
Abstract
Objective:
Explore the characteristics of parathyroid injury during thyroid surgery and the potential for sonography to reduce the risk of parathyroid injury.
Methods:
Retrospective analysis was conducted on 39 patient cases, with parathyroid injury (including 29 cases of total thyroidectomy plus central lymph node dissection and 10 cases of total thyroidectomy). Sonography and related medical laboratory testing were performed pre- and postsurgery. Clinical symptoms and associated postsurgical gland changes were compared and analyzed according to the relevant laboratory values.
Results:
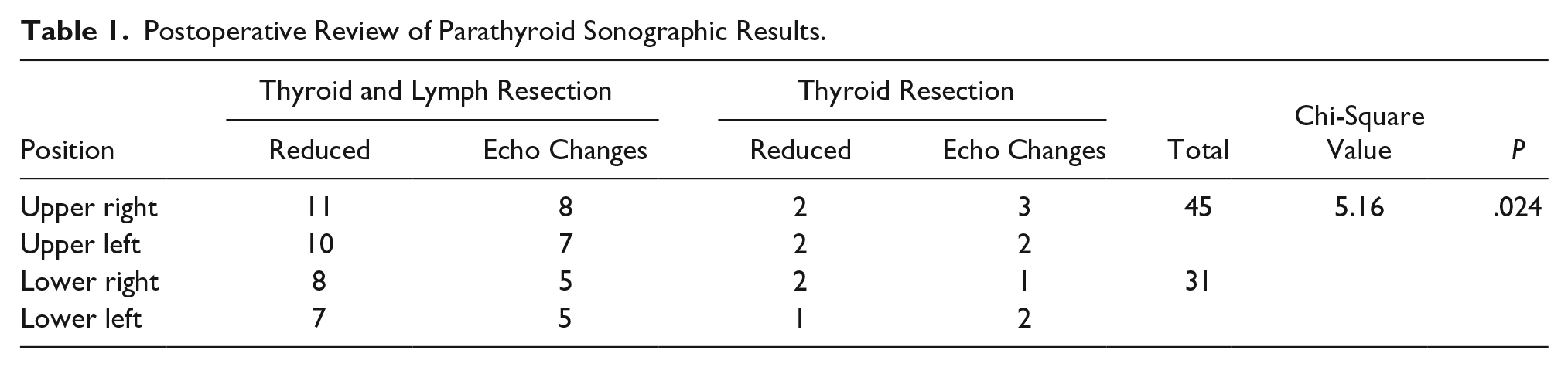
The patient case review demonstrated that the total number of glands decreased by 43 compared with preoperation, with 25 glands in the upper pair and 18 glands in the lower. There were 33 glands with uneven echo and blurred edges, with 20 in the upper pair and 13 in the lower pair. The damage rate of the upper gland (45/76) was higher than that of the lower gland (31/76) (P < .05). A total of 69.7% (23/33) of gland blood flow signals were reduced compared with preoperation, of which 10 showed uneven enhancement when the contrast-enhanced ultrasound reached its peak.
Conclusion:
Thyroid surgery can easily damage parathyroid glands, especially during a total thyroidectomy, with lymph node dissection. Sonography of the parathyroid glands in patients with postoperative hypocalcemia can provide imaging surveillance and mitigate the damage of these glands postsurgically.
Hypoparathyroidism, caused by surgical injury of the parathyroid glands, is referred to as hypoparathyroidism syndrome (HP). HP has varied clinical manifestations such as increased neuromuscular excitability, hypocalcemia, hyperphosphatemia, decreased parathyroid hormone (PTH), hand-foot convulsions, and epileptic seizures. Hypocalcemia is a common symptom after thyroidectomy. Accurate prediction and proper management may help reduce the incidence and length of hospital stay. Many studies1–3 have analyzed the biochemical and clinical predictors of hypocalcemia after thyroidectomy to find a suitable treatment for hypocalcemia after thyroidectomy. The purpose of this study was to analyze parathyroid injury from the perspective of sonography and to provide a reference for clinicians by detecting the related blood biochemical indexes of patients. This article summarizes the cases of parathyroid gland damage caused during surgery, based on a patient case review that spanned 10 years of clinical practice.
Methods
A total of 39 patients with parathyroid damage (total thyroidectomy plus neck lymph node dissection in 29 cases, total thyroidectomy in 10 cases) were selected for review, based on surgeries conducted from 2008 to 2018. Both preoperative and postoperative sonograms, with related laboratory examinations, were performed.
Instruments and Methods
The SuperSonic Imagine Aixplorer (Aix-en-Provence, France) ultrasound equipment, with a 15- to 4-MHz transducer, was used to examine all the patients. The patients were examined in the supine position, with a pillow under the shoulder and the head tilted back to fully expose the front of the neck. The patient’s head was tilted to one side only when it was deemed necessary. The scanning range was from the mandible down to the suprasternal fossa, with both sides laterally scanned to include the common carotid artery. Using the thyroid gland, the parathyroid glands were anatomically divided into the upper right region, the lower right region, the upper left region, and the lower left region. Sonographic images, including the parathyroid glands, were screened using a one-by-one image exclusion method. Data were recorded based on parathyroid location, size, boundary, internal echo, and vascular perfusion. The number and sonographic changes of parathyroid glands, before and after surgery, were compared and analyzed. In addition, contrast-enhanced ultrasound (CEUS) with SonoVue (Bracco Sine Pharmaceutical, Shanghai, China) contrast media was added for further diagnostic evaluation. The CEUS evaluations were made with a Philips (Eindhoven, the Netherlands) IU-22 ultrasound equipment and a L3-9 MHz transducer. The contrast media were vigorously mixed with 5 mL of 0.9% saline injected into the SonoVue powder. The patients were injected with 2.0 mL of contrast media via an elbow vein. The contrast bolus and the time were recorded, with the scan lasting no less than three minutes.
The review was also based on biomarkers with the following normal reference standards: blood calcium, 2.1 to 2.6 mmol/L; blood phosphorus, 0.8 to 1.6 mmol/L; and PTH, 12 to 65 pg/mL. For hypocalcemia, serum calcium after thyroidectomy was less than 2.0 mmol/L. For hypoparathyroidism, parathyroid hormone was below 15 ng/L 15 minutes after thyroidectomy. 2
Statistical Analysis
The data were statistically analyzed with SPSS software version 17.0 (SPSS, Inc, an IBM Company, Chicago, Illinois). The value of postoperative biochemical indexes was expressed as mean ± SD. The chi-square test was used to compare the rate of parathyroid number. P <. 05 was considered statistically significant a priori.
Results
The cohort reviewed included 17 men and 22 women, aged 20 to 65 years, with an average age of (45 ± 3.4) years. The cohort’s preoperative blood calcium, phosphorus, and PTH examinations were in the normal range. During the operation and 6 months postoperation, there were differing degrees of hypocalcemia. The lowest calcium value was 1.4 mmol/L. It is of note that significant clinical manifestations included 2 cases of intraoperative convulsions, 19 cases of frequent spasms of calf muscles in the first month after operation, and 18 cases of numbness of upper limbs and mouth.
Postoperative Reexamination Sonography Results
Preoperative sonography demonstrated one to four parathyroid glands in various forms of high echogenicity and slightly higher in all of these cases (Figure 1). From 2 weeks to 3 months postoperatively, the total number of parathyroid glands was reduced by 43 (25 for upper glands and 18 for lower) compared with preoperative sonography, and the echogenicity of 33 glands was inhomogeneous and low resolution (20 for upper glands and 13 for lower) (Figure 2). The injury rate of the upper glands (45/76) was higher than that of the lower glands (31/76). Chi-square value was 5.16, with P = .024. (See Table 1 for sonographic changes and positions of the parathyroid glands postoperation.) Color Doppler showed that 69.7% (23/33) of the glands with varied echogenicity had reduced blood flow signals compared with the preoperation. There was no significant improvement in blood flow signals in glands after 3 months of follow-up (Figure 3). Ten glands examined with CEUS demonstrated uneven enhancement within 21 to 48 seconds after injection.
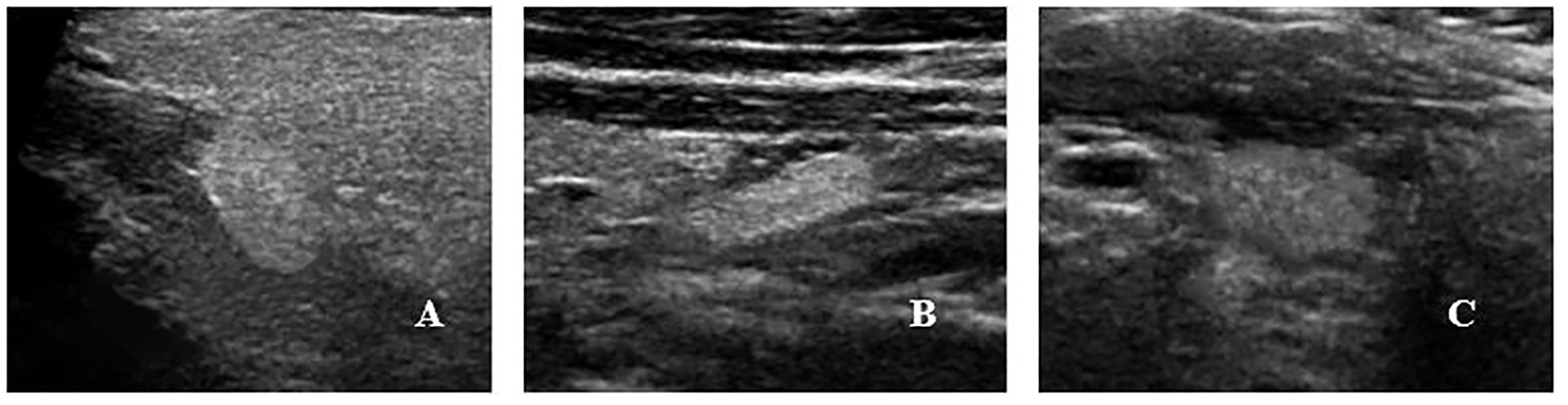
Preoperative normal parathyroid gland with multiple forms of high echo and slightly higher echo node.
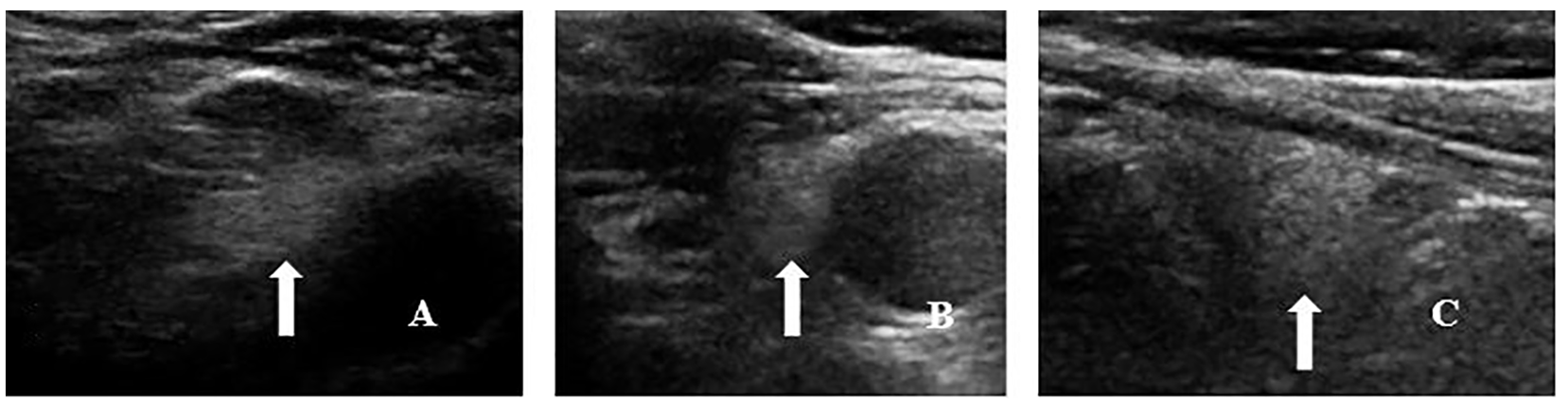
The boundary of the parathyroid gland after operation is unclear and the echo is not uniform (white arrow). (A) Ultrasonography two weeks after operation. (B) Ultrasonography one month after operation. (C) Ultrasonography two months after operation.
Postoperative Review of Parathyroid Sonographic Results.
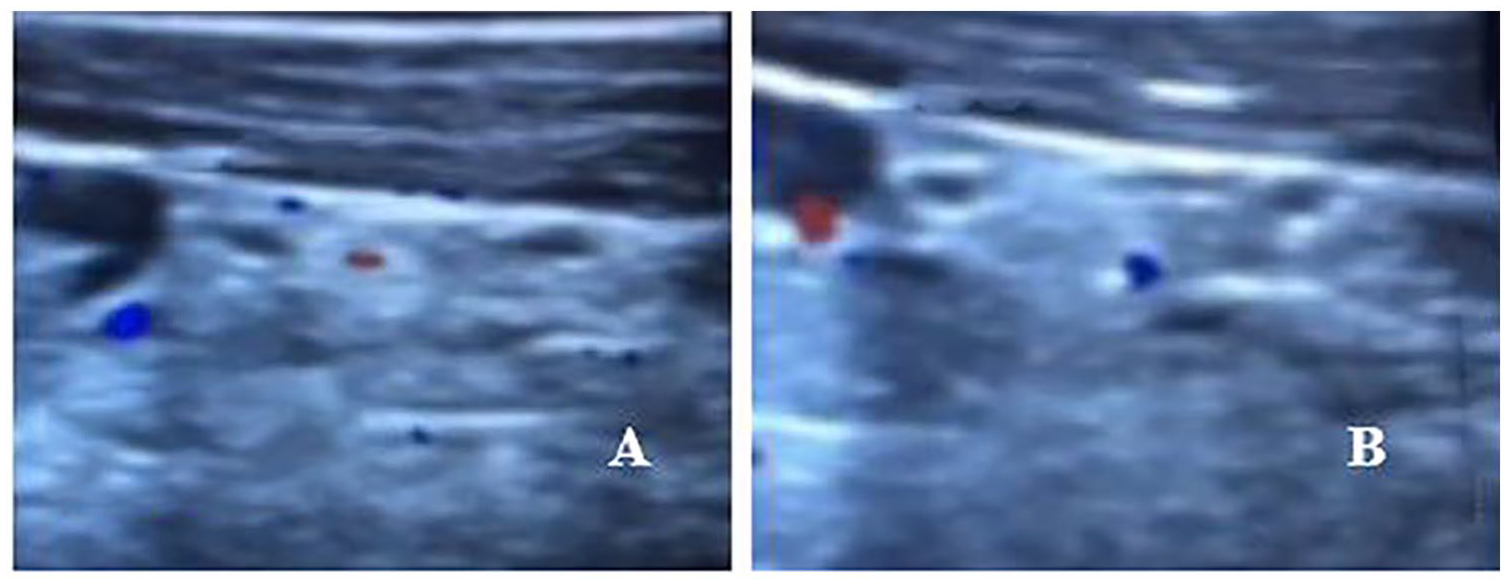
Decreased blood flow signal of parathyroid gland after operation. (A) One month after operation, only fine strips of blood flow signal could be seen in the gland. (B) Three months after operation, punctate blood flow signals could be seen in the gland.
Related Blood Biochemical Results
All patients undergoing thyroid surgery had blood calcium-, phosphorus-, and PTH-related biochemical examinations. These biomarkers were taken more than four times from the time of surgery to one year afterward. Two patients had documented intraoperative convulsions during total thyroidectomy and neck lymph node dissection. In addition, these patients had immediate blood calcium of 1.4 mmol/L and 1.6 mmol/L. The blood calcium was still less than 1.9 mmol/L after one year of nondrug treatment. The remaining 27 patients had hypocalcemia of varying degrees within 3 months after the operation, with the lowest calcium level of 1.65 mmol/L. Seven patients with complete thyroidectomy had hypocalcemia of varying degrees within one month after the operation. These patients had the lowest serum calcium of 1.67 mmol/L, while two other patients had the lowest serum calcium of 1.7 mmol/L after the operation but returned to normal in a week. There were 2 cases of permanent hypoparathyroidism after having a total thyroidectomy and lymph node dissection. The serum calcium, phosphorus, and PTH were increased and decreased in different degrees in all the patients who underwent surgery. (See Table 2 for relevant blood biochemical changes and time after operation.)
Blood Biochemical Changes After Thyroid Surgery.
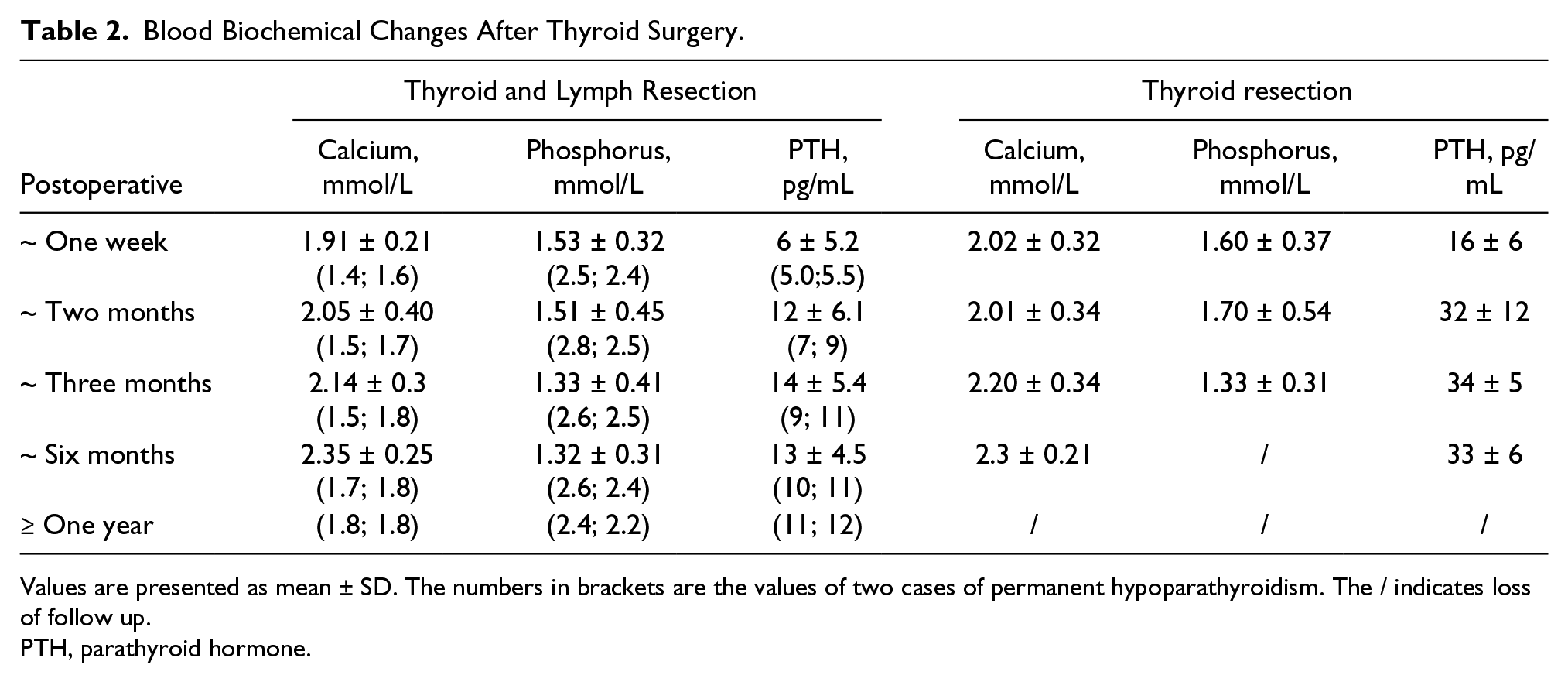
Values are presented as mean ± SD. The numbers in brackets are the values of two cases of permanent hypoparathyroidism. The / indicates loss of follow up.
PTH, parathyroid hormone.
Discussion
The parathyroid gland is an oval gland that is the size of a grain of rice or flat oval soybean shape. The parathyroid unfortunately has varied positions, and the number of these glands is not constant. Generally, the parathyroid has two pairs of upper and lower glands, located behind the lateral lobe of the thyroid gland or near the lower pole, or in the thyroid capsule or at the upper mediastinum. Normal parathyroid glands show about 77.5% to 91% with sonography.4,5 High-frequency sonography shows various forms, mostly an oval and slightly hyperechoic tubercle. During thyroid surgery, if parathyroid glands are accidentally removed or damaged, temporary or permanent hypoparathyroidism may result. A recent multicenter longitudinal study showed that the incidence of hypoparathyroidism postsurgery was as high as 28.8%. 6 The two cases of permanent hypoparathyroidism in this group of patients were reduced by four glands compared with the preoperation, with one gland in the thyroid, two in the upper third behind the thyroid, and one in the vicinity of the lower pole. In 34 cases, the number of parathyroids decreased by 1-2, mainly the upper glands, which may be adjacent to the thyroid, vulnerable to injury, or may be missed by sonographers due to anatomical changes after surgery. The incidence of temporary hypocalcemia during total thyroidectomy was 44.1%, 7 which may be related to the blood supply of parathyroid glands damaged by surgery. This would include the incorrect removal of parathyroid glands during operation. In the present study, color Doppler demonstrated a decrease in blood flow signals in glands, and contrast-enhanced ultrasound showed uneven enhancement of glands. The echo of 33 parathyroid glands in this group changed, and most of the boundaries were unclear. The decrease of blood supply may lead to the formation of cellular swelling or local small hematoma, resulting in changes in the composition of glands. Retention of two to three parathyroids in situ can significantly reduce the risk of hypocalcemia after operation. 8 Traditional total thyroidectomy leads to a higher incidence of hypocalcemia after operation, while near-infrared autofluorescence imaging (NIR) can detect the parathyroid gland during thyroidectomy, which may be helpful for early identification of parathyroid glands during thyroidectomy. 9
Conclusion
This cohort review of patient cases underscores some very important points for planning surgery with the use of sonography. On the sonogram, the upper parathyroid gland is mainly located between the true and false thyroid envelope near the isthmus level (behind the upper third of the thyroid gland), while the lower parathyroid gland is located within 2 cm below and behind the lower third of the thyroid gland, near the blood vessels under the thyroid. 4 Sonography of the parathyroid glands before total thyroidectomy can provide the surgeon with the approximate location and number of glands and may prevent the resection of parathyroid glands in thyroid. Sonography of the parathyroid glands in patients with hypocalcemia after thyroidectomy can determine the number of gland injuries, the presence or absence of hematoma compression, and blood supply damage.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Shijiazhuang Science and Technology Research and Development Guidance Plan (the first batch). Item number: 181460443.