
Abstract
Objective:
To determine if a simulation lab using lightly embalmed cadavers would improve diagnostic medical sonography (DMS) students’ perceived competence in ultrasound-guided native renal biopsy examinations.
Methods:
Subjects included DMS students (n = 49) enrolled in academic years 2012 to 2018. Each DMS student performed a native renal biopsy with a nephrology fellow. Skills practiced included machine setup, inferior renal pole localization, biopsy guide preparation, needle visualization, and communication skills. Pre- and postlab surveys assessed DMS students’ perceived competence.
Results:
Prelab, 12% (n = 6) of students felt competent to assist in the procedure. Postlab, 61% (n = 35) of students felt competent, a statistically significant (P < .001) change. All students viewed the lab as a valuable experience. Hands-on experience (53%), student/physician collaboration (33%), and low-stress environment (13%) were reported themes. Additional resources (50%) and scheduling (22%) were areas for improvement.
Conclusion:
A renal biopsy simulation lab using lightly embalmed cadavers is an effective method to improve DMS students’ perceived competence in this procedure.
Percutaneous renal biopsy is considered the gold standard in diagnosis and management of many kidney diseases. 1 A renal biopsy can cause serious complications, including hematoma with need for blood transfusions, additional surgical procedures including nephrectomy, and rarely death. 2 The use of ultrasound guidance in this procedure has improved accuracy, increased patient safety, and helped reduce complications. 2 Ultrasound-guided biopsy is recognized as one of the most important methods of tissue diagnosis in radiology practices worldwide 3 and is a recommended standard of practice by the American Society of Nephrology. 1 Sonographers play an important role in the success of ultrasound-guided renal biopsy procedures. It takes practice and experience to develop the skills and confidence to participate in these procedures. Due to the technical nature of the examination and the risk of patient complications, it can be difficult for sonography students to practice and gain experience in ultrasound-guided biopsy examinations while in the clinical education setting.
One way to provide students with experiential learning is through simulation. Simulation serves as an effective bridge between didactic learning and performance of procedures on patients.4,5 Simulation allows for development of necessary skills without placing patients at risk and provides a lower stress yet realistic learning setting.6–8 The knowledge and skills practiced in simulation are taught in a clinical context, so students can retain and apply these skills in their clinical practice. 5 Simulation also allows learners to receive feedback on their performance of their procedural skills. It also provides an opportunity to retry and improve the skill after feedback has been given. 5 Research has proven that practicing skills, with simulation, increases the possibility of future success and decreases the possibility of complications.9,10 A review of medical education simulation activities demonstrated reduced procedural complications, such as pneumothorax or excessive needle passes. 8 Learning in a simulated environment has also been reported to increase confidence of the learners to perform procedural skills.5,11
The number of institutions using lightly embalmed cadaver-based educational simulation is increasing.5,12–15 Studies by these facilities are adding to the body of knowledge on the effectiveness of this simulation model. Benefits of using lightly embalmed cadavers in medical education include increased learner confidence, reduced time required to perform a skill, and increased accuracy in diagnoses. Lewis et al. 13 developed a cadaver-based program to teach surgical residents complex surgical procedures. Over half of participants either strongly agreed or agreed the simulation increased their confidence in performing procedures. 13 Levine et al. 14 studied the time it took to perform surgical procedures prior to and after laparoscopic training on lightly embalmed cadavers. After the training, participants’ median time to complete a suture decreased from 106.5 seconds to 26.5 seconds. 14 A study conducted by Keim Janssen et al. 5 used this model for enhancing anatomical learning and clinical competence in an interdisciplinary team of students to diagnose anterior cruciate ligament (ACL) tears. Participants who received hands-on training with lightly embalmed cadavers correctly diagnosed 72% of ACL tears, compared to 21% of participants who only received knowledge of ACL diagnosis in a didactic format. 5 Results of the study also showed that hands-on training with the cadavers increased confidence and retention of knowledge among participants. 5
In recent years, lightly embalmed cadavers have become a simulation model for ultrasound-guided diagnostic procedures.7,11,12,16,17 Lightly embalmed cadavers differ from the traditional cadavers because a weaker embalming fluid is used, a smaller volume of fluid is used, and the fluid is not allowed to collect in the tissues.14,18 This technique allows tissue of the lightly embalmed cadavers to retain a more natural tissue texture than those of traditionally embalmed cadavers.14,18 Sonographic imaging of subcutaneous tissues, liver, and kidneys in lightly embalmed cadavers demonstrates excellent preservation and near-realistic visualization of anatomy.7,19 Biopsy needles are also easily visualized sonographically within tissues of lightly embalmed cadavers, which allow for their use in ultrasound-guided renal biopsy training. 7 Other advantages of cadaver-based simulation include no risk to patients, multiple students and fellows trained in the same session, and use of multiple cadavers to acquire technical skills.7,19–22 By providing a realistic means of practicing percutaneous renal biopsy, the use of lightly embalmed cadavers keeps with best practice in clinical simulation education. 19
The use of simulation with sonography and lightly embalmed cadavers has been documented in medical student and resident education.7,11,12,18,20 For example, Hoyer et al. 12 used sonography and lightly embalmed cadavers to enhance the anatomy curriculum for medical students. However, utilization of this teaching strategy in diagnostic medical sonography (DMS) education has not been commonly reported in the literature. The purpose of this study was to determine if a simulation lab using lightly embalmed cadavers would improve DMS students’ perceived competence in ultrasound-guided renal biopsy examinations.
Materials and Methods
The subject population consisted of 49 students enrolled in a DMS program at an academic health sciences center in the Midwest, over a period of seven years (Table 1).
Subject Numbers Demonstrated for Each Year of the Study.
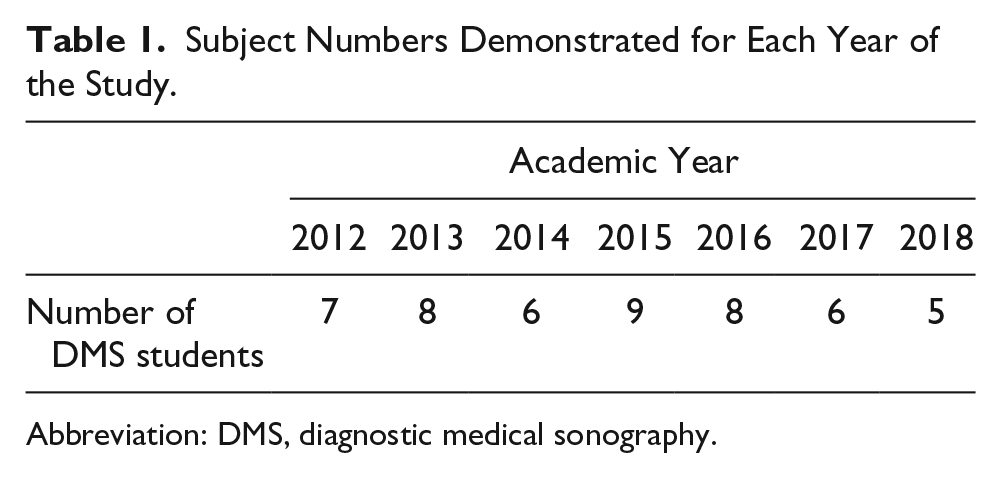
Abbreviation: DMS, diagnostic medical sonography.
All participants followed the same 12-month curriculum, which included didactic and clinical education simultaneously. Prior to the lab simulation, students had two one-hour didactic lectures on ultrasound-guided renal biopsy examinations covering indications and contraindications, patient preparation, sterile technique, equipment and biopsy guide information, procedural and postprocedural steps, and complications. Students averaged 26 hours per week in the clinical education setting. Clinical rotations provided varying exposure to invasive procedures, although all participants rotated to one site that routinely performed renal biopsies.
The simulation lab was held annually, in March or April, depending on department faculty and nephrology fellow availability. The nephrology fellows were either in their first or second year of fellowship training and had varied levels of experience in performing native kidney biopsies. Two lightly embalmed cadavers were ordered through the Gross Anatomy Department each year. After year 2, only male cadavers were used due to wider space below the costal margin and easier scanning. Prior to the start of the simulation lab, each DMS student completed a three-question prelab survey on the number of native renal biopsies observed, the number of native biopsies performed, and perceived level of competence to perform a native kidney biopsy.
The simulation lab was supervised by the same sonography and nephrology faculty each year, both credentialed in their respective fields. The simulation lab protocol was standardized and followed each year. The lab began with introductions of DMS students, nephrology fellows, and supervising faculty. The nephrologist then led an interactive discussion reviewing a native kidney biopsy procedure that included indications, contraindications, pertinent lab values, and patient safety protocols. Strong emphasis was placed on the importance of the sonographer’s role in a successful biopsy and the need for teamwork and communication between the sonographer and nephrologist.
After the introductory discussion, the group moved to the cadavers, where dialogue focused on patient position and biopsy supplies used during the procedure. The ultrasound machines used for the lab were Philips iU22 (Bothell, Washington) between 2012 and 2015 and Philips ClearVue 650 between 2016 and 2018. Each DMS student practiced placing the biopsy guide on the transducer and using the biopsy guidance feature on the ultrasound machine. The order of participants was voluntary, and each DMS student participated in a complete renal biopsy with a nephrology fellow. Students and fellows who were not actively engaged in biopsy practice were present in the lab and allowed to observe. Due to the cost of cadavers, both kidneys were used for practice during the lab.
For each biopsy, the ultrasound machine, DMS student, and supervising sonographer were on the left side of the table, the nephrology fellow on the right, and the nephrologist at the table head. Using a 5- to 2-MHz transducer, the DMS student located the assigned kidney and renal anatomy was reviewed. The DMS student and nephrology fellow worked together to determine the best needle angle for the biopsy and the depth to the inferior pole. The DMS student marked the biopsy site with an indelible marker for the incision. Faculty synchronously added verbal suggestions for improvement on transducer manipulation for optimal needle placement of the 18-gauge, 20-cm Bard Max-Core (Tempe, AZ) disposable core biopsy instrument. Under the guidance of the nephrologist, the retrieved tissue sample was viewed by both the DMS student and fellow. Biopsies were performed until tissue was successfully obtained and then the next student took over.
At the conclusion of the lab, a four-question postlab survey assessed whether the lab improved biopsy skills, perceived level of competence to perform a native kidney biopsy, what they liked about the lab, and suggestions for future labs. Descriptive statistics, including means and standard deviations, for pre- and postlab survey results were used to summarize the survey data. All analyses were completed using STATA Version 14.2 (StataCorp LLC, College Station, Texas). Qualitative survey questions were analyzed after all data were deidentified and aggregated. Three medical imaging faculty applied the constant comparisons method for analyzing qualitative comments independently and then collaborated to unify codes. This strategy resulted in the identification of themes regarding participants’ experiences with the simulation lab and suggestions for improvement. 23
Results
A total of 49 DMS students participated in the renal biopsy activity between 2012 and 2018. Although prelab didactic education and number of clinical education hours were similar for each academic year, observation and performance of native renal biopsies varied by academic year. Prelab surveys reported 47% of participants (n = 23) had observed a native kidney biopsy during the first seven months of their clinical education. This percentage varied by year with the lowest prelab observations occurring in academic year (AY) 2014 (n = 1, 16%) compared to AY 2017 (n = 6, 100%). Twenty-six participants (53%) had not observed a biopsy (Figure 1). Only 8% of participants (n = 4) reported performing a native kidney biopsy prior to the lab, and this occurred in AYs 2017 and 2018. From AYs 2012 to 2016, no students participated in a native renal biopsy prelab (Figure 2).
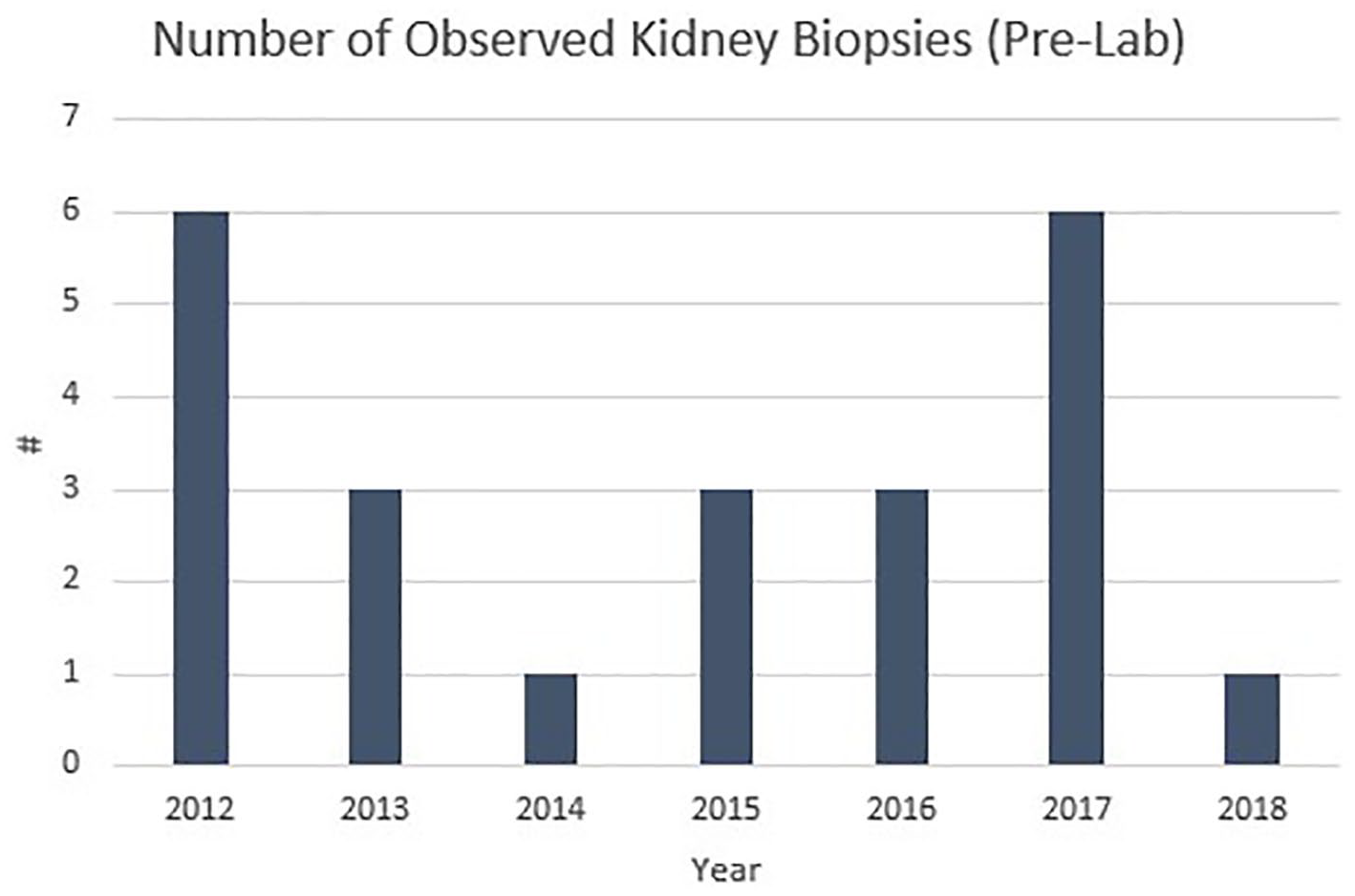
Data demonstrating the number of students each year reported to have observed at least one kidney biopsy prior to the lab.
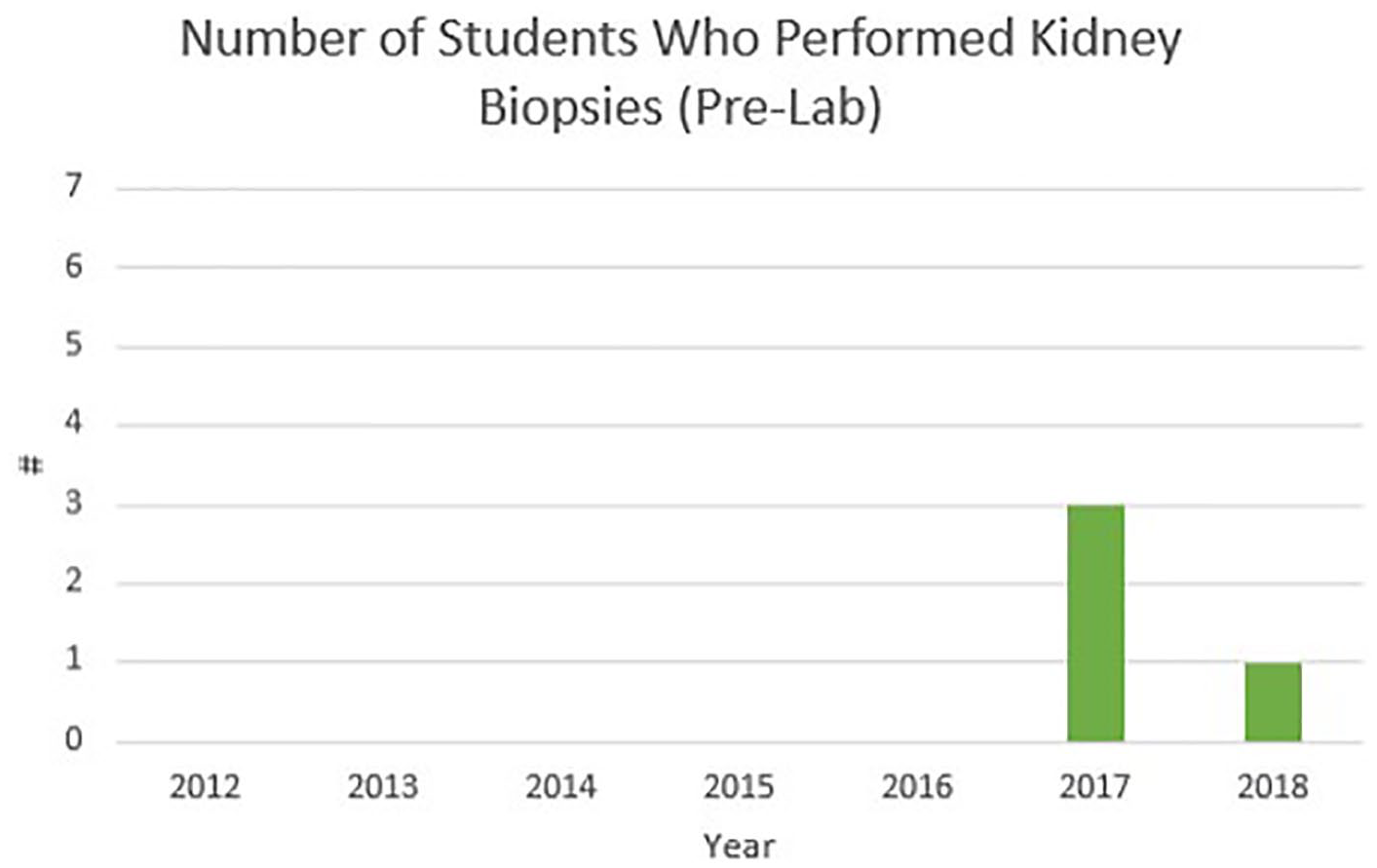
Data depicting the number of students each year reported to have performed a kidney biopsy prior to the lab.
The primary outcome for this study was prelab to postlab change in level of agreement with the question, “Do you feel competent to perform a kidney biopsy?” Prior to the cadaver simulation lab, only 12% (n = 6) agreed or strongly agree with this statement, 14% (n = 7) were neutral, and 74% (n = 36) disagreed or strongly disagreed with the statement. Postlab, 71% (n = 35) agreed or strongly agreed with the question, “Do you feel competent to perform a kidney biopsy?”; 24% (n = 12) were neutral, and only 4% (n = 2) disagreed or strongly disagreed. In this cohort, 100% (n = 49) of the students responded “yes” that the lab improved their skills to perform a native kidney biopsy (Figure 3).
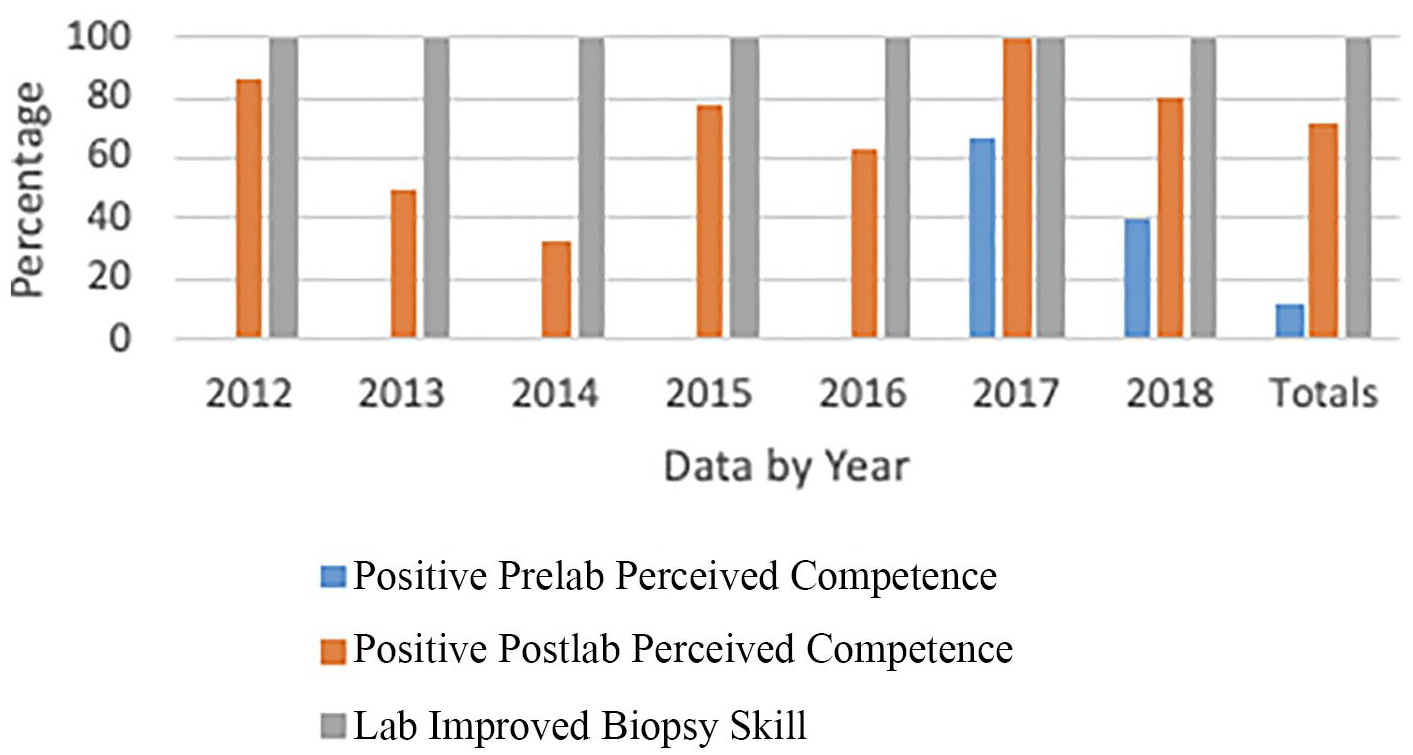
Data demonstrating the reported increase in perceived competence and skills of students to perform a kidney during each year of the study.
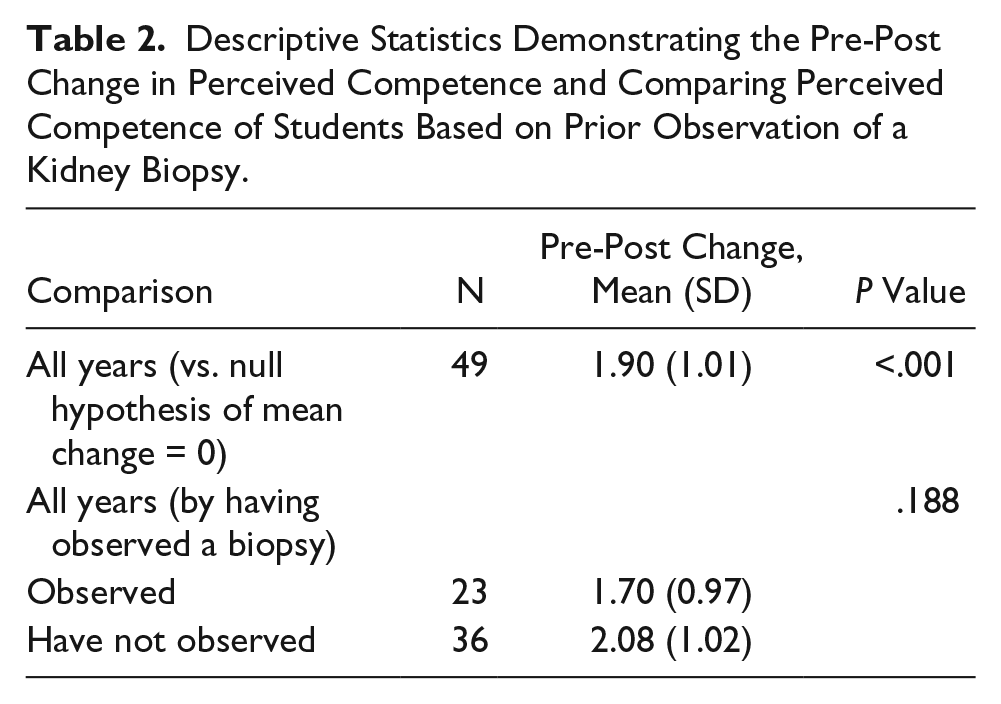
A positive prelab to postlab change of nearly two scale points was noted in students’ perceived competence to perform a native kidney biopsy. A t test showed this change was significantly different from the null value of no change (mean [SD] = 1.90 [1.01], P < .001). Those students who had previously observed a biopsy (n = 23) reported a slightly smaller change than those who had not (1.70 [0.97] vs. 2.08 [1.02]), although this difference was not significant (P = .188) (Table 2). Differences in perceived confidence between those who had previously performed a biopsy and those who had not were not evaluated, as there were only four respondents who reported previous participation.
Descriptive Statistics Demonstrating the Pre-Post Change in Perceived Competence and Comparing Perceived Competence of Students Based on Prior Observation of a Kidney Biopsy.
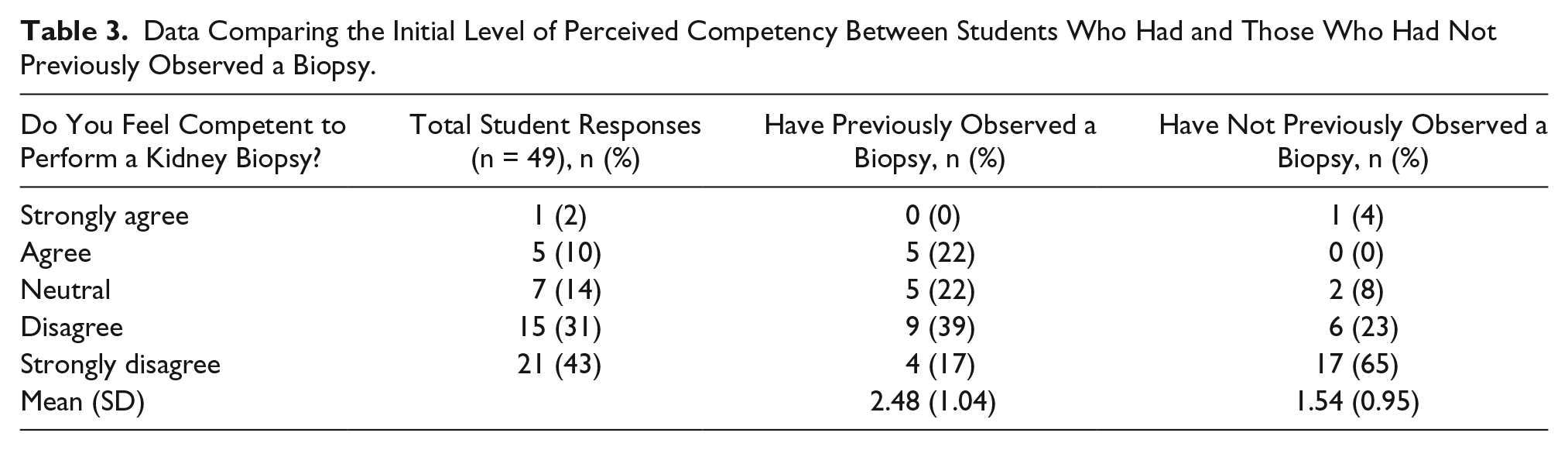
Initial competency was also evaluated by whether the student had previously observed a biopsy. Table 3 demonstrates the distributions of prelab competency by whether students had previously observed a biopsy. The experienced group felt they were significantly more competent that the nonexperienced group (2.48 [1.04] vs. 1.54 [0.95]) as would be expected (two-sample t test P = .002).
Data Comparing the Initial Level of Perceived Competency Between Students Who Had and Those Who Had Not Previously Observed a Biopsy.
Qualitative data were also collected from postlab surveys regarding what students liked about the simulation lab and suggestions for future lab improvements. Most participants (n = 37, 76%) responded to the question, “What did you like about this lab?” with a total of 45 comments. Three themes emerged after analysis, including hands-on experience, collaboration, and low-stress environment. Over half of the comments (n = 24, 53%) were related to hands-on experience gained during the simulation. Participants liked being able to get a feel for scanning during a biopsy and using a biopsy guide. The ability to practice skills outside the clinical environment in a “lifelike setting” was important. One-third of the comments (n = 15, 33%) were related to student/physician collaboration. Participants liked practicing with the nephrology fellows and found it beneficial to understand the needs of the physician during the biopsy procedure. The importance of communication between the sonographer and physician also emerged with this theme. Remaining comments (n = 6, 13%) were related to the low-stress environment of the simulation.
Over half of participants (n = 29, 59%) responded to the question, “What could be done to improve this lab?” with 32 comments. Two themes emerged related to resources/experiences and scheduling. Half of the responses (n = 16, 50%) recommended future labs increase resources or experiences. Participants suggested providing more cadavers, ultrasound equipment, time, and opportunities to practice. Several comments (n = 7, 22%) were related to scheduling of the lab. Participants remarked that scheduling the lab in shifts would allow more time to practice and would reduce the noise level in the lab. Several comments (n = 7, 22%) recommended no changes to the simulation lab.
Discussion
This study is one of the first to report both quantitative and qualitative data gathered from a sonography simulation lab that allowed DMS students to practice ultrasound-guided renal biopsies on lightly embalmed cadavers with nephrology fellows. The development of the simulation lab drew on published literature from medical education that showed the use of lightly embalmed cadavers was an effective method to teach and practice clinical skills in a safe environment.19,24 This type of simulation has also been shown to improve students’ confidence to perform a procedure in the clinical setting.19,14,25,26 The quantitative outcomes from this study support these findings, but also add to literature as a new instructional method for sonography programs to improve DMS student confidence in these challenging procedures, but also a method to ensure consistent education among all students in the program, even with comparable clinical rotations.
Less than 50% of the DMS students enrolled in the program from 2012 to 2018 had observed a native renal biopsy by the second semester of the program. This percentage varied by year from 16% to 100%. The variability possibly relates to the number of students enrolled in the program each year, the inconsistency of examinations performed at different clinical sites, types of examinations performed when students are in clinic, and students’ choice in examination involvement while at a clinical site. The clinical instructor’s (CI’s) encouragement to observe this type of examination may also be an influencing factor. CIs may encourage students to participate in examinations, such as an abdominal ultrasound, that they may routinely perform after graduation to improve competence. Some CIs may want to avoid training students in this often complicated and stressful examination. The amount of time at that site may have varied by student depending on the size of the class. Observation of unique or specialty procedures should be encouraged to help provide the students with a well-rounded education that will ultimately affect their ability to provide quality patient care and be a productive, competent sonographer.
For those 47% (n = 23) of DMS students who did report prelab renal biopsy observation, their examination experience fluctuated also. The majority (n = 15, 65%) reported 1 prelab biopsy observation and the minority (n = 1, 4%) documenting 4 prelab observations. The student with the highest observations did not participate in a native kidney biopsy procedure prelab. This lack of participation may have been attributed to the time restraints in the clinical schedule, patient body habitus, student’s confidence level, or preference of sonographer/nephrologist.
Only 8% (n = 4) of DMS students reported participating in a renal biopsy during their clinical rotations prior to the spring lab. During AYs 2012 to 2016, no students reported participating in an ultrasound-guided renal biopsy. In 2017, 50% of the students (n = 3) participated in 1 renal biopsy before the lab and 17% (n = 1) of the 2018 class. It is not known whether the students participated in the examination in the fall semester or early in the spring semester. Although a renal biopsy examination would not be expected to be performed early in a student’s clinical education, the data show that a small number of students do feel confident enough to seek out this examination early in their clinical experience or have CIs encouraging participation of students who they felt would be successful to participate in this examination.
The opportunity for students to practice a skill, ask questions, and make errors in a safe learning environment that does not affect patient care is instrumental in improving confidence. It can also help in achieving competency for procedures that are not performed on a regular basis.26,27 The opportunity to practice skills without fear of a patient complication, feel comfortable to ask questions, and be in an environment that was not nerve-racking was conducive to a low-stress learning experience. Over half of the comments (n = 24, 53%) about what students liked about the lab were related to hands-on experience gained during the simulation, including using the equipment and guiding during a biopsy. Many students (n = 15, 33%) liked that the lab facilitated communication and collaboration with the physicians. Students were able to ask questions to both supervising faculty and the nephrology fellows, and the physicians were able to communicate their needs during the procedure.
While the simulation activity did improve confidence of the DMS students, there are several challenges to providing this lab, including facilities, cost, faculty, time, and institutional culture. To perform the lab, participants need a gross anatomy lab, which offers lightly embalmed cadavers. It may not be possible for all DMS programs to have access to these special facilities. The expense may also be a drawback for some programs. The cost of cadavers varied each year during the study, most recently costing approximately $665 each. Expenses built into this cost are fees and the infrastructure needed to procure, maintain, and dispose of the bodies. 21 Supplies like biopsy devices and biopsy guides were additional expenses. Participation is needed from supervising faculty in both sonography and nephrology departments, as well as nephrology fellows, which may not be an option for some programs. The DMS program in this study is a part of an academic health science center with availability of clinical physicians and residency and fellowship programs. Time constraints of participants are also a consideration of the lab, as it may be challenging to coordinate schedules of the lab facility, faculty, fellows, and DMS students. In addition, the culture of the educational institution may also be a challenge for some programs if interprofessional education activities are not supported. Limitations of the study include accuracy of student self-reported examinations, small sample size, and collection of data from only one institution.
Conclusion
A renal biopsy simulation lab using lightly embalmed cadavers is an effective method to improve DMS students’ perceived competence in this procedure. In this cohort, 100% (n = 49) of students believed the lab improved their skills to perform a native kidney biopsy. Simulation training offers an alternative to the “see one, do one” method, which carries a potential to cause patient harm or an inadequate biopsy specimen. The use of the lightly embalmed cadavers to teach and practice ultrasound-guided renal biopsy skills had multiple benefits. Sonography students were better prepared to assist with renal biopsies. Nephrology fellows were able to practice performing biopsies without risk to patients. Both groups realized the importance of communication and working as a team to provide a shared service.
Footnotes
Acknowledgements
The authors would like to acknowledge those who graciously donated their bodies to the Nebraska Anatomical Board for education and research. The generous gift of their human remains to the Board allowed this project to be possible. The authors would also like to thank the Joseph C. and Darlene Anderson Professorship and the Charles R. O’Malley Charitable Trust for their support of this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.