
Abstract
Left ventricular ejection fraction (LVEF) is vital to manage heart failure (HF). Studies have reported variable correlations for LVEF between echocardiography (ECHO) and single-photon emission computed tomography (SPECT). A retrospective review of 235 patients was conducted to compare LVEF via ECHO and SPECT done within 72 hours. Mean LVEF by ECHO was 51% and 57% by SPECT. A moderately positive correlation resulted (r = .76, P ≤ .05) for all, but a weak correlation was noted in 99 with LVEF of 25% to 50% (r = .43, p≤0.05). Further imaging may be needed for discordant results when medications and/or devices are considered.
Keywords
Heart failure (HF) is a major cause of mortality and morbidity in most of the world. In 2012, 2.4% people in the United States had HF. 1 HF can be classified into either HF with reduced ejection fraction (HFrEF) or HF with preserved ejection fraction (HFpEF). Treatment choice for HF is guided predominantly by symptoms and left ventricular ejection fraction (LVEF). 1
LVEF is one of the most important measurements used to evaluate HF patients. Based on the current 2013 American College of Cardiology/American Heart Association (ACC/AHA) guidelines on management of HF, measurement of LVEF is a class I recommendation for evaluating patients with HF. 1 This measurement clearly defines (1) prognosis, (2) mode of treatment with devices (implantable cardiac defibrillators [ICDs] and cardiac resynchronization therapy), and (3) types of medical therapy, such as use of neurohormonal therapy 1 and titration of chemotherapy.2,3
Currently, LVEF can be measured by an echocardiogram (ECHO), single-photon emission computed tomography (SPECT), contrast-enhanced left ventriculogram, cardiac computed tomography (CCT), and cardiac magnetic resonance imaging (CMR).4,5 None of these techniques are without problems, and all have some limitations. Up to 10% variability may be found in the LVEF by ECHO in the same examination.2,3,6 The most accurate test is felt to be CMR and is used in most studies as the “gold standard” to evaluate the accuracy of LVEF measured by other techniques.4,5 However, the expense, availability, and the inability to use CMR in patients who have pacemakers or artificial valves limit its use.
Many studies have reviewed the correlation of LVEF determined by ECHO and SPECT compared to CMR as the gold standard. Although LVEF by ECHO is the standard guideline-approved technique1,2 to measure LVEF in most HF patients, SPECT is an accepted modality to determine LVEF.1,7,8 Both ECHO and SPECT have their limitations.7,9
Multiple studies have evaluated the concordance between LVEF by ECHO and SPECT with variable findings.10–15 There does not appear to be an analysis of LVEF specifically limited to patients with a moderate reduction of LVEF between 25% and 50%.
Methods
This study was conducted in a West Virginia medical center, after the local human subjects institutional review board (IRB) approved the study. Hospital IRB was also completed prior to study execution. This was a retrospective chart review of the electronic medical records (EMRs) of 235 randomly selected patients who had undergone both ECHO and SPECT within 72 hours.
A patient population of adults older than 20 years of age who were either admitted or evaluated as an outpatient, between 2012 and 2014, was selected. Patients who had stable HF, stable coronary artery disease, structural defects of the heart, left ventricular hypertrophy, and valvular defects were included. Patients were excluded who, within the last 30 days before imaging, had a revascularization procedure, acute coronary syndrome, or acute decompensated HF.
Left ventricular end systolic and end diastolic volumes and hence LVEFs were measured by SPECT using previously validated software QGS (Mirada Medical Limited, Denver, CO) during postexercise image acquisition. 8 All 2D ECHO examinations were performed within 72 hours of the SPECT examinations using available cardiac ultrasound equipment.
Standard long-axis, short-axis, and apical views were recorded as all examinations include long-axis, short-axis, and apical two- to three-chamber views per standard protocol. LVEF was calculated using Simpson’s rule, but the LVEF was typically reported by the readers using a combination of their visual estimation and quantitative determination of LVEFs, by Simpson’s rule. All readers were certified by the American Society of Echocardiography (ASE) to interpret ECHOs.
There were no clinically significant events reported between the two studies.
Data Analysis
The statistical program SAS version 9.3 (SAS Institute, Cary, NC) was used to analyze the data. Basic descriptive statistics, such as means, standard deviations for continuous variables, proportions, and frequencies for categorical variables, were used to analyze the data. Correlations between the two parameters were analyzed using linear regression analysis. Categorical variables of interest included demographics and comorbidities. Continuous variables included age and left ventricular ejection fraction. A P value of ≤.05 was established for statistical significance. Specifically determined was the percentage of patients who had LVEF reported by either ECHO or SPECT between 25% and 50%.
Results
LVEF assessment by ECHO and SPECT was performed on 235 patients within a 72-hour period. Of the 235 patients, 99 had an LVEF between 25% and 50%. Baseline characteristics of the study groups are presented in Table 1.
Baseline Characteristics. a
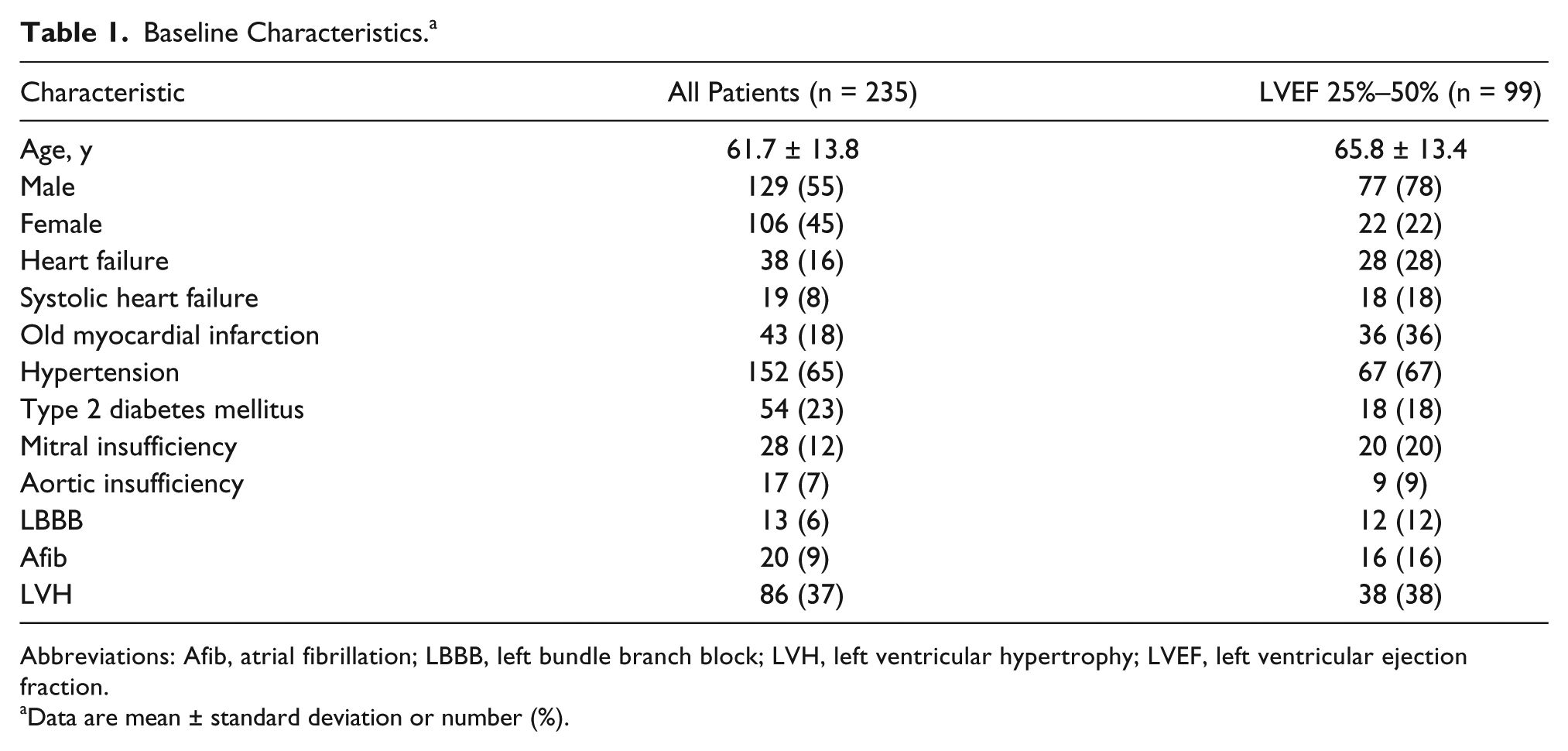
Abbreviations: Afib, atrial fibrillation; LBBB, left bundle branch block; LVH, left ventricular hypertrophy; LVEF, left ventricular ejection fraction.
Data are mean ± standard deviation or number (%).
For the overall group of 235 patients, the mean ± standard deviation (SD) LVEF measured was 57% ± 14.5% by SPECT and 51% ± 11.7% by ECHO. The linear regression analysis demonstrated a concordance between ECHO and SPECT assessments for the entire group (r = 0.76) (Figure 1).
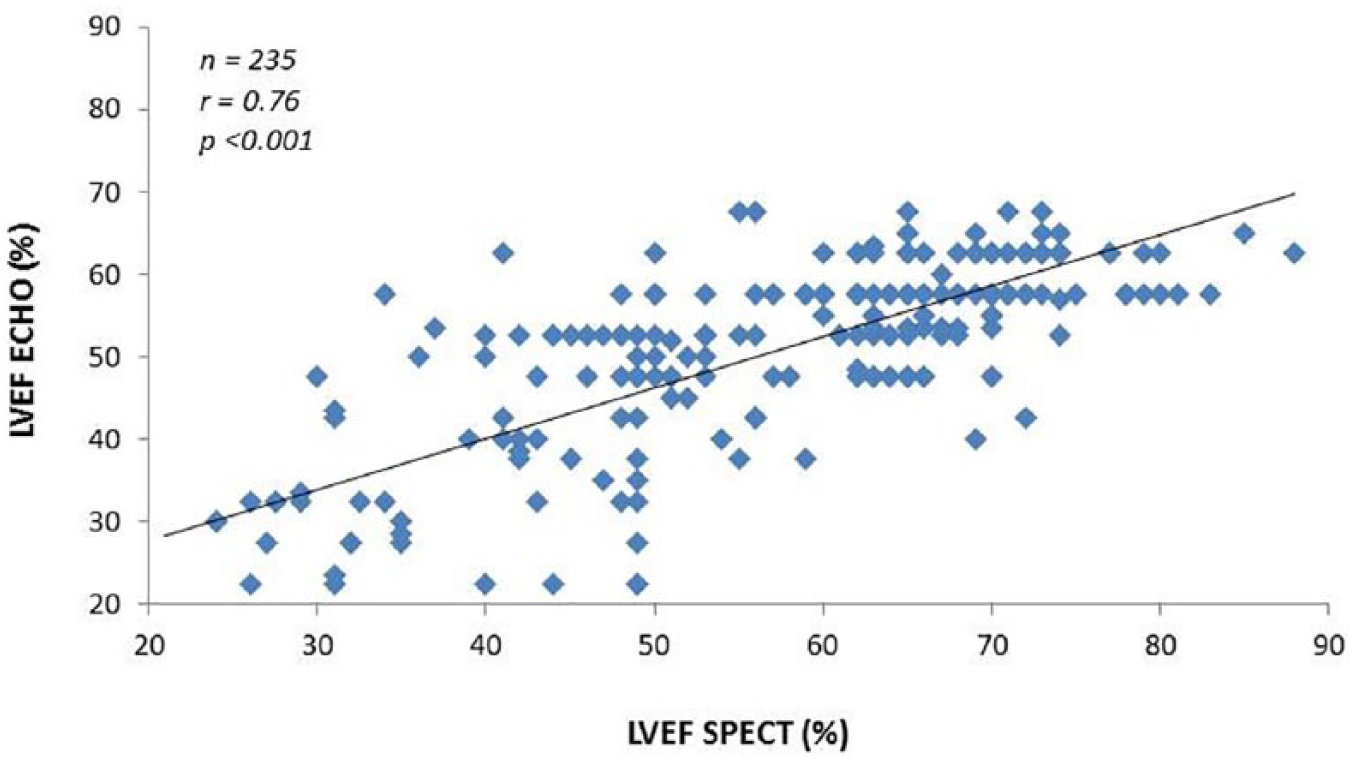
Correlation of left ventricular ejection fraction (LVEF) by single-photon emission computed tomography (SPECT) and echocardiogram (ECHO) for all patients.
No difference in concordance was noted in the correlation when either modality was interpreted by the same or a different reader (Table 2).
LVEF Measurements Between Techniques.
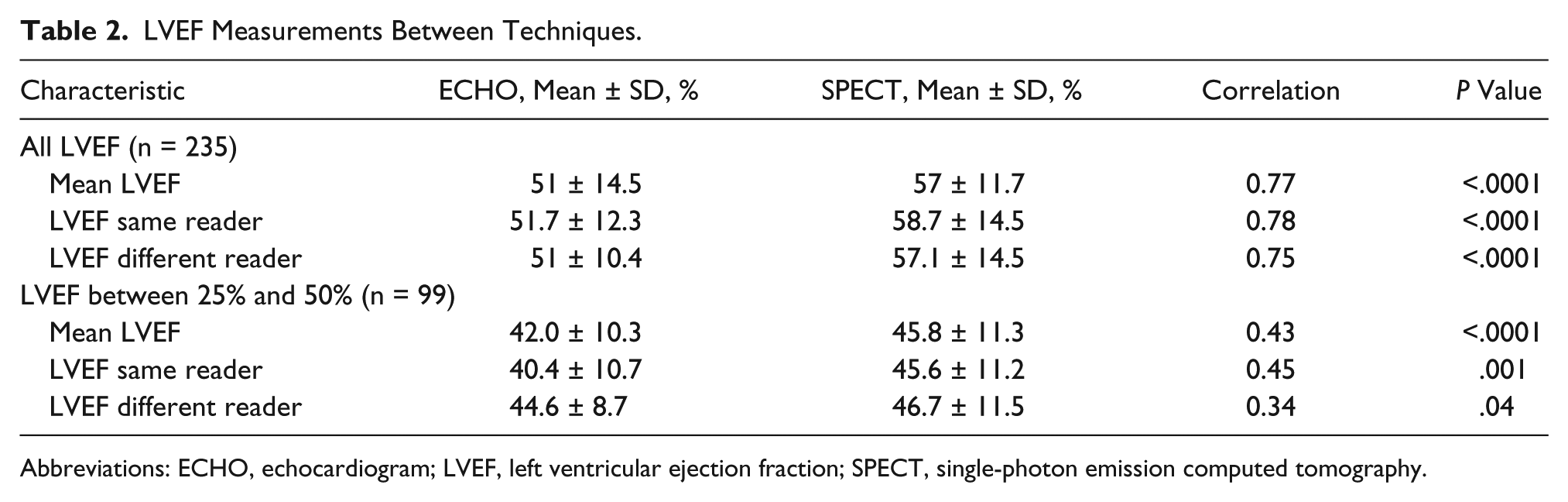
Abbreviations: ECHO, echocardiogram; LVEF, left ventricular ejection fraction; SPECT, single-photon emission computed tomography.
The subgroup of 99 patients who had LVEF between 25% and 50% by either modality showed less concordance (r = 0.43), with a mean ± SD LVEF of 46% ± 11.3% by SPECT and 42% ± 10.3% by ECHO (Figure 2).
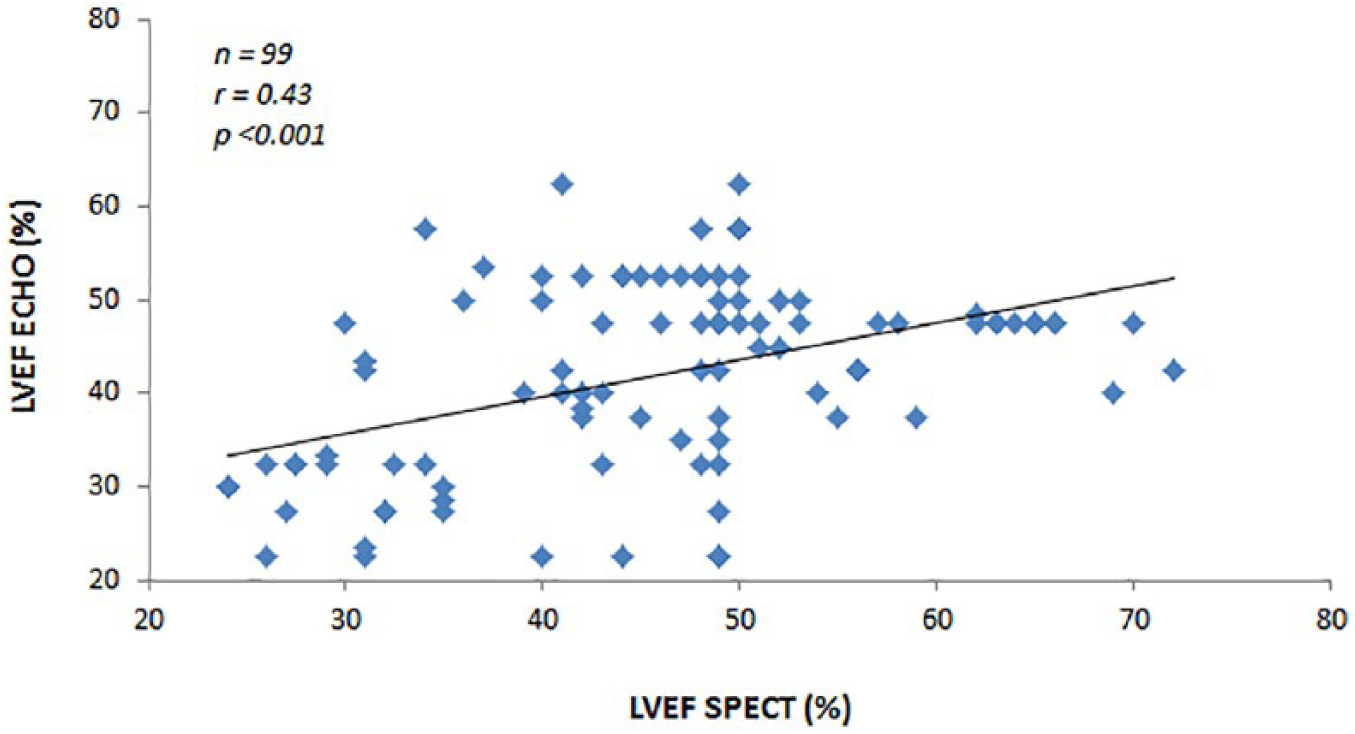
Correlation of left ventricular ejection fraction (LVEF) between 25% and 50% by either technique. ECHO, echocardiogram; SPECT, single-photon emission computed tomography.
A moderate degree of concordance was observed for LVEF measurements between the modalities when the same reader was used (r = 0.45), whereas a low degree of concordance was noted when LVEF was read by different individuals (r = 0.34) (Table 2).
Discussion
Knowledge of the potential for inaccuracies of ECHO and SPECT is needed before physicians can make important clinical decisions, which might involve placement of defibrillators and/or biventricular pacemakers, or starting medications for HF, such as neurohormonal blockers or adjustment of chemotherapy.2,3
The Multicenter Automatic Defibrillator Implantation Trial II (MADIT-II) was a randomized study comparing defibrillators to usual care of patients with systolic heart failure and a LVEF ≤30%. This trial used ECHO, SPECT, or left ventriculogram. 16 However, the relative frequency of use, for the different modalities used to measure LVEF, was not reported. In those patients with a LVEF between 25% and 50%, a potential difference of 10% in reported LVEF may lead to different clinical choices, such as devices, inclusion, or exclusion to the MADIT-II trial.
It is not clear whether ECHO or SPECT is the most accurate test technique to measure LVEF when comparing CMR as the gold standard. The correlation coefficient between ECHO and SPECT in clinical literature varies between 0.69 and 0.81 for patients with all LVEFs (Table 3).
Published Studies Comparing LVEF by ECHO and SPECT.
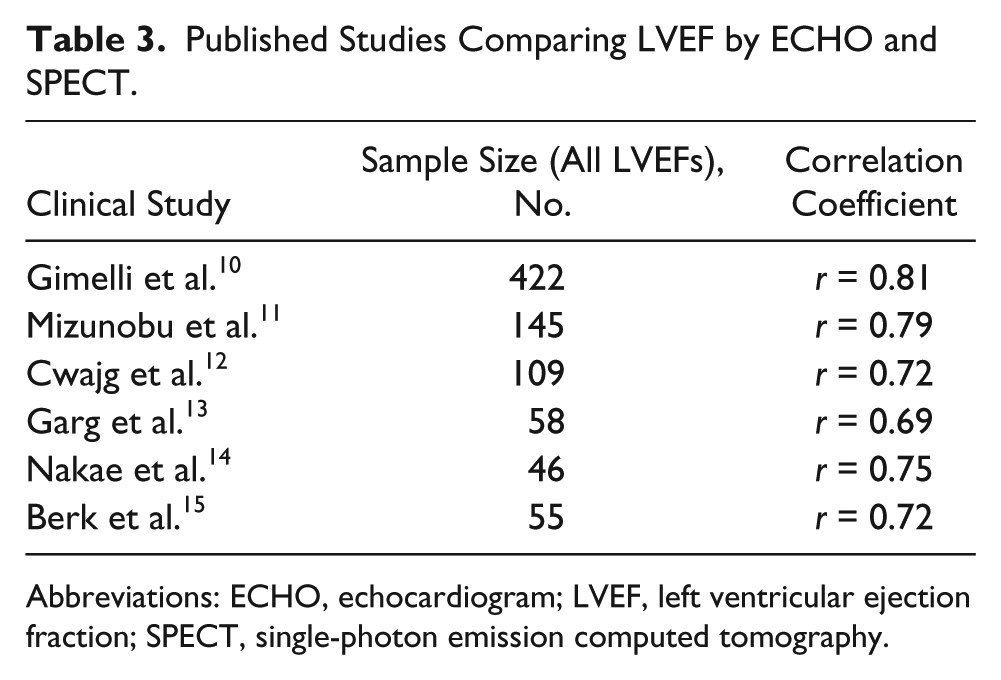
Abbreviations: ECHO, echocardiogram; LVEF, left ventricular ejection fraction; SPECT, single-photon emission computed tomography.
These studies involve all patients, including those with very high and very low LVEFs, where a difference of 10% would be clinically unlikely to affect treatment decisions.
There is, however, a relative paucity of information concerning the correlation of LVEFs by ECHO and SPECT in the intermediate range of 25% to 50%. The present study gives insight into the correlation between LVEF by ECHO and SPECT on subjects as a whole, as well as in a subset with patients having LVEF from 25% to 50%. Thus, knowledge of the results of correlation for LVEF from 25% to 50% is necessary for most providers evaluating HF patients for device implantation and/or medical therapy.
Multiple trials have compared ECHO and SPECT to each other (Table 3)10–15 and, at the same time, ECHO with CMR5,17 and SPECT with CMR.5,18 In three studies, patients underwent all imaging techniques, including SPECT, ECHO without contrast, and CMR. These studies demonstrated similar scattergrams for a small number of patients having LVEF between 25% and 50%, similar to the present study.19–21
This study as expected demonstrated a statistically significant correlation between LVEF by the two techniques; however, the correlation coefficient of 0.43 to 0.76 indicates that the clinical significance of this correlation is minimal. This fact has been recognized for decades. 22
For example, in this study, of the 99 patients with an LVEF between 25% and 50%, 36 had an LVEF of ≤35% by one of the two techniques. Furthermore, of that subset of patients, nine (25%) had an LVEF of ≥45% by the other assessment. Thus, in subgroups such as these, the clinical choice of medication or devices may not be appropriate without further evaluation.
These patients could potentially be denied an ICD if the LVEF by either technique has been used. This study informs the practitioner of the possible discrepancies between LVEF measured by ECHO and SPECT, especially when the discrepancy of LVEF by the two techniques may be as much as 10%.10–15
Rijnierse et al. 23 reported that 29 of 149 (19%) patients had an LVEF by CMR of <35% but an LVEF by ECHO of >35%, and thus these 29 patients would not have been eligible for ICD therapy by ECHO criteria. However, appropriate device therapy discharges occurred at a rate of 2.1% per year in this group who would not have received an ICD had only the ECHO criteria been used.
Options When LVEF Results Are Discrepant
Guidelines recommend ECHO as the preferred method to measure LVEF, 1 but physicians should be aware of the potential need for other imaging studies on patients when LVEF varies by 10% or more by two techniques. These options include performing a repeat ECHO with imaging contrast since multiple studies have demonstrated using imaging contrast markedly enhances the correlation of LVEF with CMR. 9 A recent study stresses the benefit for management of patients with reduced ejection fraction using CMR contrast-enhanced ECHO. 24 Other options include (1) review of ECHO studies with colleagues since the estimated LVEF is still unfortunately somewhat subjective, as evident from the intra/interobserver variability noted in our study and other studies4,5; (2) contrast biplane left ventriculogram; (3) noncontrast 3D ECHO if equipment and expertise are available and give a better correlation with CMR than contrast 2D ECHO 2 ; (4) use of cardiovascular computed tomography (CCT), which is reported to be increasing and has an excellent correlation to CMR 4 ; or (5) CMR, which is generally considered the gold standard.5,6 Thus, it is vital to enlist the most experienced readers of the various noninvasive modalities to help determine the LVEF when discrepant results occur.
Strengths
The main strength of this study is the evaluation of a predefined subgroup of patients with an LVEF between 25% and 50% by either technique who are in a range that a 10% difference may influence and alter clinical decisions. The LVEF determined by ECHO and SPECT was performed in a real-world clinical setting in a large referral tertiary center by cardiologists meeting the ASE standards.
In this study, both the compared tests (ECHO and SPECT) were done within a period of 72 hours. This decreases the variables that may have an influence on LVEF such as preload and afterload. Most studies in the literature had a period of greater than three days between the two tests. Only the studies by Cwajg et al. 11 and Mizunobu et al. 12 reported comparisons performed within three days (Table 3).
Weaknesses
This study was not designed to establish the accuracy of LVEF measured by ECHO or SPECT. The 2D ECHO was not performed with contrast, which has been shown to significantly improve LVEF when compared to CMR. 9 There was no comparison of LVEF by ECHO or SPECT with CMR.
Although all studies were read by a cardiologist meeting current ASE guidelines, it was very difficult to assess the number of cardiologists who were ECHO board certified due to the nature of this study. The LVEF determined by ECHO is subjective and based on the overall impression of the LVEF by the reader who may combine the quantitative LVEF by Simpson’s rule and the visual impression. We feel our teaching community reflects “real-world” practice and hence is generalizable to current practices in most US hospitals. It could be assumed that visual impressions of LVEF are the choice for most interpreters but cannot be confirmed for all settings.
Conclusions
Critical decisions are made for HF patients based on LVEF. Most studies for a selection of patients for ICD are based on LVEF determined by various techniques, especially ECHO and SPECT. We report a clinically significant discrepancy by the two techniques when LVEF is between 25% and 50%. Thus, the physician needs to be aware that LVEF determined by ECHO and SPECT may be discordant, and considerations should be given to additional imaging techniques, such as contrast ECHO, when there is a clinical need for a very accurate LVEF to help make decisions for medical and device therapy.
Footnotes
Acknowledgements
The authors would like to acknowledge Rob Cagna, MA, MSLS, JD, AHIP, for his extensive help with literature review and Kevin Driver, MD, for consultation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.