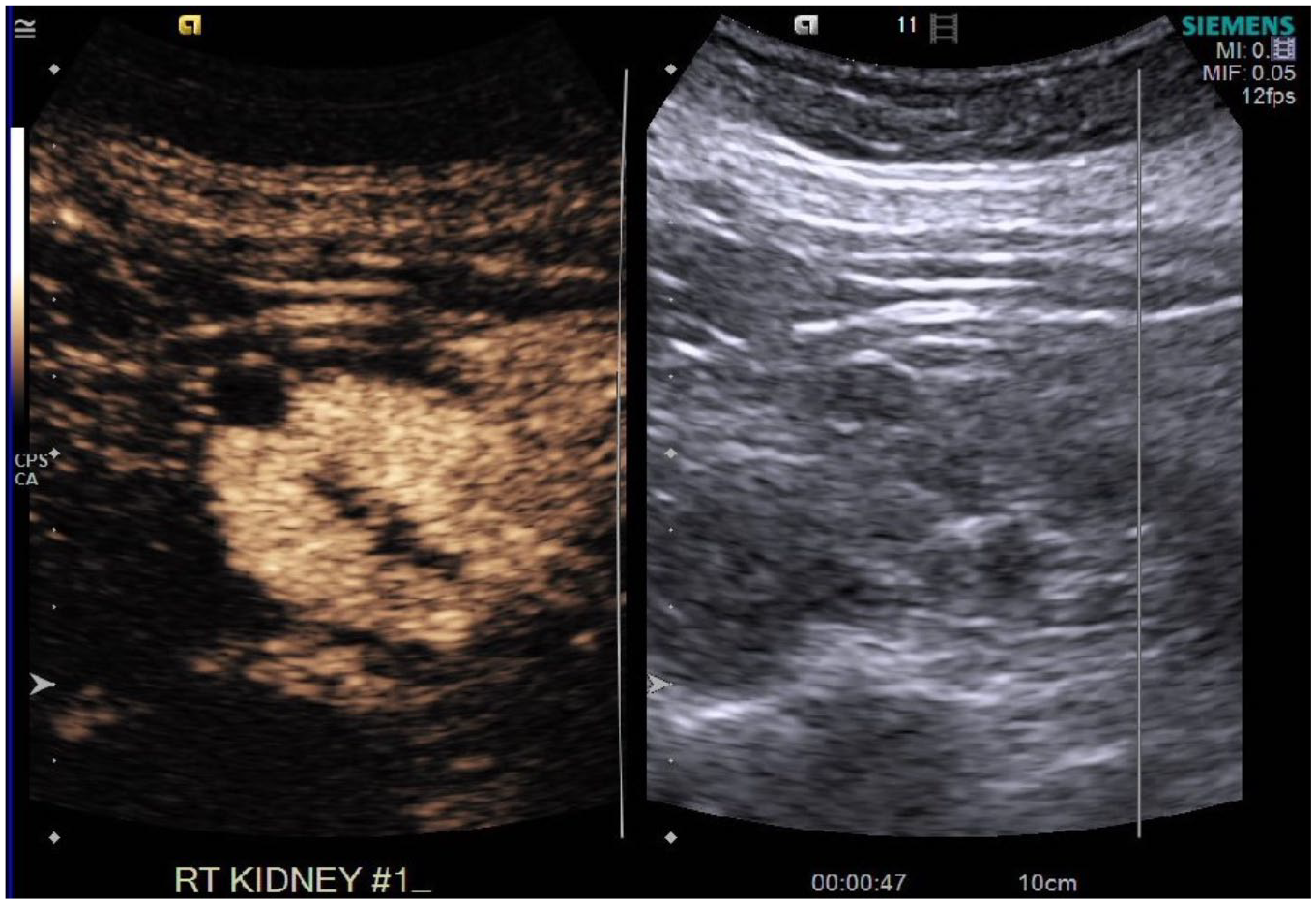
The use of CEUS was first explored in the diagnosis of suspicious liver lesions. However, this technique is now being used in the evaluation of questionable masses of the kidney. CEUS offers the combination of real-time examinations with intravenously injected contrast agents for more in-depth investigation of suspicious masses. Contrast media are gas-filled microbubbles that are injected intravenously into the patient’s systemic circulation. Once administered, the enhancement pattern of the lesion is observed and compared to that of the surrounding kidney parenchyma. Vascular and solid structures will enhance (Figure 7), while cystic structures remain anechoic. This technique is considered safe across all age groups and is especially beneficial for those patients where the use of other imaging modalities is contraindicated.
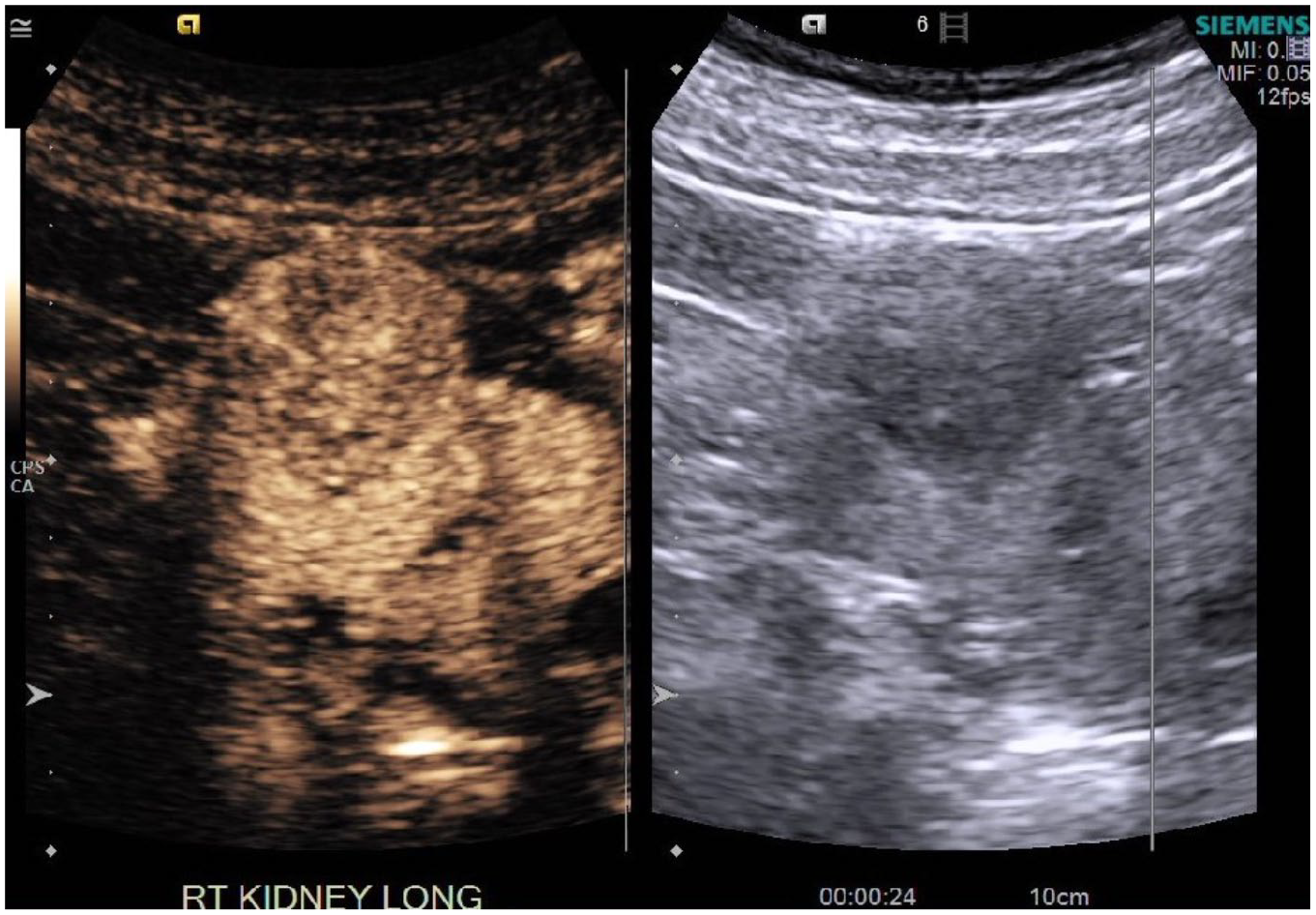
Solid enhancing mass in upper pole of right kidney concerning for renal cell carcinoma.
CEUS is especially beneficial for the evaluation of renal masses in younger patients, patients with impaired kidney function, and patients in whom CE-CT and MRI are contraindicated. Patients with chronic renal failure with impaired kidney function, hyperthyroidism, or known allergic reactions to iodine or gadolinium are not suitable candidates for CE-CT or MRI studies. Also, patients with metal implants are not able to be examined by MRI. 4 CEUS is the best alternative for investigation in patients with any of these contraindications.
CEUS contrast agents differ from those containing iodine or gadolinium used in CT and MRI. Ultrasound contrast agents are purely intravascular and do not diffuse into the interstitial space in the abdominal cavity. 4 They can also be used independently from thyroid and renal function. 4 CEUS is safe in its ability to allow multiple contrast administrations to fully evaluate questionable lesions. CEUS contrast agents are associated with a very low incidence of adverse events. CEUS studies have shown to have only 1 in 10,000 incidents of anaphylactic reaction to contrast agents. 4 For these reasons, CEUS is safer for patients with a compromised renal system or allergies to other contrast agents.
There are several other benefits to using CEUS. CEUS is much more cost-effective than MRI. CEUS is also a nonionizing radiation technique, unlike CT imaging. CEUS is useful for renal masses with borderline enhancement on CT. 7 CEUS is beneficial even in the evaluation of renal malignancy. The modality is an increasingly popular test used for imaging and staging RCC because it is low risk, efficient, and cost-effective. Malignant lesions show a different enhancement pattern than benign structures or that of normal surrounding tissues. CEUS has shown potential to classify renal masses into either “nonsurgical” or “surgical” categories for urological follow-up. 15 CEUS has shown promising results in differentiating benign lesions such as angiomyolipomas, oncocytomas, and malignant subtypes of RCC. 7 This technique has also often been used for further investigation of unclear MRI renal lesions. CEUS could reduce the amount of CT examinations and associated radiation and contrast exposure, as well as the high costs associated with an MRI approach. 2
A limitation of CEUS is that certain types of benign lesions may produce a very similar enhancement pattern to that of malignant lesions. For example, benign oncocytomas are mostly undifferentiated from malignant lesions using CEUS. 2 Also, despite the benefits to this modality, CEUS may not provide a definitive diagnosis, and therefore patients may still require further evaluation with CE-CT or MRI investigation.
Combined Imaging Modalities
Evaluation of a suspicious renal lesion with one imaging modality alone may not be sufficient in the diagnosis and care of a patient. The primary imaging modality that a lesion is discovered with may not always be the best to accurately characterize it. For example, a lesion discovered on DMS may require a more thorough investigation through CE-CT, MRI, or CEUS. Once a lesion is properly diagnosed by one modality, another may be recommended for follow-up.
In recent years, technological improvements have increased spatial, temporal, and contrast resolution of all of these imaging modalities, allowing for higher detection and more detailed evaluation of questionable renal lesions. 16 DMS is a great screening technique, helpful in determining cystic versus solid features, and often effective for follow-up imaging. It is also completely safe and cost-effective. However, DMS is less sensitive than MRI or CT. While MRI is superior in imaging capability, it is the least cost-effective approach for patients. CT is also excellent in imaging renal lesions but involves contrast and radiation exposure for the patient. CEUS is a great alternative to CE-CT and MRI for young patients and for those with impaired renal function, hypothyroidism, or known contrast media allergic reactions (e.g., iodine or gadolinium).
Physicians must consider all of the benefits and limitations of each technique to recommend the best imaging modality for their patients. While a lesion may be initially discovered on one imaging modality, a different technique may be recommended for further evaluation. This allows for a more definitive diagnosis and could be a more cost-effective and safe method that can be recommended for continued follow-up imaging.
Conclusion
Renal lesions are an extremely common pathologic finding in patients. Most of these lesions are discovered incidentally; however, they still require further investigation to determine whether they exhibit benign or malignant features. Radiologic imaging modalities, specifically DMS, CT, MRI, and CEUS, are used in the investigation of these questionable masses of the kidneys. Each technique features its own level of expertise and limitation for interrogating these lesions. CT and MRI are very accurate and thorough in detailed characterization of these masses, while CEUS is a new and effective method for patients in whom other imaging modalities are contraindicated. DMS is a great tool for initial screening and continued follow-up of findings. It is crucial for a physician to choose the best modality for thorough investigation of renal pathology. It is not uncommon for a patient to navigate multiple routes of imaging to completely and accurately characterize, diagnose, and treat these questionable renal lesions.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.