
Abstract
Patients are frequently referred for pelvic sonograms to evaluate for adnexal masses. Determining the etiology of the adnexal mass can be challenging, but is necessary to establish a follow-up strategy and correct diagnosis. It is particularly important in those cases when adnexal lesions appear to be complex and the ovaries are not visualized sonographically. Perineural cysts were found incidentally by Tarlov in 1938 during autopsy. This report documents a lesion now bearing his name, Tarlov cysts (TCs). They are defined as cerebrospinal fluid–filled saccular lesions located in the extradural space of the sacral spinal canal and are formed within the nerve root sheath at the dorsal root ganglion. The perineurium and neural tissue make up the cysts’ walls. Usually asymptomatic, a TC is mostly found on magnetic resonance imaging (MRI) of the lumbar spine and sacrum. Occasionally, a TC mimics an adnexal cyst.
Adnexa uteri or adnexa include the ovaries, uterine tubes, and uterine ligaments. Most adnexal masses arise from the ovary, but diagnostic errors occur when that is assumed rather than proved. Adequate characterization of an adnexal mass is important to determine which patients need surgery or other treatment. 1
In 1938, an American neurosurgeon, Isadore M. Tarlov, published an article in the Archives of Neurology and Psychiatry about five cases of cysts on the extradural portions of the posterior sacral or coccygeal nerve roots that he had encountered at autopsies. 2 Those cysts developed in the space between the endoneural and the perineural sheath (perineural space). According to Tarlov, it is likely that the cysts develop because of inflammation in the sheath of the nerve roots followed by enloculation of fluid in the perineural space. The clinical significance of these cysts was unclear. Now named after him, Tarlov cysts (TCs) are uncommon. In females, they can appear as adnexal masses on sonographic examinations. The TCs may be unilocular or multilocular, and it may be difficult to determine their exact location and extension sonographically, especially by transvaginal sonography. Continuity of the lesion with the sacral area is a key imaging finding, which confirms its extraperitoneal origin, therefore excluding a cystic ovarian lesion. Magnetic resonance imaging (MRI) is the best modality for the confirmation of such lesions. 3
Case Presentation
Transabdominal and transvaginal pelvic sonography was performed on a postmenopausal woman in her late 50s (gravida 5, para 0). She complained of pelvic pain and had a history of uterine leiomyomas; she was not on hormone replacement therapy or tamoxifen. Sonography was done using a GE-Logiq 9 scanner (GE Healthcare Ultrasound, Waukesha, Wisconsin) using a curvilinear 4.0-MHz and an endocavity 8.0-MHz transducer. The protocol followed included sagittal and transverse scanning of the uterus, endometrium, ovaries, and the adjacent structures using B-mode and color Doppler imaging.
Sonography identified multiple uterine intramural and subserosal leiomyomas, ranging from 1 to 6 cm in diameter. The endometrium was partially seen—secondary to the uterine heterogeneity— and measured focally 0.9 cm in maximal thickness (Figure 1). Neither ovary was detected. The right adnexa had a hypoechoic 2.9 × 1.9 × 2.4 cm complex cyst. According to a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group publication, 4 the cyst appeared to be unilocular, the internal wall of the cyst was irregular, and the cystic content appeared to have numerous internal thread-like structures (possible fibrin strands, septa, or debris); there was no posterior acoustic shadow and no appreciable Doppler flow noted (Figures 2–4).
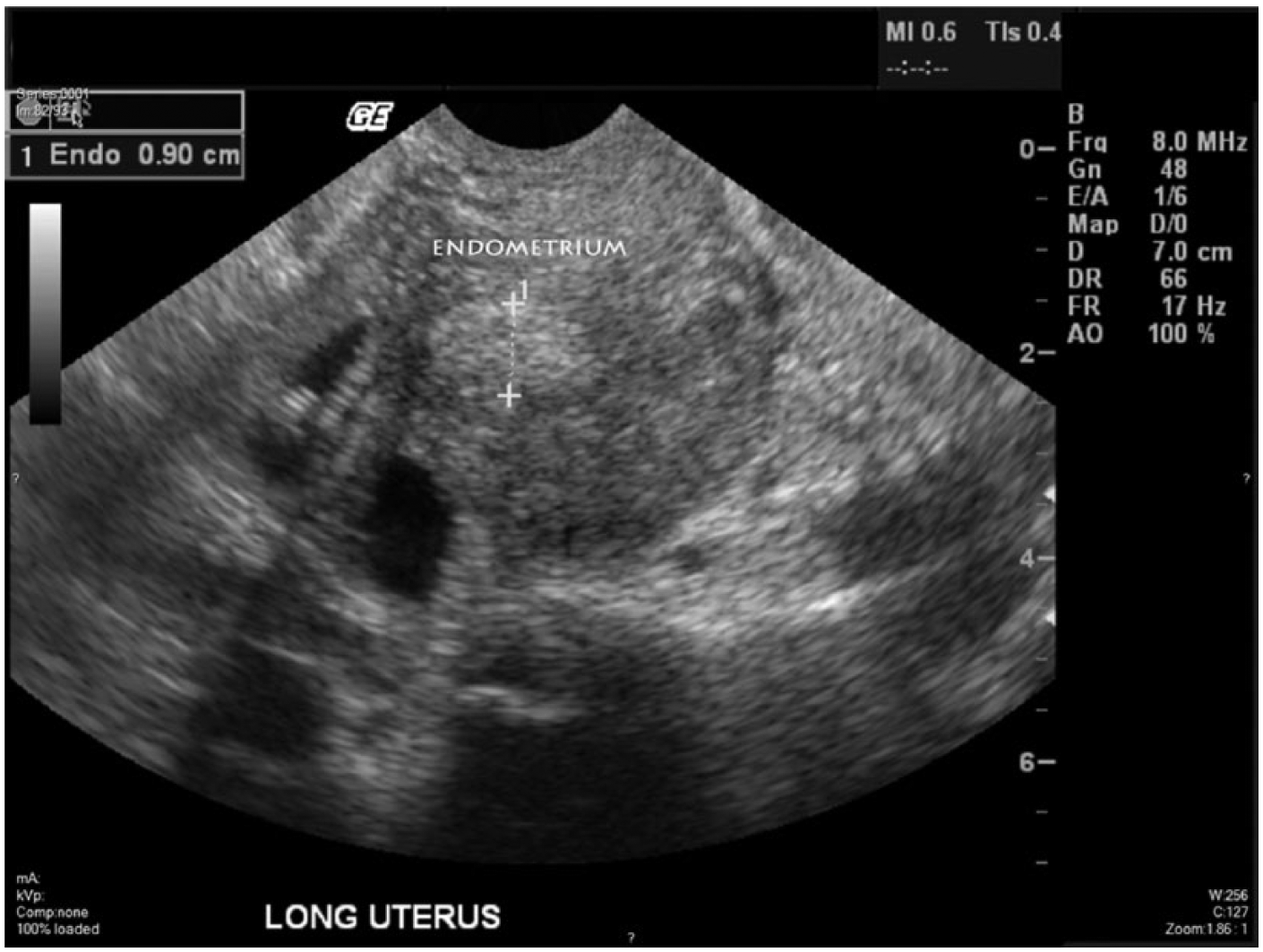
Transvaginal gray-scale sonogram showing uterine heterogeneity; the visualized part of the endometrium measured 0.9 cm at its thickest point.
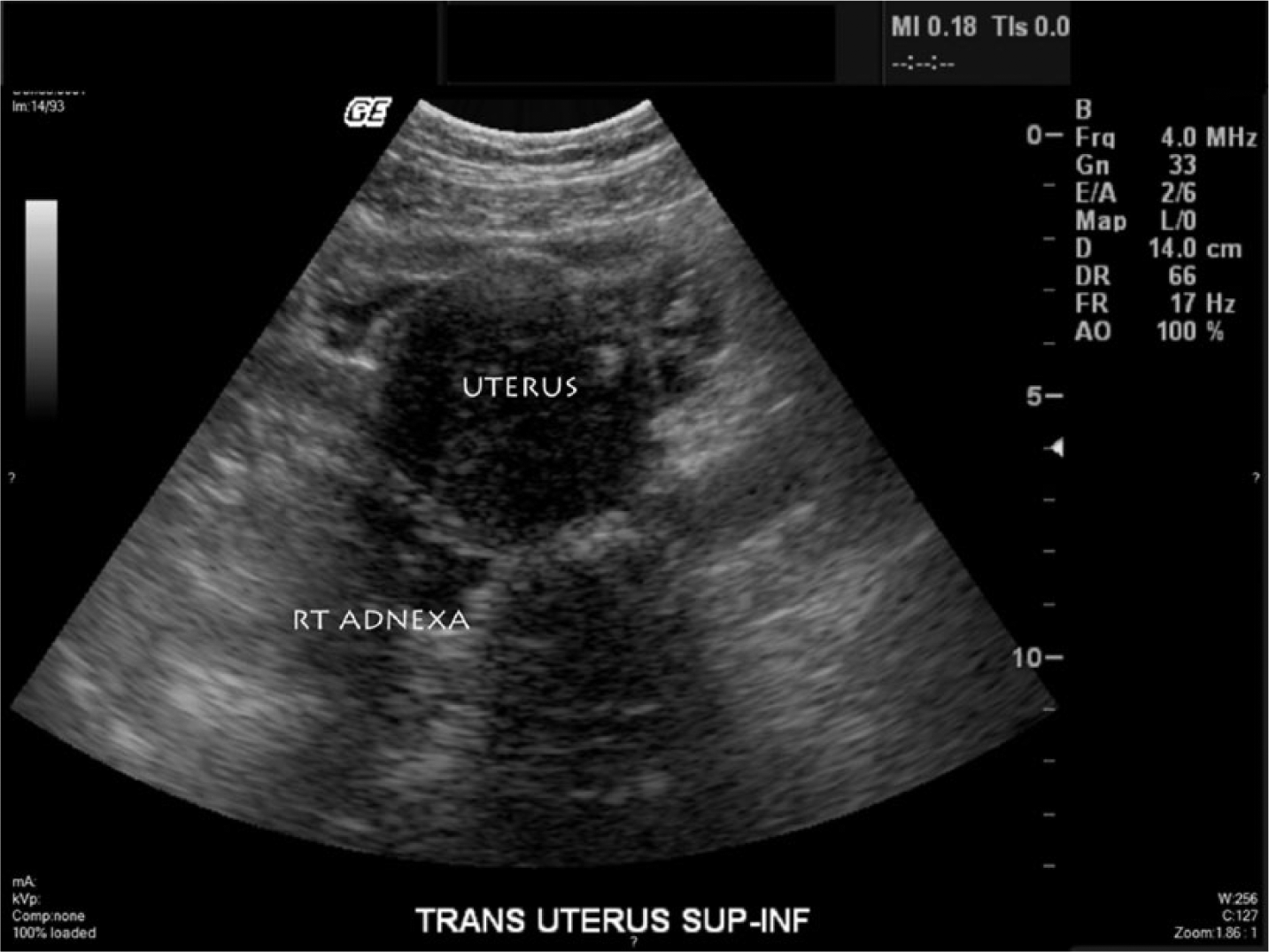
Transabdominal gray-scale sonogram showing the enlarged uterus and a complex cystic structure in the right adnexal region.

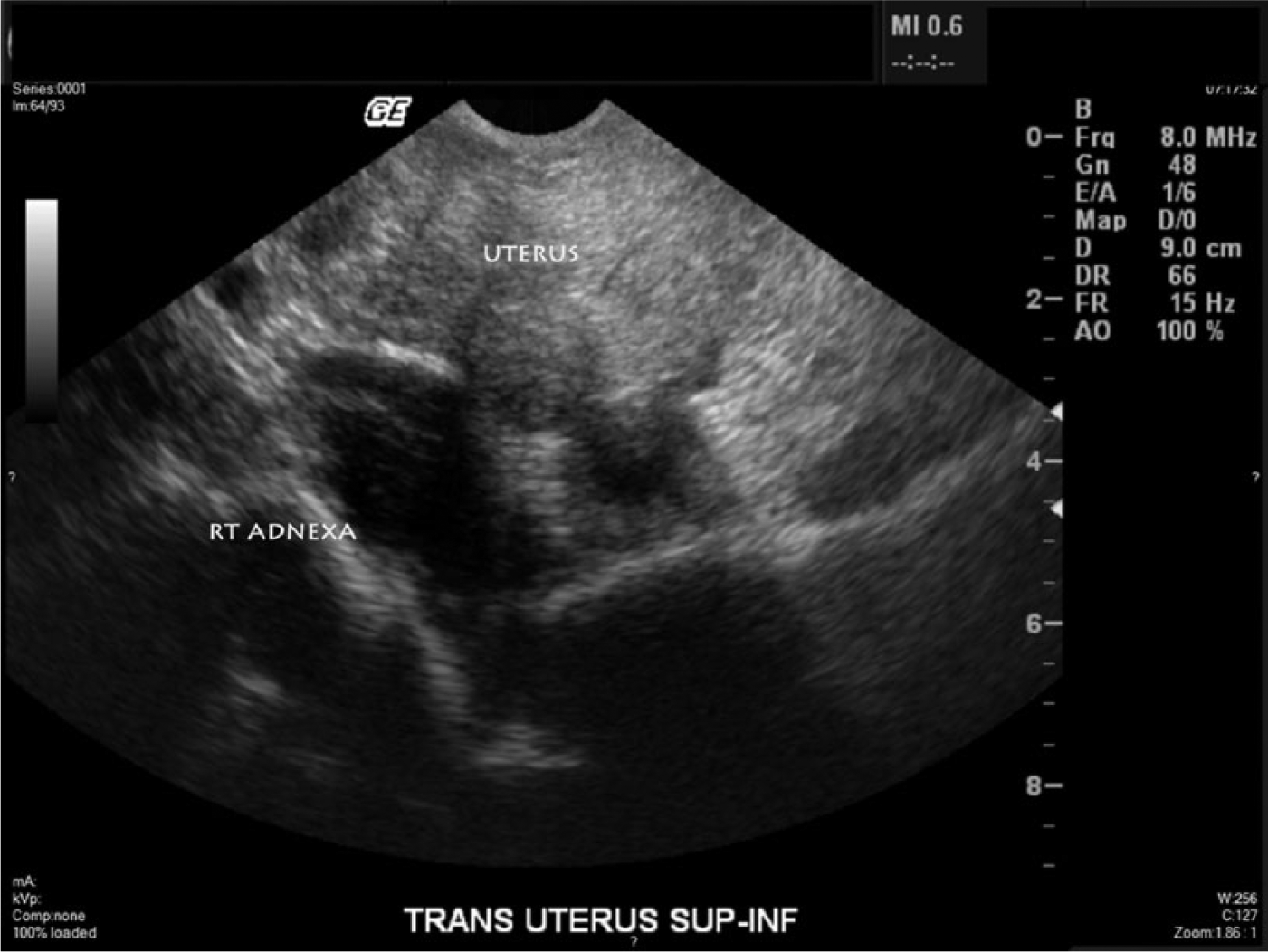
Transvaginal sagittal gray-scale sonogram showing the enlarged and heterogeneous uterus with a complex cystic structure in the right adnexal region measuring 2.9 × 1.9 cm.
Transvaginal gray-scale sonogram showing the enlarged and heterogeneous uterus with a better image of the complex cystic structure in the right adnexal region. The cyst can be seen to be unilocular, with a slightly irregular wall, and with cystic contents appearing to have internal thread-like structures (possible fibrin strands, septa, or debris). No posterior acoustic shadowing can be seen, and no appreciable Doppler flow (not shown) was noted.
Considering recommendations on management of asymptomatic ovarian and other adnexal cysts imaged sonographically by the Society of Radiologists in Ultrasound consensus, 5 MRI was suggested to further clarify the right adnexal lesion and better visualize the endometrium. Two days after the pelvic sonogram, MRI of the pelvis without and with contrast was performed using a GE Discovery LS 1.5 Tesla scanner (GE Medical Systems, Milwaukee, Wisconsin). The following sequences were provided: three-plane localizer, T2-weighted sagittal and axial, fat-saturated T2-weighted axial, fast spoiled gradient echo (FSPGR) T1-weighted and fat-saturated FSPGR T1-weighted axial sequences of the pelvis, and angled T2-weighted sequences through the axis of the uterus, before intravenous contrast administration. With intravenous contrast, fat-saturated FSPGR T1-weighted axial, sagittal, and coronal sequences of the pelvis were obtained. The patient was injected with 10 mL of MRI contrast, OptiMARK (Mallinckrodt Pharmaceuticals, manufactured by Liebel-Flarsheim Company LLC, Raleigh, North Carolina). On MRI examination, the uterus again showed multiple fibroids. The endometrium was visualized, measuring up to 0.3 cm in thickness (Figure 5). The ovaries were not clearly detected. In addition, multiple bilateral cystic structures without enhancement in the sacral region, compatible with bilateral Tarlov cysts, were detected. On the right side, a TC extended beyond the first right sacral neural foramen and measured 3.6 × 2.0 × 2.4 cm (Figures 6 and 7).

T2-weighted sagittal pelvic magnetic resonance image (MRI) showing the enlarged uterus with numerous leiomyomas. The endometrium is visualized more clearly than on transvaginal sonography and was measured as being only 0.3 cm in thickness.

T2-weighted sagittal pelvic magnetic resonance image showing a Tarlov cyst originating in the sacral region of the spinal canal.

T2-weighted coronal pelvic magnetic resonance image showing bilateral Tarlov cysts in the sacral region. The cyst on the right can be seen to correspond to the 2.9-cm complex right adnexal lesion seen on the sonogram in Figure 3.
Discussion
Tarlov cysts occur in about 1% to 5% of the general population. 6 The exact etiology of the TCs is uncertain, and possible causative factors include inflammation, trauma, congenital origin, and degenerative processes. 7 They are typically asymptomatic and found incidentally on MRI or computed tomography (CT) of the lumbar spine and sacrum. They are frequently multiple. 7 Tarlov cysts are best appreciated by MRI, which is able to show the connection of the mass to the thecal sac or nerve roots (nonovarian cystic lesions).
Depending on their location, size, and relationship to the nerve roots, some of those cysts may become symptomatic and cause sensory disturbances, motor deficits, or bowel/bladder dysfunction. Patients with symptomatic Tarlov cysts may also complain about low back pain, sciatica, and nonspecific symptoms such as abdominal pain and headache, possibly because of the extrinsic compression of the regional nerves and internal organs by the cysts.6–8 These symptoms occur in approximately 1% of patients. The clinical significance of a TC must be meticulously assessed before planning surgical treatment. There is no consensus on the best treatment of symptomatic sacral cysts, although various surgical strategies have been proposed. 6
The patient above had a complex adnexal cyst that turned out to be a Tarlov cyst, situated in front of the lumbar-sacral region. A similar cyst could be found incidentally on pelvic sonographic examinations, where it may present itself as a simple or complex, anechoic or hypoechoic structure of various shapes adjacent to the uterus and/or ovaries. Such lesion could be erroneously diagnosed as hydrosalpinx, paraovarian or ovarian cyst, hematoma, or abscesses.7,8
The sonographic characteristics of TCs that may help distinguish them from adnexal cysts include more posterior location, bilateral presentation, and absence of movement with respiration. 7 The uterus, ovaries, and lesions associated with the female’s urogenital organs move with respiration because they are supported by the pelvic floor, which shifts parallel with the diaphragm during breathing.9,10 Tarlov cysts, on the other hand, are connected to the extradural space of the spinal canal rather than the pelvic floor, hence the lack of movements with respiration. Perineural cysts are usually confirmed on MRI, CT, or myelography. The presence of internal thread-like structures, septa, or debris on transvaginal sonography and a corresponding heterogeneous T2-weighted MRI signal may represent the occurrence of blood or non-blood-related cells and might support the traumatic etiology of Tarlov cysts. 11
In the case presented, the sonographically measured endometrial thickness may have been seriously exaggerated due to the distortion of the myometrium by leiomyomas. There was a noticeable discrepancy in the measurements of the endometrial thicknesses between the initial sonogram and following MRI examination. Cases such as this should lead to further investigation of the endometrium. A sonographically thickened endometrium is worrisome for endometrial cancer, the most common gynecologic malignancy in North America. 12
Conclusion
Adnexal masses seen on pelvic sonography have an extensive differential diagnosis. We present an unusual case, a Tarlov cyst, mimicking a complex adnexal cyst. The sonographic characteristics of a TC include the posterior location (closer to the spine), possible bilateral presentation, and absence of movement with respiration. The differential diagnosis comprises hydrosalpinx or pyosalpinx, paraovarian or ovarian cysts, hematomas, and abscesses.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.