
Abstract
This case study describes six sonographic findings, with correlative imaging, in an adult patient with congenital Madelung deformity. Two are typical of congenital Madelung deformity: a thick volar hyperechoic band extending from the ulnar side of the distal radius toward the lunate-triquetrum area, the so-called Vickers ligament, adjacent to the radiotriquetral ligament, and a cortical defect on the ulnar and volar side of the distal radius. Other findings may be also observed, such as a narrowed distance between the Lister tubercle and the distal radioulnar joint, a dorsal subluxation of the ulnar head, an extensor tendons entrapment and pronator quadratus modifications. Although the diagnosis of congenital Madelung deformity is based usually on clinical examination, this rare malformation may remain undiscovered until adulthood. When sonography is used as the first imaging technique, the sonographic findings of congenital Madelung deformity can facilitate diagnosis and the appropriate radiographs.
Congenital Madelung deformity (CMD) is a rare pathology involving less than 2% of the general population and results from an asymmetric growth failure of the distal radius, triggered by genetic factors and by two contiguous aberrant hypertrophic volar ligaments that cross the distal metaphysoepiphyseal region of the radius. 1 The first, the Vickers ligament, is tied between the ulnar and volar sides of the radial notch and the volar pole of the lunate. 2 The second, the radiotriquetral ligament, adjacent to the Vickers ligament, is tethered between the ulnar and dorsal side of the radial notch and the volar pole of the triquetrum, with variable extensions to the adjacent ligaments as well.3,4 CMD is usually bilateral and diagnosed during childhood, especially when associated with Leri-Weill and Turner syndromes, or with other congenital or hormonal disorders, such as multiple enchondromatosis (Ollier disease), multiplex dysostosis in mucopolysaccharidosis, or pseudo-hypoparathyroidism. 5 Less frequently, the condition may be diagnosed in adults after a minor trauma or in patients presenting with carpal tunnel syndrome, wrist pain, rotational deficiency, or extensor tendinopathy.1,6–8 CMD is important to detect even in young adults, because treatment may diminish the evolution of the deformity and weaken the development of complications. Besides other considerations, including aesthetics, diagnosis of CMD may also have genetic implications.1,2
Case Report
A 20-year-old woman of short stature was referred to the Radiology Department for ultrasonography (US) evaluation of her right wrist because of wrist deformity and moderate pain, without neurologic deficit or known trauma. At clinical examination, both wrists presented a dorsal subluxation of the ulnar heads, much more obvious on the right side than on the left one (Figure 1). US of the dorsal wrist revealed a narrowed distance between the Lister tubercle and distal radioulnar joint (DRUJ) and a thickened common extensor tendon, while the extensor tendon of the fifth finger and the extensor retinaculum appeared normal (Figure 2). US of the palmar wrist revealed a round bony defect on the ulnar side of the distal radius. Within that bony defect, a thick hyperechoic lobulated fibrillar structure that continued obliquely toward the lunate-triquetrum bones was observed (Figures 3 and 4). The pronator quadratus muscle (PQ) appeared thin, with loss of bulk and increased echogenicity, with normal adjacent flexor muscles (Figure 5). No hematoma, additional muscle, nerve abnormality, or articular effusion was detected. The deformity was bilateral, although more obvious on the right side. The diagnosis of CMD was in fact obvious on subsequent radiographs (Figure 6). After complementary wrist computed tomography arthrography (CTA) and magnetic resonance imaging (MRI), the patient was referred to an orthopedist for further evaluation, but as no surgical procedure was planned, the patient did not return.
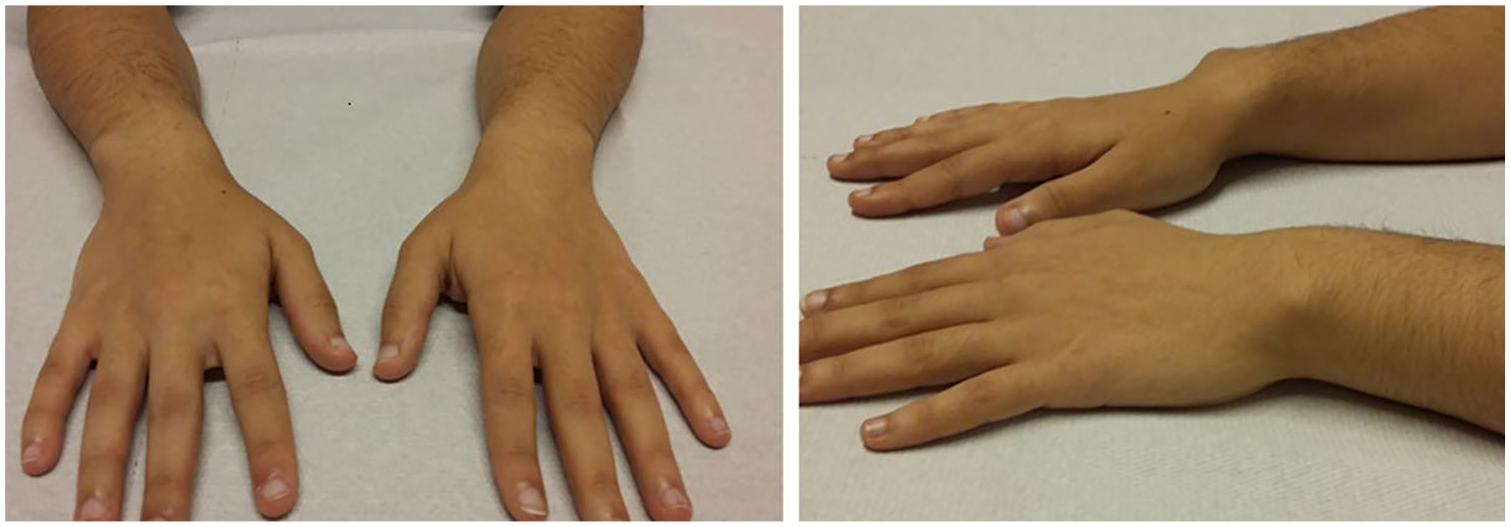
A 20-year-old woman of short stature was referred to the Radiology Department for evaluation of right wrist deformity and moderate pain, without sensory deficit or known trauma. Note bilateral dorsal subluxation of the distal ulna more obvious on the right side.
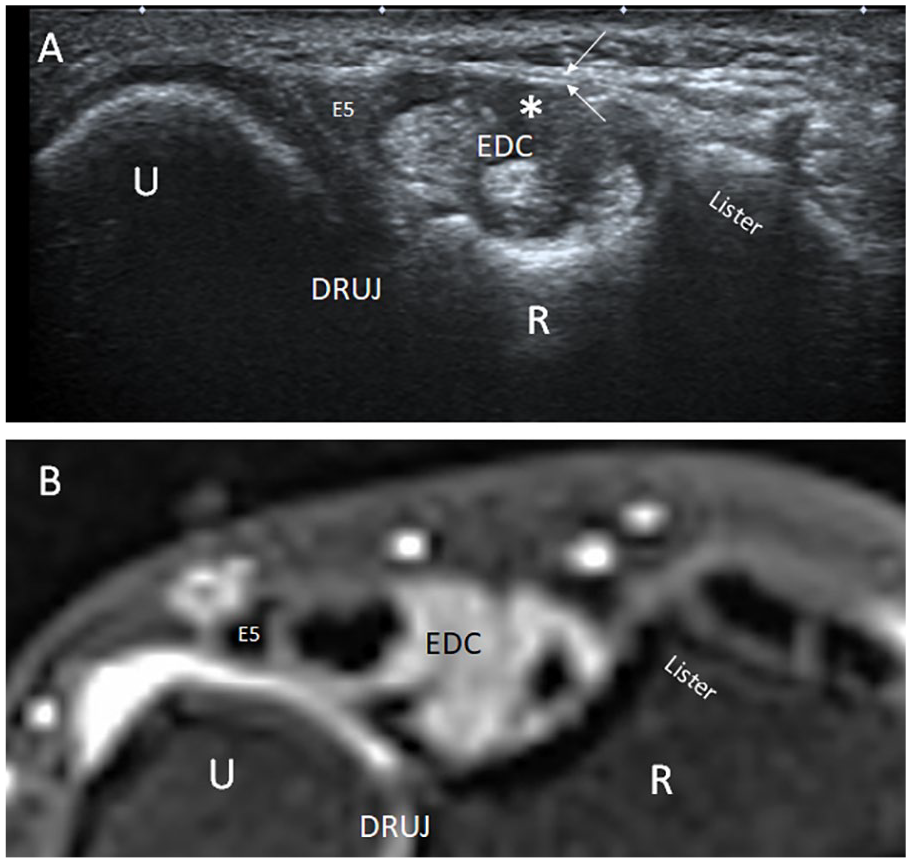
Axial sonogram (A) and reformatted axial computed tomography arthrography (B) of the dorsal right wrist at the level of the Lister tubercle illustrate dorsal subluxation of the ulna. Note the abnormally rounded and tenosynovitis of the extensor tendons of the fourth compartment (star). The extensor tendon of the fifth finger (E5) and the extensor retinaculum are normal (arrows). DRUJ, distal radioulnar joint; EDC, common extensor tendon; E5, extensor tendon of the fifth finger; R, radius; U, ulna.
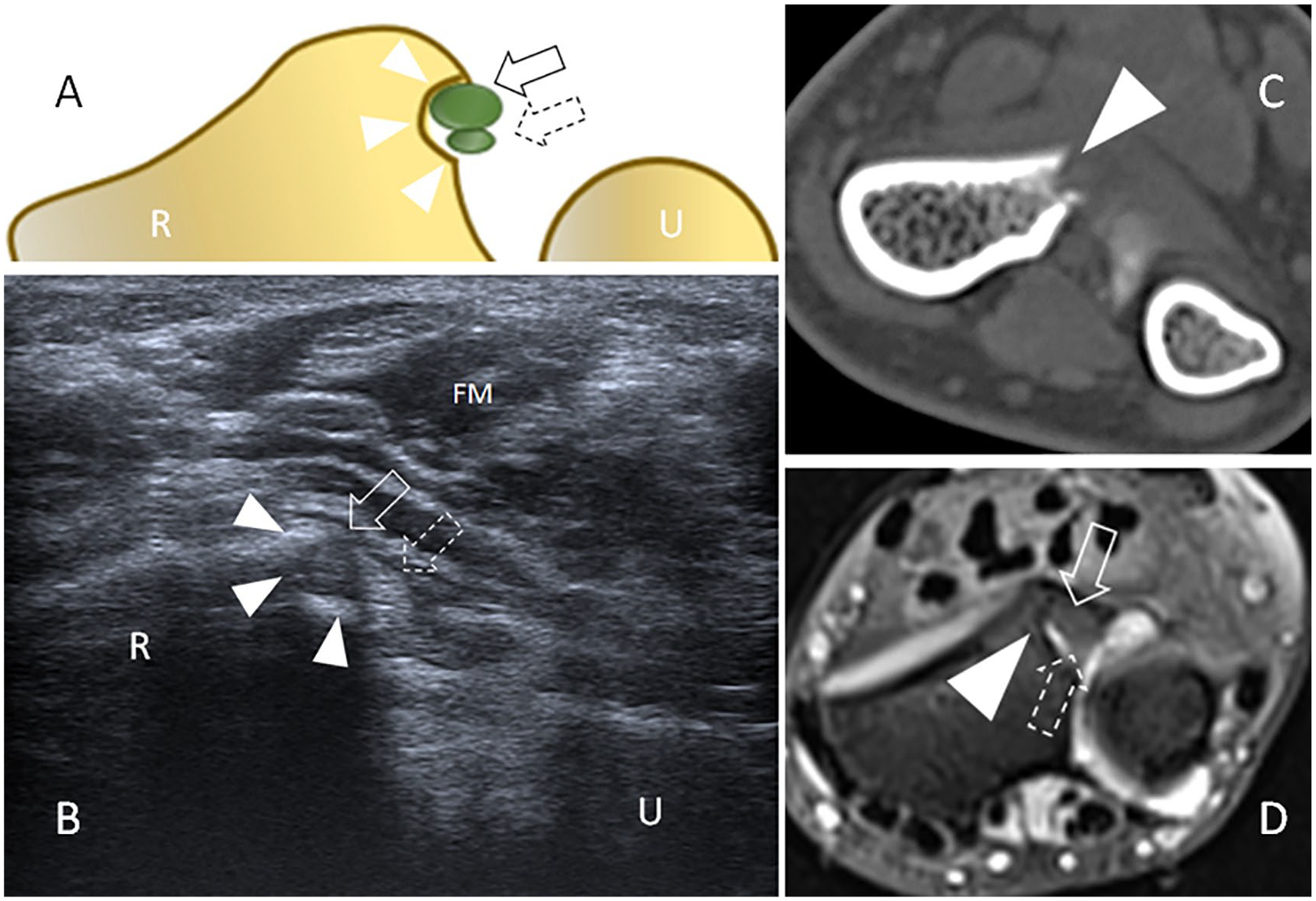
Drawing (A) and axial sonogram (B) obtained at the palmar side of the right wrist, with corresponding axial computed tomography arthrography (CTA) reconstructions (C) and axial T2-weighted fat-suppressed magnetic resonance (MR) image (D). Both CTA and MR are issued from the reported patient. Ultrasonography (US) depicts a round bony defect (arrowheads) on the ulnar side of the distal radius (R) containing the Vickers (thin arrow) and radiotriquetral ligament (dotted arrow) examined in their short axis. The Vickers ligament is most volar and radial and appears hypoechoic because of anisotropy. The radiotriquetral ligament (dotted arrows) is most dorsal and ulnar. Overall, the two ligaments display an “eight shape” configuration with a thickness of 7 to 8 mm. Although MR delineates bone and ligament abnormalities, confirming the US image, CTA represents a precise and fast modality to diagnose bone abnormalities, especially the cortical defect, that may be not always clearly demonstrated on radiographs. FM, flexor muscles; U, ulna.
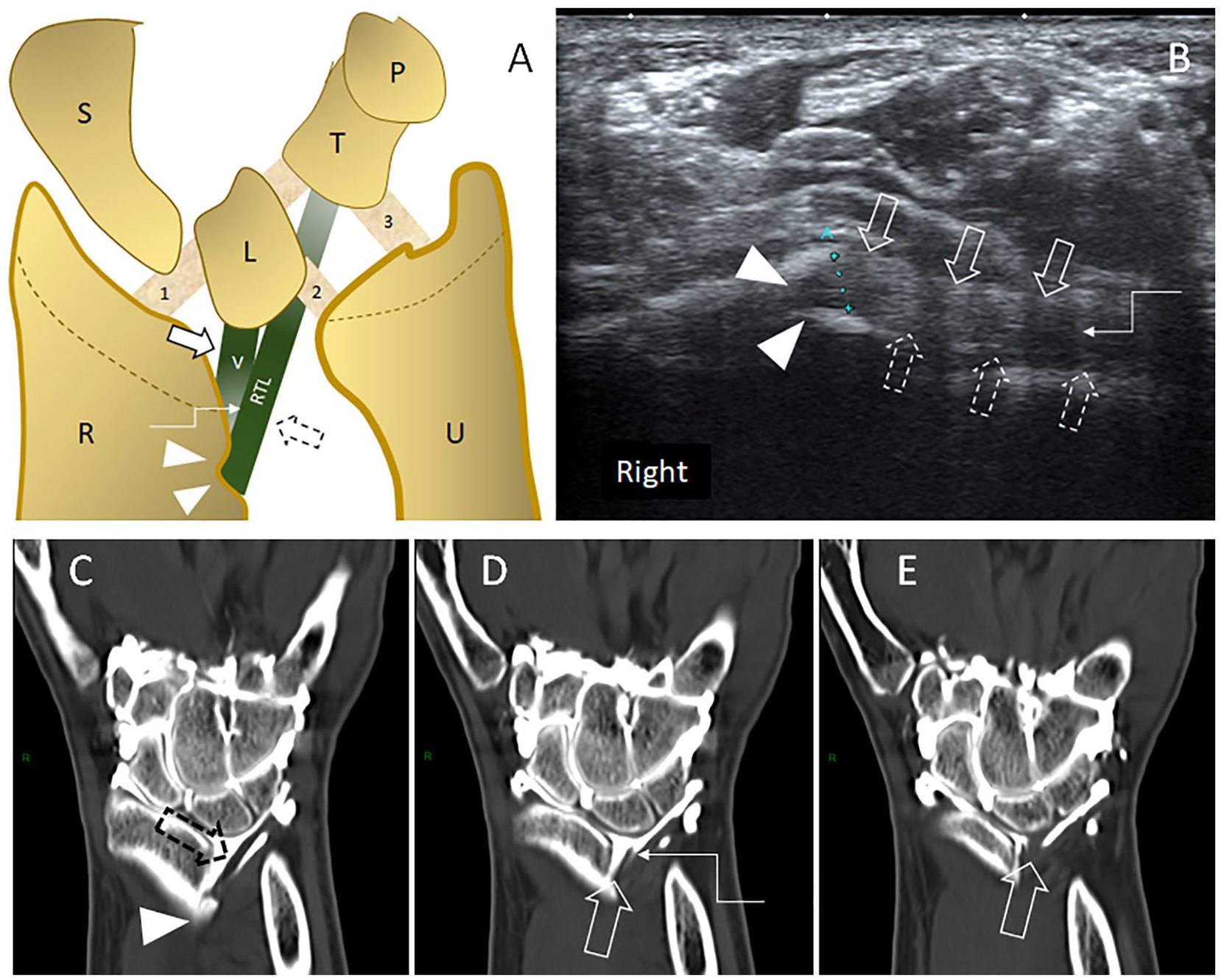
Coronal drawing (A) and sagittal oblique sonogram (B) obtained at the palmar side of the right wrist, with corresponding successive coronal computed tomography arthrography (CTA) reconstructions (C–E). Both CTA and magnetic resonance are issued from the reported patient. Ultrasonography (US) view was obtained by maintaining one end of the transducer over the cortical notch (arrowheads) and tilting the other one toward the lunate/triquetrum region. The Vickers (thin arrow) and radiotriquetral (dotted arrows) ligaments are imaged in their long axis. The two ligaments are separated by a thin cleft (step-arrow), hypoechoic on US (B), delineated by contrast material on CTA (D).
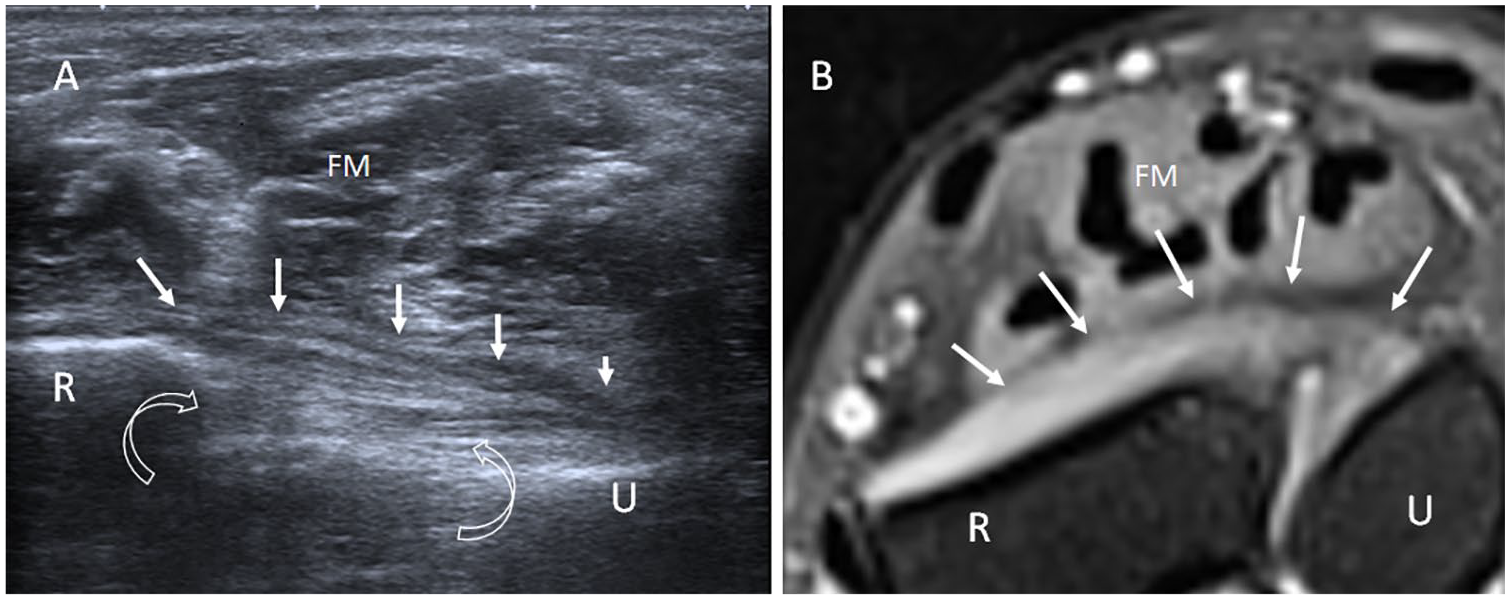
Axial sonogram at palmar side of the right wrist (A) with corresponding axial T2-weighted fat-suppressed magnetic resonance (MR) image issued from the reported patient. (B) The pronator quadratus muscle (arrows) is hypotrophic, and hyperechoic curved arrows indicate the interosseous membrane, more clearly depicted on the sonogram than on the MR image. FM, flexor muscles; R, radius; U, ulna.
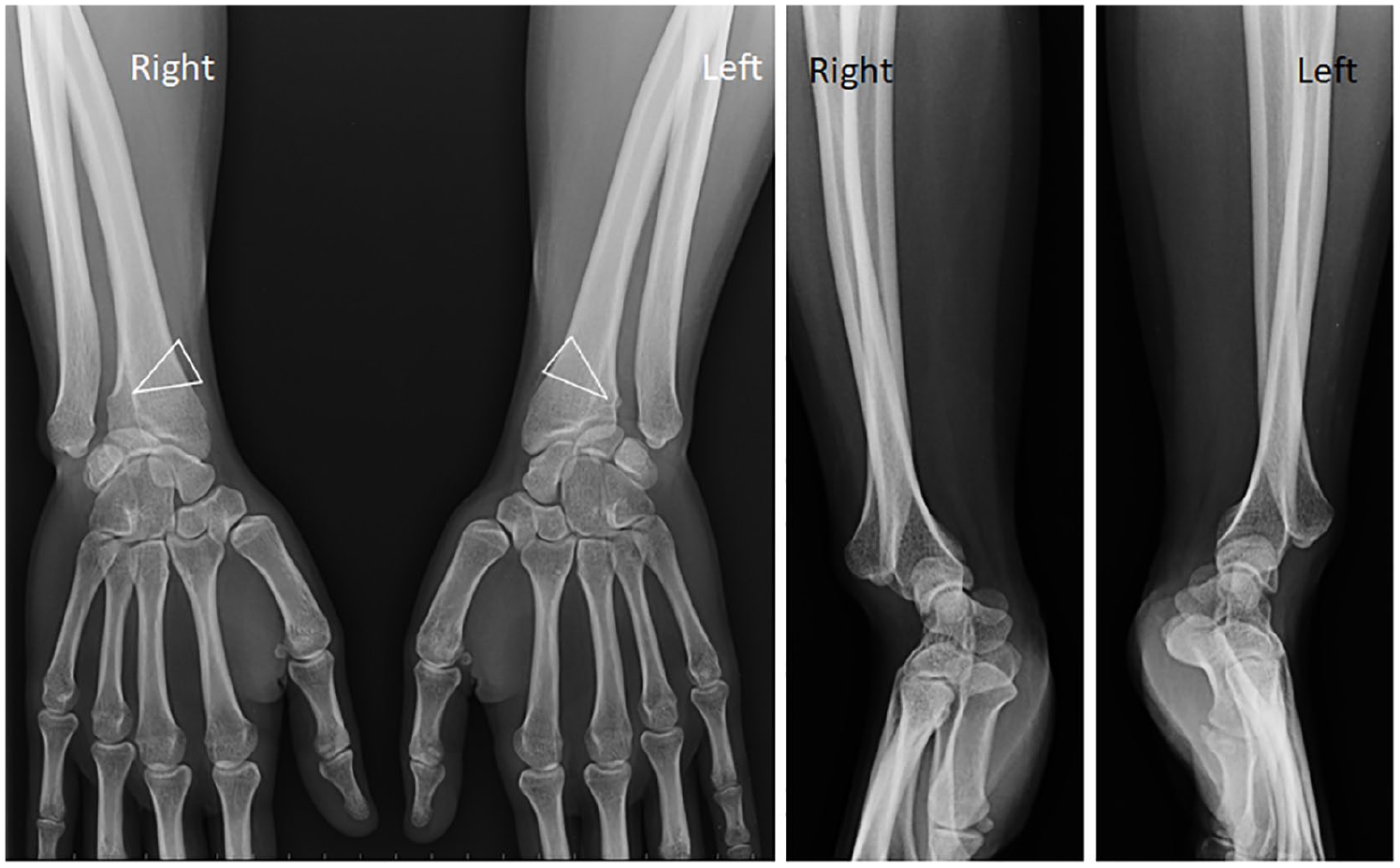
Standard radiographs show bilaterally typical findings of congenital Madelung deformity, including an increased curvature of a short radius, a long ulna with a positive variance, an ogival shape of the carpus, a distal radioulnar diastasis with dorsal subluxation of the ulna, a lunate subsidence, and a cortical notch on the ulnar side of the distal radius (arrowhead).
Discussion
Diagnosis of CMD relies classically on clinical examination and imaging studies, including radiography, wrist CTA, and/or MRI.9–11 Because CMD mostly affects young patients, MRI is preferred to CTA, but limited access and cost of MRI may represent a constraint in a routine diagnostic workup. 5 Although US cannot entirely assess the bone changes of CMD, it can accurately evaluate the associated soft tissue lesions and the superficial osseous abnormalities as well.12,13 US findings in adult CMD may be divided into primary and secondary findings. Primary findings are specifically observed in CMD, while secondary findings may also be present in other wrist pathologies, such as acquired Madelung deformity (AMD).
Primary Findings: Cortical Notch and Anomalous Volar Ligaments
The cortical notch, classically described in CMD, may be seen on a radiograph, CT, and MRI. It consists of a radiolucent area on the volar and ulnar sides of the distal metaphysis of the radius. Its definite nature is unclear. It can reflect a loss of bone due to a focal growth arrest of the ulnar portion of the distal radial epiphysis. 3 Its shape and size may vary from a small defect to a large flame-shaped area (Figures 3 and 6). Recently, in eight cases of CMD, Hanson et al. 4 used MRI to retrospectively describe an anomalous volar radiotriquetral ligament that was more visible than the Vickers ligament. Although MRI represents the modality of choice in the demonstration of wrist ligaments, US may also assess them as anisotropic echogenic bands and/or fibrillar structures.11,13 US of the volar aspect of the wrist is realized with the patient’s forearm in a supinated position. The patient sits on a chair in front of the radiologist or sonographer. The examination begins by transversal views. US demonstration of these anomalous volar extrinsic ligaments starts with the detection of the cortical notch, which can be easily made by moving the probe transversally up and down. Once the cortical notch is visualized, the two adjacent ligaments are displayed as an “eight” shape configuration, with a thickness of 7 to 8 mm (Figure 3). The two ligaments show anisotropic artifacts due to their different orientations. The most volar and radial ligament is the Vickers ligament, while the most dorsal and ulnar is the radiotriquetral ligament. 4 Then, by maintaining one side of the probe within the cortical notch and tilting the other side obliquely toward the ulna, the lunate, and triquetrum, it is possible to follow the Vickers ligament and the radiotriquetral ligament in their longitudinal axis (Figure 4). In this orientation, these ligaments are separated by a thin hypoechoic line. This line corresponds to the intermediate signal cleft observed on MRI, as described by Hanson et al. 4 in 75% of their series. However, in our patient, this cleft was hard to observe on MRI and was partially identified on coronal CTA reconstruction, probably thanks to surrounding contrast material.
Secondary Findings: Decreased Distance Lister Tubercle-DRUJ, Ulnar Head Instability, and PQ Modifications
While no criteria have been established in the literature for the normal distance between Lister tubercle and DRUJ on a transversal view, our laboratory uses 16 mm for females and 18 mm for males. In our patient, this distance was evaluated at 12 mm (Figure 2). This finding may result from the combination of factors, such as reduction of the ulnar segment of the distal radial epiphysis, increased radial bowing, volar tilting of the distal radius, ulnar rotation, and axial distortion of the carpus (Figure 6). These forearm and wrist distortions lead to functional disability. 9
Instability of the ulnar head may manifest as dorsovolar translation and may have several causes, such as the relative pronation of the distal radius and the lengthening of the ulna, which are common features of CMD (Figure 6). 5 Dorsovolar translation of the ulnar head may be evaluated by dynamic CT using the epicenter technique, but important variations are observed in the normal subject, and the method exposes the patient to radiation. 14 US was used as a screening method by Hess et al. 15 with a sensitivity and specificity of over 80%. In that study, the averaged dorsovolar translation of the pathological wrists was measured at 5.1 mm on a transversal US view at the level of the floor of the fourth extensor compartment. In our patient, the averaged translation of the ulnar head was estimated at 5 mm at rest and in a pronated position, which is abnormal (Figure 7). However, besides abnormal volar ligaments and osseous deformities, only a very small tear was observed in the radial enthesis of the triangular fibrocartilage (TFCC) in our patient. In this particular case, the ulnar head instability may be due to biomechanical alteration of the PQ, which appeared flattened and hyperechoic (Figure 5). Isolated hyperechoic PQ flattening may suggest anterior interosseous nerve entrapment but also a pronator teres dominance overriding the PQ action during forearm pronation, especially with normal adjacent flexor muscles or with an increased bowing of the radius, as observed in our patient. 16
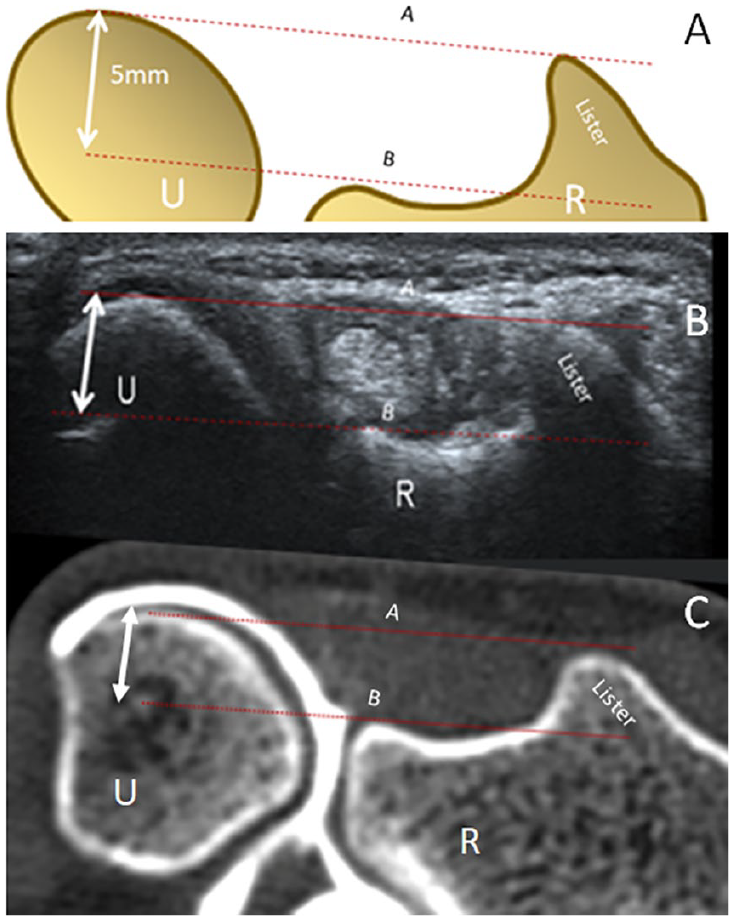
Drawing (A) and axial sonogram at the dorsal aspect of the right wrist (B) with corresponding axial computed tomography arthrography (CTA) reconstruction (C). CTA is issued from the reported patient. The images illustrate the method used to estimate the dorsal translation of the ulna. The distance between the base of the Lister tubercle and the dorsal aspect of the ulnar head (dotted line A) is measured at the level of the floor of the fourth extensor compartment (dotted line B). Dorsal subluxation of the ulnar head is estimated at 5 mm even at rest and in a pronated position, which is abnormal.
Extensor tendon rupture, more often observed in rheumatoid arthritis, is a rare condition in CMD. 17 Such severe complication usually follows tearing tendinopathy. US of the dorsal aspect of the wrist is realized with the patient’s forearm in a pronated position. As for the volar aspect of the wrist, the patient sits on a chair in front of the radiologist or sonographer. The examination begins by transversal views, with demonstration of two anatomic key structures that are the extensor retinaculum and the Lister tubercle. In our patient, the extensor tendon of the fifth finger (E5) and the extensor carpi ulnaris tendon are normal. However, the tendinopathy, involving the entire fourth compartment, may result from chronic entrapment between the tendons and the dorsally dislocated distal ulna together with the abnormal configuration of the distal radius, especially following repetitive wrist dorsiflexion (Figure 2).17,18 US may diagnose promptly tendinopathy, tears, or rupture, as treatment of rupture is usually surgical.7,19 In their systematic review, based on a retrospective analysis of 25 studies, Peymani et al. 20 describe a variety of different surgical procedures, such as combined radial lengthening and ulnar shortening, Sauvé-Kapandji procedure, and/or resection of the Vickers ligament. Genetic testing is also helpful in patients with an obscure etiology or lack of preceding wrist trauma to identify potential chromosomal aberrancies.1,20
Conclusions
The diagnosis of Madelung deformity in the adult is usually made on clinical appearance and typical radiographic appearance. In the appropriate clinical setting and when realized by an experienced sonologist or sonographer, US can diagnose CMD by demonstrating abnormal volar ligaments and cortical notch, allowing differentiation with acquired form of Madelung deformity or other wrist pathologies. In addition, US can diagnose associated severe complications of entrapment such as tendon tears or rupture. It is important to diagnose promptly this tendinopathy, which may occur in previously undiagnosed Madelung deformity. CTA and MRI can help in appreciating subtle additional or atypical findings but are expensive and invasive. Moreover, if US is the first imaging technique, awareness of the findings of CMD can facilitate its diagnosis and suggest, as a minimum, the use of standard radiographs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.