
Abstract
Introduction:
Renal biopsy is a useful diagnostic procedure. In developing countries, two techniques of renal biopsy, blind percutaneous renal biopsy and real-time ultrasound-guided percutaneous renal biopsy, have been performed. The majority of studies compared these using different types and sizes of biopsy needle. The aim of this study was to compare both techniques in resource constraint country.
Method:
We reviewed renal biopsy database, between 1 January 2014 to 30 June 2017. The primary outcome was the total number of glomeruli. The other outcomes were tissue adequacy and bleeding complications. We also analyzed multivariable logistic regression to find factors associated with tissue adequacy and bleeding complications.
Result:
Of the 204 renal biopsies, 100 were blind percutaneous renal biopsy and 104 real-time ultrasound-guided percutaneous renal biopsy. The number of native renal biopsies was 169 (82.8%). Baseline characteristics of two groups were comparable. The mean number of total glomeruli from real-time ultrasound-guided percutaneous renal biopsy was significantly more than blind percutaneous renal biopsy (20.8 ± 12.1 vs 16.0 ± 13.0, p = 0.001). The real-time ultrasound-guided percutaneous renal biopsy obtained more adequate tissues than blind percutaneous renal biopsy (45.2% vs 16%, p < 0.001) and was the only factor associated with adequate tissue. Moreover, 16 renal biopsies from blind percutaneous renal biopsy obtained inadequate tissue. The overall bleeding complications were not statistically different. We found being female, lower eGFR and lower hematocrit were associated with bleeding complications.
Conclusion:
In comparison with blind percutaneous renal biopsy, real-time ultrasound-guided percutaneous renal biopsy obtained more adequate tissue and number of glomeruli. While the complications of both were comparable. We encourage to practice and perform real-time ultrasound-guided percutaneous renal biopsy in resource constraint countries.
Keywords
Introduction
Percutaneous renal biopsy (Bx) is a useful diagnostic procedure for kidney diseases.1,2 Adequate tissue and sufficient glomeruli are vital for pathological diagnostic yield. However, biopsy-complications, especially bleeding complications such as hematuria and perinephric hematoma should be of concern.3–5 Two techniques of Bx which are “blind percutaneous renal biopsy (BBx)” and “real-time ultrasound-guided percutaneous renal biopsy (RBx)” are still being performed in developing countries. Previous studies mostly performed BBx with Tru-cut needle showing less efficacy and more complications than RBx which is performed with automated biopsy needle.6–12 That were performed by different type and size of biopsy needles between two groups. The results from studies showed that the different sizes of needle biopsy affects the adequacy of tissue and complications.13,14 The aim of this study was to compare efficacies and complications of both techniques performed with an automated biopsy needle in the same size.
Methods
Study design
This was a retrospective study. We reviewed our renal biopsy database from 1 January 2014 to 30 June 2017.
Population
Our hospital is tertiary, university and referral hospital in Bangkok, Thailand. Renal biopsies were performed when there was an indication and no contraindications, as verified by our nephrology staff. All renal biopsies were done by renal fellows under supervision of nephrology faculty staff. Before 1 August 2016, we performed BBx for all renal biopsies, after that RBx became the standard technique. We included all native and transplant renal biopsies that had completed data. The exclusion criteria were incomplete pathological data.
BBx
The patient lay in the proper position. The ultrasound was used for identifying the kidney, measuring the distance from the skin to renal cortex and marking the proper introducing needle site at skin by the nephrologist. The skin was cleaned with antiseptic solution and draped with sterile towels. Infiltration with 1% or 2% xylocaine at the skin and underlying subcutaneous tissue was performed, then a small incision was made at the skin. The renal biopsy needle was introduced at the site marked on the skin then advanced the expected distance and evaluated from initial ultrasound through the skin and the underlying tissue to the kidney. Verifying the proper location of the biopsy needle was done by observing respiratory movement of the needle. The patient was asked to hold his breath then the biopsy was performed. The needle was immediately removed then the specimen was collected in the container. For transplant kidney biopsy, the proper location of the biopsy needle was justified by feeling the resistance of the kidney. The renal biopsy was re-performed 1–3 times for adequate specimens and sent to the pathology laboratory. The renal biopsy needle was a 16-gauge (G), 15-cm length, automated spring-loaded needle.
RBx
The patient also lay in the proper position. The skin was cleaned with antiseptic solution and draped with sterile towels. The ultrasound probe was covered by a clear sterile cover. The ultrasonic gel was placed between the probe and inner side of the sterile cover. Chlorhexidine solution was used for transmitting ultrasonic waves from the skin to sterile cover. The operator performed aseptic ultrasound for kidney visualization. Local anesthesia was injected then a small incision at the skin was made. The needle biopsy was introduced through the incision site to renal cortex under real-time ultrasound guidance. The patient was asked to hold his breath then the biopsy was performed. The needle was immediately removed then the specimen was collected in the container. For transplant kidney biopsy, the upper pole of allograft was identified and biopsied under real-time ultrasound-guidance. The renal biopsy was re-performed 1–3 times for adequate specimens which were sent to the pathology laboratory. The renal biopsy needle was 16-G, 16-centimeter length, automated spring-loaded needle.
The post-biopsy monitoring
As per our post-biopsy protocol, patients were admitted for 12 h for absolute bed rest and 24 h observation. Vital signs were measured hourly until stable. Complications such as hematuria, abdominal pain, and perinephric hematoma were recorded. We performed renal ultrasound immediately after the biopsy. During the observation period, we performed renal ultrasound only in cases of suspicious bleeding complications. The hematocrit was serially measured if bleeding complication was clinically suspected. Blood transfusions were provided when clinically indicated. The role of renal angioembolization was considered where there were active bleeding complications.
Outcome parameters
The primary outcome was an average number of total glomeruli. The number of total glomeruli was the number of glomeruli from light microscopy specimens plus the number of glomeruli from immunofluorescence specimens.
Secondary outcomes were adequacy of tissue that was categorized in three classes
Complete adequate tissue means specimens included cortex, medulla and all the following: Native renal biopsy: at least 20 glomeruli and 2 vessels. Transplant renal biopsy: at least 10 glomeruli and 1 vessel.
Essential adequate tissue means specimens included cortex, medulla and all the following: Native renal biopsy: at least 10 glomeruli and 1 vessel. Transplant renal biopsy: at least 7 glomeruli and 1 vessel.
Inadequate tissue means the specimen contained insufficient structure for pathological diagnosis by the pathologist.
The post-biopsy complications were hematuria, perinephric hematoma, required transfusion of blood component, required renal angioembolization and nephrectomy.
Data collection
This study was approved by the Institutional Review Board of Navamindradhiraj University (IRB 160/60) and registered to Thailand clinical trial registry (TCTR20181024002). We reviewed renal biopsy database focusing on patient characteristics, laboratory data (blood urea nitrogen (BUN), creatinine, estimated glomerular filtration rate (eGFR), hemoglobin, hematocrit (Hct), platelets and coagulogram), biopsy indications, biopsy complications and therapeutic procedures to manage complications. Pathological reports were reviewed to evaluate outcomes.
Statistical analysis
Considering that mean of total glomeruli was a continuous outcome and assuming mean of total glomeruli would be 40% higher in RBx than BBx (15.4 vs 11). We estimated that 88 patients per group would need to be enrolled to provide 90% power at a two-sided alpha level of 0.05.
For the statistical analysis, R version 3.4.4 (R Foundation for Statistical Computing, Vienna, Austria) was used. We compared patient characteristics, outcomes, and complications between the two groups. For continuous variables, normality test of Kolmogorov–Smirnov was performed to confirm that the samples were normal distribution or not. The student’s t-test was used if normal distribution data, and Mann–Whitney U test was used if non-normal distribution data. The chi-square and Fisher’s exact test were used for categorical variable analysis. We analyzed the multivariable logistic regression to find the factors associated with adequate kidney biopsy tissue and post-biopsy bleeding complications. We chose the risk factor from the univariable model if the p value < 0.3.
Results
We performed 246 renal biopsies in 42 months. Forty-two renal biopsies were excluded because of incomplete data. Of 204 renal biopsies, 169 (82.8%) were native renal biopsies and 35 (17.2%) were transplanted renal biopsies. Patients who had renal biopsy by RBx numbered 104 patients and 100 had biopsy by BBx. There were no significant differences in the demographic data, clinical features or pre-biopsy laboratory data based on biopsy technique (Table 1). The median age was 41 years old (quartile 1 (Q1)-quartile 3 (Q3); 31–53) and females were 56.4%. The first three-common comorbidities were type 2 diabetes mellitus, hypertension, and systemic lupus erythematosus. The median creatinine and estimated eGFR were 1.72 (Q1-Q3: 0.96–2.64) mg/dL and 42 (Q1-Q3: 24.5–78.5) mL/min/1.73 m2, respectively. The first three common indications for native renal biopsy were nephrotic syndrome (27.9%), glomerulonephritis (23.7%), and isolated proteinuria (23.1%). Allograft dysfunction was the primary indication for transplant renal biopsy.
Baseline characteristics, clinical features and pre-biopsy laboratory data.

AKI: acute kidney injury; BUN: blood urea nitrogen; BBx: blind percutaneous renal biopsy; CKD: chronic kidney disease; DM: diabetes mellitus; eGFR: estimated glomerular filtration rate; Hb: hemoglobin; INR: international normalized ratio; n: number per group; Q1: the first quartile; Q3: the third quartile; RBx: real-time ultrasound-guide percutaneous renal biopsy; SLE: systemic lupus erythematosus; SD: standard deviation.
The average number of total glomeruli with RBx (median 19, Q1-Q3: 11.8–27) was significantly more than with BBx (median 12, Q1-Q3: 7.8–21.3) (p < 0.001) (Table 2). RBx showed greater efficacy for both native and transplant renal biopsy. For completely adequate tissue definition, RBx achieved 47 (45.2%) specimens from 104 specimens, which was significantly better than the 16 (16%) (p-value < 0.001) specimens from BBx. RBx also achieved more adequate tissue than BBx (75% vs 50%; p-value < 0.001). Moreover, BBx had significantly more inadequate tissue specimens (16, 16%) than RBx (p-value < 0.001). Bleeding complications were not statistically different in terms of hematuria (p-value = 0.215) and hematoma (p-value = 0.445) (Table 3). The frequency of blood transfusion was the same for both groups (p-value = 0.949). No patient was sent for embolization or nephrectomy and no biopsy-related deaths occurred.
Comparing outcomes of two techniques.

BBx: blind percutaneous renal biopsy; Q1: the first quartile; Q3: the third quartile; RBx: real-time ultrasound-guide percutaneous renal biopsy.
Comparing biopsy complications of two techniques.

BBx: blind percutaneous renal biopsy; n: number per group; RBx: real-time ultrasound-guide percutaneous renal biopsy.
After we analyzed the univariable and multivariable logistic regression, RBx was the only factor significantly associated with adequate biopsy tissue (odds ratio (OR): 5.46; 95% confidence interval (CI): 2.66–11.24; p-value < 0.001) (Table 4). We also did logistic regression to find factors associated with bleeding complications, which means a composite of any hematuria or hematoma, or need for blood transfusion (Table 5). After multivariable logistic regression was analyzed, the lower Hct (increase 1% of Hct: OR 0.90; 95% CI: 0.83–0.98; p-value = 0.014), lower eGFR (increase 1 mL/min/1.73 m2 of eGFR: OR 0.98; 95% CI: 0.96–1.00; p-value = 0.026) and female (OR 2.87; 95% CI: 1.03–7.98; p-value = 0.043) were found to be significantly associated with bleeding complications.
The univariable and multivariable logistic regression for association between biopsy data and complete adequate kidney tissue.
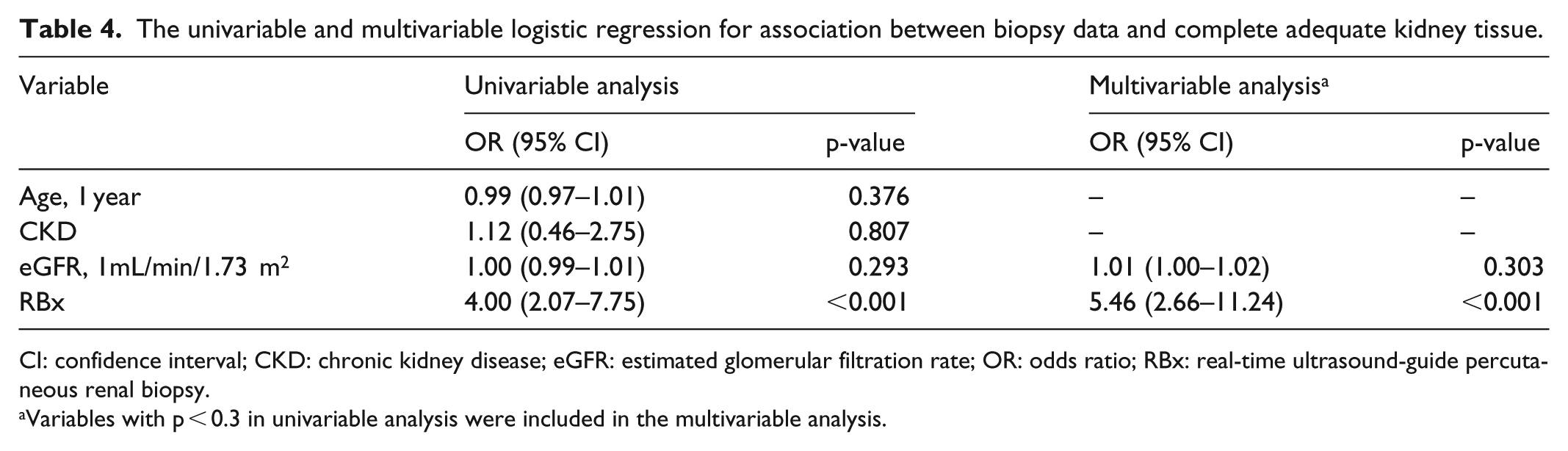
CI: confidence interval; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; OR: odds ratio; RBx: real-time ultrasound-guide percutaneous renal biopsy.
Variables with p < 0.3 in univariable analysis were included in the multivariable analysis.
The univariable and multivariable logistic regression for association between biopsy data and bleeding complications.

CI: confidence interval; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; Hct: hematocrit; PT: prothrombin time; OR: odds ratio; RBx: real-time ultrasound-guide percutaneous renal biopsy.
Variables with p < 0.3 in univariable analysis were included in the multivariable analysis.
Discussion
This study compared the two biopsy techniques that are still being performed in developing countries. We found that real-time ultrasound-guided percutaneous renal biopsy was superior to blind percutaneous renal biopsy in terms of the number of total glomeruli and adequacy of biopsy tissue. Bleeding complications were not significantly different for both techniques. We found that only RBx was a factor associated with adequate tissue. Bleeding complications were associated with lower hematocrit, lower eGFR, and being female but were not associated with biopsy technique. There was no association between the renal biopsy technique and bleeding complications.
The previous study from Maya et al. 9 reported real-time ultrasound-guided biopsy with 18-G automated biopsy needle obtained more glomeruli than the blind technique with 14-G Tru-cut biopsy needle, 18 ± 9 versus 11 ± 9 (p-value = 0.0001) respectively. Likewise, Cozens et al. 12 observed the diagnostic yield from real-time ultrasound-guided biopsy with 18-G automated biopsy needle was greater than with the blind technique with 15-G Tru-cut biopsy needle. The results were the same as our study even though our BBx was performed with a 16-G automated loaded biopsy needle. The study from Riehl et al. 10 compared two different biopsy needles, 14-G Tru-cut and automated biopsy needle, using blind technique and found that the efficacy was not significantly different. The explanation of the superiority of RBx may be related to real-time renal visualization during the renal biopsy. In contrast, Bataille et al. compared five renal biopsy techniques by retrospective review of five centers that had different routine practice. They found the number of glomeruli was equal in the center that performed the blind biopsy with a 14-G automated biopsy needle, and the center that performed the real-time ultrasound-guided biopsy with the 14-G automated biopsy needle, while the center that performed the real-time ultrasound-guided biopsy with the 16-G automated biopsy needle had lower mean number of glomeruli. The centers, however, which performed the renal biopsy by blind technique did not obtain more renal core tissue than the centers that performed real-time ultrasound-guided technique. 11 This result was also observed from our study that BBx resulted in more inadequate tissue than RBx. Whereas, the study from Kim et al. 7 also reported a lower mean number of glomeruli in RBx with the 18-G biopsy needle, when compared to BBx with 14-G Tru-cut biopsy needle. Interestingly, Chung et al. 15 reported the number of glomeruli was greater when obtained by nephrologists rather than radiologists, and this was not associated with biopsy technique. The difference of efficacy among the studies might be related to physician experience and the needle size of renal biopsy.
Our study showed a higher frequency of post-biopsy hematuria (7.8%) than in some previous studies.4,5 However, the study from Esposito et al. 16 reported minor complication (arteriovenous fistula, minor hematoma spontaneously reabsorbed, gross hematuria, post-procedural hypotension) from RBx with 14-G biopsy needle by young trainee nephrologist was 17.3 percent and that was not different from experienced nephrologist. The several studies reported that the post-biopsy bleeding complications were lower in RBx.6–9 However, BBx in those studies was performed with the larger diameter and the Tru-cut biopsy needle, which was associated with more bleeding complications.4,10,14 This was unlike our study, in which we performed the biopsy with the 16-G automated biopsy needle for both techniques, so the results of bleeding complications were not significantly different.
Tondel et al. 5 analyzed the Norwegian Kidney Biopsy Registry from 1988 to 2010 (total 9288 native renal biopsies) and reported the major risk factors for major post-biopsy complications (blood transfusion, surgery and/or arterial embolization) were reduced eGFR and small clinical center size. Furthermore, the lower eGFR associated with bleeding complications was also confirmed by our study. A study from Sweden included 1001 native and transplant renal biopsies; they found women (OR 2.2; 95% CI: 1.3–3.7; p-value = 0.002), right-sided kidney, lower body mass index (BMI) and younger age were greater risk factors for major post-biopsy complications. 17 Some results from meta-analysis showed being female was one of the risk factors for hematuria and blood transfusion after real-time ultrasound-guided native renal biopsy. 4 We also found females had higher risk for bleeding complications which may be related to being female, having lower BMI, or kidney size was smaller than males. An association between lower hemoglobin and major bleeding was also reported. 9 We observed that every 1% decline of hematocrit increased the risk of bleeding complication by about 11%.
The strength of our study is two techniques were compared by using the same sizes and types of biopsy needle. Limitations of this study include its retrospective nature. Some important data were not recorded, such as BMI, weight, height, and number of needle passes. In our hospital renal biopsy was performed by renal fellows. First-year renal fellows come to our hospital every year. In the early period of their new renal fellowship, they need to gain experience for renal biopsy under supervision by nephrology staff. Although the results might be confounded by operator experiences, the first-year renal fellows performed both techniques. This may imply that RBx is simple to perform by inexperienced operators due to the kidney and biopsy needle being visualized during operation. In contrast, the BBx must be performed by a confident and experienced operator.
Although RBx requires to add-on infrastructures such as sterile coverage and biopsy guide, its diagnostic yield is superior to BBx. Infrastructures of RBx add more cost, however, these are inexpensive and can be afforded by developing countries. Therefore, we encourage to perform RBx. On the other hand, BBx is still acceptable without higher complications in limited resources. Female gender, anemia and low eGFR should caution biopsy-performers to be aware of post-renal biopsy complications.
Conclusion
Our study confirms that the diagnostic yield of RBx is superior to BBx. The resulting complications are the same for both techniques.
Footnotes
Acknowledgements
The authors thank all nurses and staffs in the Department of Medicine, Faculty of Medicine, Navamindradhiraj University and Vajira Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of Navamindradhiraj University (IRB 160/60).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Navamindradhiraj University.
Informed consent
Informed consent was waived by Institutional Review Board.
Trial registration
Thailand Clinical Trial Registry (TCTR20181024002).