
Abstract
Nutcracker syndrome is a venous entrapment phenomenon characterized by the impingement of the left renal vein between the superior mesenteric artery and abdominal aorta. Treatment, if necessary, consists of surgical intervention. In the case presented, a young female presented at an outpatient vascular surgical center for surveillance of a surgically repaired nutcracker syndrome. A renal sonogram was performed to evaluate patency and hemodynamics of the left renal vein. Color and spectral Doppler were used to evaluate the left renal vein as well as the left kidney to document appropriate renal perfusion.
Introduction
Nutcracker syndrome is a venous entrapment phenomenon characterized by the compression of the left renal vein (LRV) between the superior mesenteric artery and abdominal aorta.1–9 Although the prevalence of this syndrome is low, sonography is looked to as the first tool of detection. Nutcracker syndrome can present with a multitude of symptoms, both sonographically and clinically. Sonographic indicators such as abnormal LRV hemodynamics, increased left kidney size, increased LRV size, and presence of venous collateral vessels should all be taken into consideration when attempting to detect nutcracker syndrome. Similarly, it is important that these indicators are evaluated in the monitoring of individuals who have known nutcracker syndrome or are postsurgical intervention for nutcracker syndrome, as this case study reports.
Case Study
An 18-year-old female patient presented with a 13-month history of left flank and upper abdominal pain, stating that 13 months ago, she awoke with severe generalized abdominal discomfort. Over this 13-month timeframe, she also reported a 40-pound weight loss. In addition, she had painful menses and reported intermittent hematuria. Urinalysis confirmed small amounts of blood in her urine. She had previously had upper and lower endoscopy procedures that showed Helicobacter pylori without ulcers.
Because of the history of abdominal pain and weight loss, an omnipaque non-ionic contrast computed tomography (CT) angiogram/venogram was done. Images were reconstructed in coronal and sagittal planes to maximize spatial resolution and aid in determining the exact location of blood vessels. The CT scan demonstrated focal narrowing of the LRV between the superior mesenteric artery and aorta (Figure 1). Further evaluation showed the LRV to be nearly occluded, consistent with nutcracker syndrome. With the significant symptoms, surgical intervention was considered necessary, and because of the young age of the patient, a transposition of the LRV was elected.
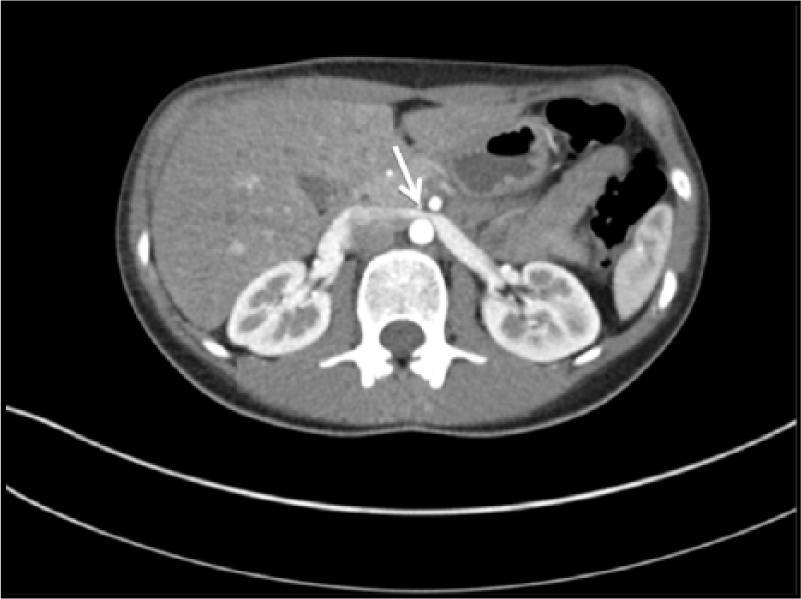
Transverse view of a computed tomographic scan showing the narrowing of the left renal vein (arrow) as it passes between the abdominal aorta and the superior mesenteric artery.
The surgery was done through a standard middle incision. Care was taken to mobilize the LRV without ligation or compromise of tributary branches such as the gonadal (ovarian) vein. The vein was translocated approximately 5 cm caudal to the original insertion site on the vena cava in an end-to-side fashion. The patient did well postoperatively, without any change in renal function.
A postoperative CT scan of the abdomen and pelvis, with contrast, was done to confirm patency of the LRV as well as rule out any other surgical complications (Figure 2). This CT showed surgical clips within the retroperitoneum adjacent to the LRV with a widely patent LRV, confirming the success of the surgery. No other pathology was seen, and there were no significant complications of the surgery.
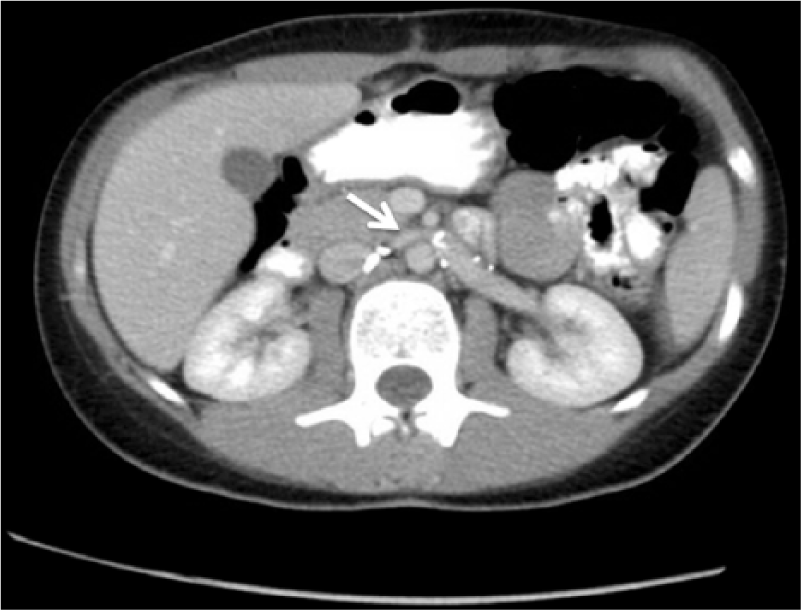
Transverse view of a computed tomographic scan done postoperatively to confirm patency of the left renal vein (arrow). Surgical clips can also be seen within the retroperitoneum.
Following surgical intervention, sonography was used for surveillance. Annual renal sonograms are done to evaluate patency of the LRV and perfusion of the left kidney. Color and spectral Doppler are used to interrogate the blood flow in the LRV returning to the inferior vena cava (IVC) (Figure 3). Color and spectral Doppler are also used to examine the vasculature within the left kidney, most specifically between the medullary pyramids and within the outer cortex to ensure appropriate kidney perfusion (Figure 4). Measurements of left kidney size were also done to rule out any atrophy or hypertrophy that may be occurring due to changes in vascular perfusion. These same measurements were taken on the contralateral kidney to be used as a comparison parameter.
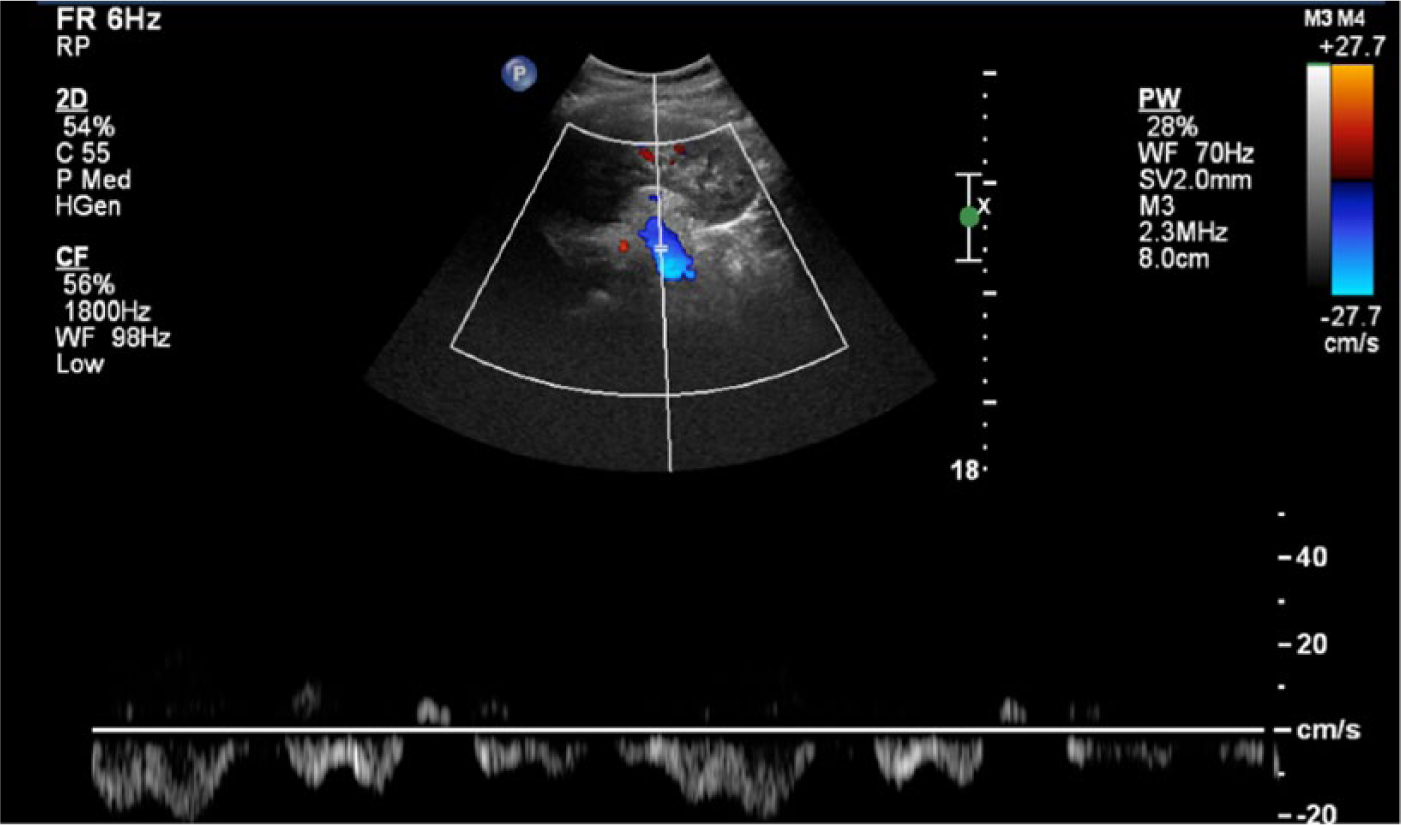
Longitudinal color and spectral Doppler image of the left renal vein following surgical repair of a nutcracker syndrome to evaluate venous blood flow returning to the inferior vena cava.
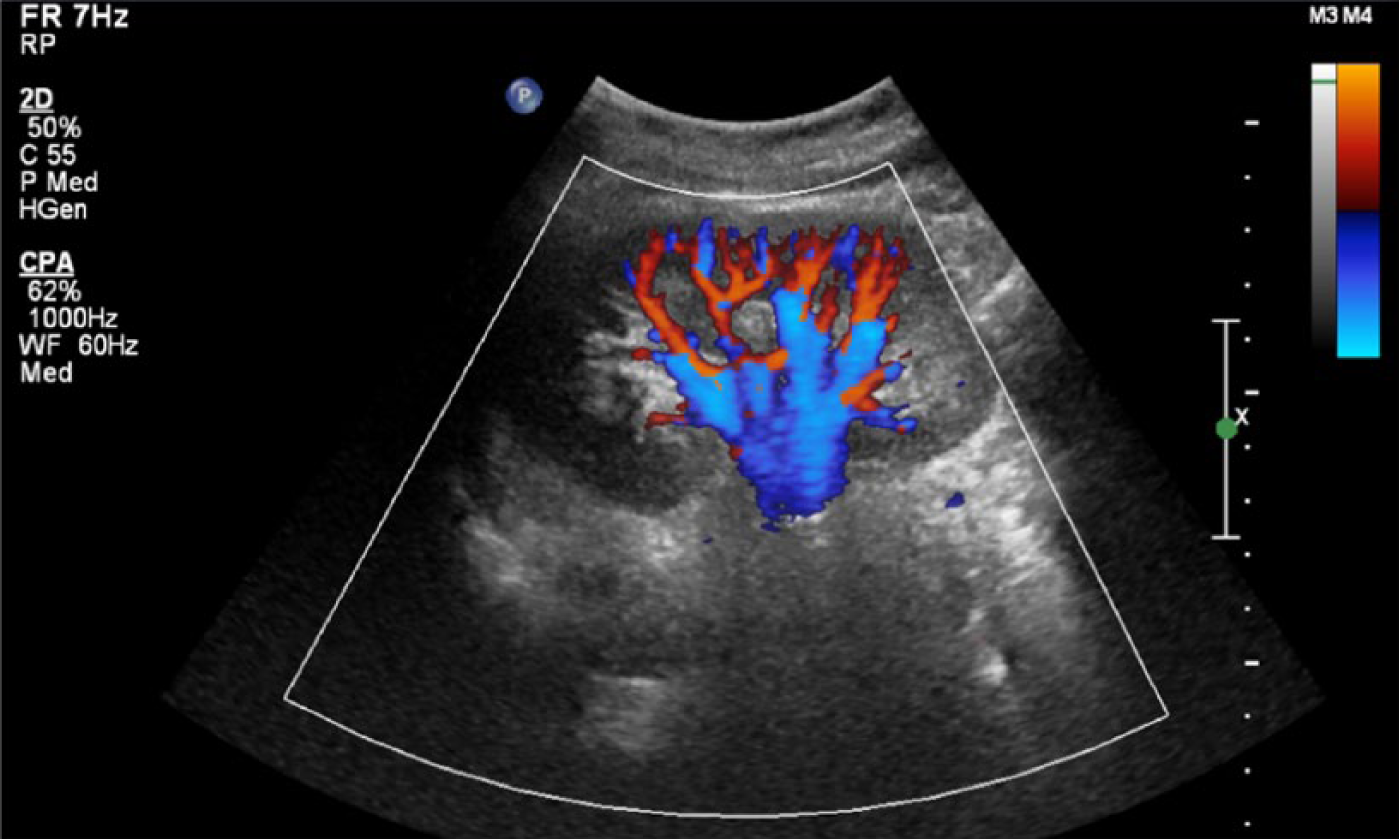
Longitudinal color Doppler image of the left kidney following surgical repair of a nutcracker syndrome to ensure appropriate perfusion of the kidney throughout the cortex.
Discussion
Nutcracker syndrome, which is characterized by the compression of the LRV, is described in two different forms. The first, which is the focus of this case study, is known as anterior nutcracker syndrome. This is characterized by the compression of the LRV between the abdominal aorta and the superior mesenteric artery. 1 In these cases, it has been found that the superior mesenteric artery branches off the aorta at an acute angle of less than 90 degrees, which in turn causes narrowing of the space through which the LRV travels.5,10 The second form, known as posterior nutcracker syndrome, occurs in individuals with retroaortic or circumaortic renal veins, and the LRV compression is caused by impingement between the aorta and the vertebral body.1,11–14
At present, renal Doppler sonography is recognized as the gold standard, receiving a ranking of three out of four from the American College of Radiology (ACR) Appropriateness Criteria, for children presenting with hematuria. 15 However, sonography is not considered the gold standard for nutcracker syndrome in adults, although it is often used as a tool for initial assessment (Figure 5). In a study by Takebayashi et al., 6 a sensitivity of 78% and specificity of 100% were found using only sonography as a diagnostic method, leaving room for improvement for sonographic detection.
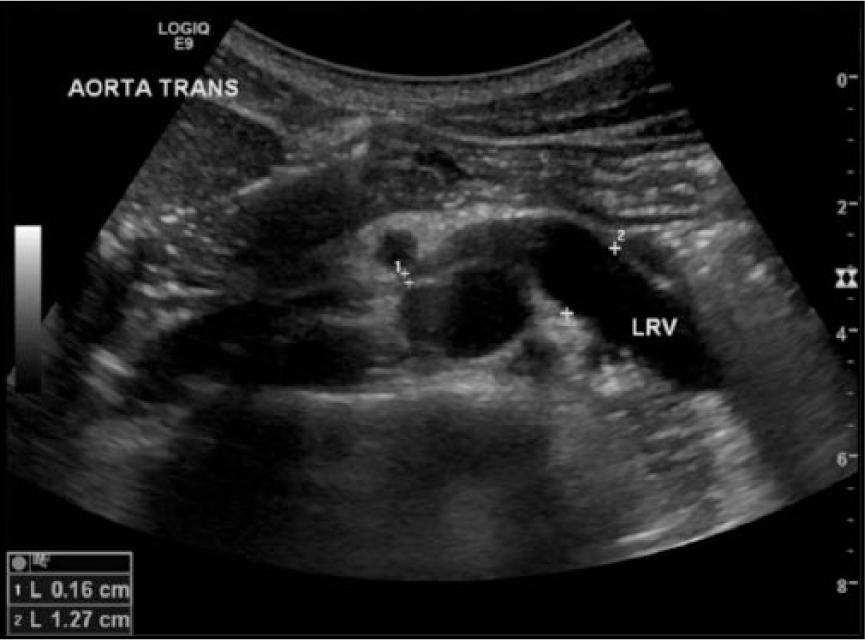
Transverse sonographic image of the left renal vein being compressed between the descending aorta and superior mesenteric artery (caliper 1). Permission obtained from Dr. Donna D’Souza, Radiopaedia.org.
Multiple factors should be taken into consideration when performing a sonographic evaluation for the suspicion of nutcracker syndrome. Initially, the size of the left kidney should be examined and compared to the size of the right kidney. Kim et al. 16 demonstrated a significant increase in left kidney size as compared to the right in patients with nutcracker syndrome. This finding is consistent with the pathophysiology of the syndrome, as the compression of the LRV increases venous pressure and causes the backup of venous blood in the left kidney. This retention of extra blood is felt to be the cause of the increase in kidney volume and the enlargement of renal vessels. Similarly, distention of the LRV has also been examined as to whether this measurement has the capability of improving nutcracker syndrome diagnosis. Guidelines have been reported stating that anterior-posterior measurements should be made of the renal vein at the renal hilum as well as at the location of where the LRV crosses the aorta and superior mesenteric artery. If the ratios of anterior-posterior measurements and peak venous flow velocities at these two locations exceed a factor of five, nutcracker syndrome should be suspected.5,17 However, Takebayashi et al. 6 concluded that measurements of the LRV may be inconclusive because of the potential presence of collateral venous flow. 1
It is thus appropriate that venous collateral vessels also be examined while attempting to determine the presence of nutcracker syndrome. Due to the increased venous pressure in the LRV toward the hilum of the kidney, the potential for collateral venous branches to form is high. Varices can present bilaterally on the patient; however, they are more common on the left.18–21 Because of the stenosis in the renal vein, venous distention and then presence of collateral pathways should be considered in its evaluation. 22 One main venous collateral pathway is the left gonadal (ovarian) vein, which will often appear dilated with associated retrograde flows. 22 Other common pathways include the left adrenal vein, which should also be evaluated for dilation and reflux. 18 It is important that these collateral vessels are documented and evaluated for flow direction, as this adds another piece of diagnostic information that can aid in the decision of the pursuit of further imaging.
Multiple imaging methods can be used to aid in the diagnosis of nutcracker syndrome. A variety of magnetic resonance imaging (MRI) and CT techniques, as well as angiography, have been used to gain more information on the status of the LRV. 1 Kurklinsky and Rooke 1 have reported that the use of multiphase CT urography is almost always required before any surgical intervention is done, as it is able to detect other causes of hematuria, such as renal tumors, arteriovenous malformations, and urothelial tumors, as well as better display the spatial relationships of the vessels being examined. The case presented above used an omnipaque non-ionic contrast CT angiogram/venogram preoperatively to determine the presence of nutcracker syndrome. Images were reconstructed in a coronal and sagittal plane to maximize spatial resolution and aid in determining the exact location of vessels.
Computed tomography imaging as used in the diagnosis for this case is deemed the most appropriate by the ACR Appropriateness Criteria guidelines for adult patients presenting with isolated hematuria. 23 It is important to note, however, that in patients in the pediatric population presenting with these criteria, an ultrasound of the kidneys and bladder is deemed most appropriate by the ACR, receiving a ranking of seven out of ten. 23 This practice of evidence-based medicine could lead to an expedited diagnosis as well as less radiation exposure to the patient.
Once determined, any necessary treatment consists of surgical or endovascular intervention. Multiple interventions are described in the literature, with the goal being to decrease LRV hypertension and restore normal left renal venous hemodynamics. 1 In this particular study, LRV transposition was used to restore venous blood flow to the IVC. Renal vein stenting, another common method of relieving LRV hypertension, was determined to be inappropriate for this particular case because of the young age of the patient and the unknown long-term effects of a renal vein stent.
This case study is being presented as a postsurgical follow-up to emphasize the techniques that should be used to ensure not only a patent LRV but also a healthy and well-perfused left kidney. As mentioned earlier, color and spectral Doppler should be used to examine the vasculature within the kidney. A quantitative measure of cortical renal perfusion is the resistive index (RI), a relative measure of peak systolic (PSV) versus end diastolic flow (EDV) velocities (RI = PSV – EDV / PSV). This measurement can be accessed and automated via the measurement package of any modern ultrasound system within the spectral Doppler mode. Because the vessels in the normal kidney are characterized as a low resistance bed, blood flow coming into the kidney should result in continuous forward flow through diastole.24,25 Based on the empirical data in the literature, 0.70 has been deemed the upper limit of normal for an RI in the kidneys. 24 In the case of acute renal thrombosis, Dubbins 25 and Parvey and Eisenberg 26 have reported an elevated RI seen within the kidney. 24 Because in both acute renal vein thrombosis and nutcracker syndrome, outflow of the renal vein is obstructed, this principle can be applied to both disorders. For this reason, increased RIs present in a left kidney in a patient who has undergone an intervention to relieve the presence of nutcracker syndrome is likely to be indicative of an abnormality such as renal vein thrombosis or a re-stenosis of the LRV.
Conclusion
The case study presented has reviewed the pathophysiology and diagnostic techniques associated with the postoperative follow-up of surgical repair of a nutcracker syndrome. Although this is a relatively uncommon reason for completing a renal sonogram, nutcracker syndrome should always be taken into consideration as a possibility with a patient presenting with left flank pain and/or hematuria. A sonogram is often the first step toward making the nutcracker diagnosis, and for this reason, careful interrogation of the LRV is imperative.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.