
Abstract
Aneurysms and pseudoaneurysms, of the anterior tibial artery, are very rare. Pseudoaneurysms of the anterior tibial artery are commonly due to iatrogenic injury, blunt trauma, fracture, or sharp penetrating injury. A young man presented to a pediatric emergency department with a pseudoaneurysm of the left anterior tibial artery due to an ankle sprain injury. Radiography, magnetic resonance imaging, and duplex sonographic imaging were completed to rule out all previously suspected diagnoses, and ultimately duplex sonography diagnosed and characterized the pseudoaneurysm. The utilization of duplex sonography in the investigation and diagnosis of injuries, particularly with extensive soft tissue swelling, provided quick diagnostic information and an expedited treatment plan. Conservative observation was initially attempted, followed by sonographic compression, sonography-guided thrombin injection, vessel ligation, and coil embolization. After initial treatment attempts failed, the patient was transferred to an adult hospital, with a specialized vascular surgery team, for vessel ligation and ultimate successful treatment with coil embolization.
Keywords
Ankle pain and swelling are common patient symptoms that present to emergency departments, following injuries designated as “ankle sprains.” 1 Pseudoaneurysms are uncommon results of such injuries but should be considered with the presentation of soft tissue swelling without musculoskeletal defects. Pseudoaneurysm of the anterior tibial artery are rare, especially when initiated by trauma versus iatrogenic causes. 2 Diagnosis and characterization of such a vascular defect is commonly made with duplex sonography due to its quick and dynamic capabilities.1,3 In this case, the pseudoaneurysm was the result of an ankle sprain injury during a basketball game.
Case Report
A 17-year-old male presented to the emergency department, of a pediatric hospital, with severe ankle pain and swelling following an eversion injury of his left ankle during a basketball game. The lateral left ankle was evaluated and significant tenderness with normal sensation and movement of the foot and toes was noted. There was no rash, laceration, or abrasion. The initial concern for the injury was a possible fracture or sprain of the left ankle. Radiography was completed of the tibia, fibula, ankle, and foot. No fracture was identified, but significant swelling of the tissue was noted (Figure 1). The new concern was for possible calcaneal tendon tear. A Thompson test was completed with a negative result for a calcaneal tendon tear. The patient was admitted for pain control and discharged the following day with pain medication, instructions to ice, and elevate his foot.

Anteroposterior radiograph of the left ankle taken on the initial date of injury demonstrating notable tissue swelling (arrow) over the lateral malleolus.
The patient returned to the emergency department two days after the initial injury occurred, with worsening pain, swelling of the ankle and foot, decreasing sensation of his foot to light touch, and the formation of ecchymosis and blisters with intact skin along the lateral left ankle. He was readmitted to the hospital for further pain control and observation. Clinicians considered possible differential diagnoses such as compartment syndrome or necrotizing fasciitis. Additional radiographic images were obtained reconfirming the absence of fracture and increasing soft tissue swelling of the dorsal and lateral aspects of the left foot and ankle (Figure 2). The patient was assessed for compartment syndrome, but all compartments of the ankle and foot were soft and compressible upon examination. Further investigation of the soft tissue ruled out necrotizing fasciitis as well.

Anteroposterior radiograph of the left ankle taken two days after the initial injury demonstrating increased tissue swelling of the left foot and ankle.
A magnetic resonance imaging (MRI) examination was completed three days after the initial injury to better characterize the soft tissue damage. The MRI demonstrated a lobulated, prominent, nonenhancing fluid collection within the soft tissue overlying the lateral malleolus and anterior ankle. The fluid collection measured 5.8 × 4.3 × 5.3 cm (craniocaudal x transverse x anteroposterior) and was determined to be a hematoma (Figure 3). Within the hematoma, an atypical focus was identified with a rim of enhancement and pulsation artifact (Figure 4). This structure was suspicious for a possible arterial injury with formation of a pseudoaneurysm. The MRI also demonstrated continued subcutaneous edema and a partial tear of the anterior talofibular ligament and deep deltoid ligament. These findings warranted a duplex sonographic examination of the left ankle, which was completed later that same afternoon.
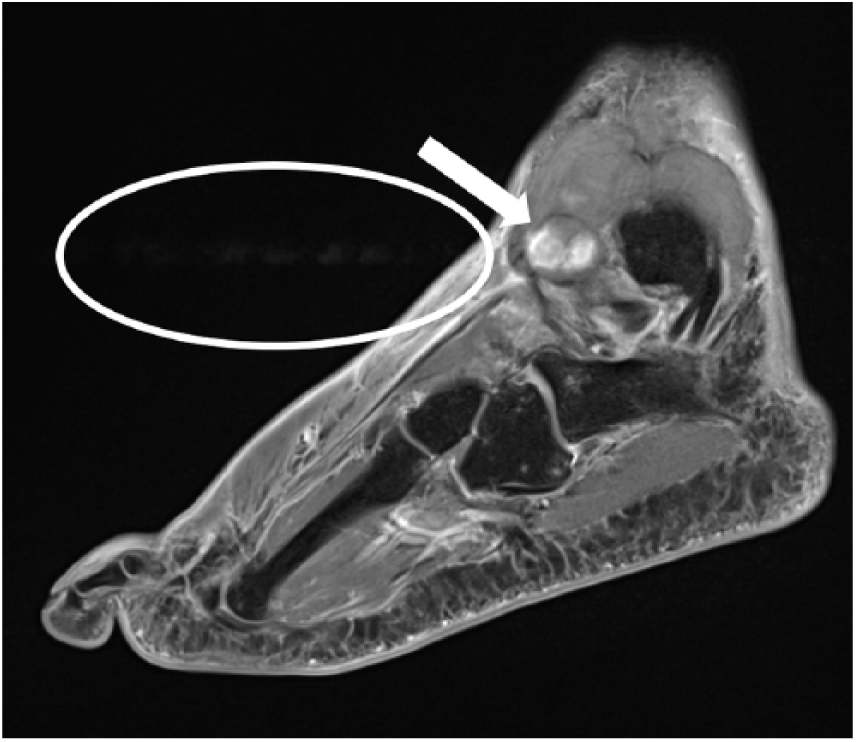
Sagittal magnetic resonance imaging view of the left ankle and foot demonstrating the hematoma (arrow) and pulsation artifact (circle).
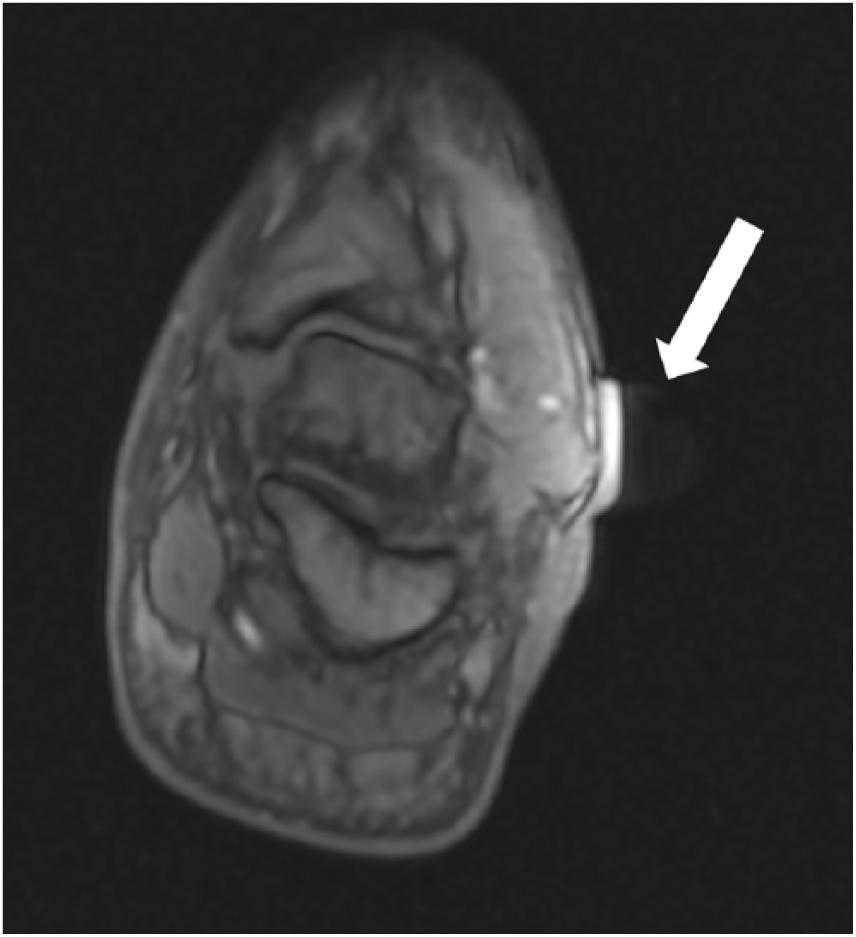
Axial magnetic resonance imaging view of the left ankle demonstrating the rim enhancement and pulsation artifact (arrow).
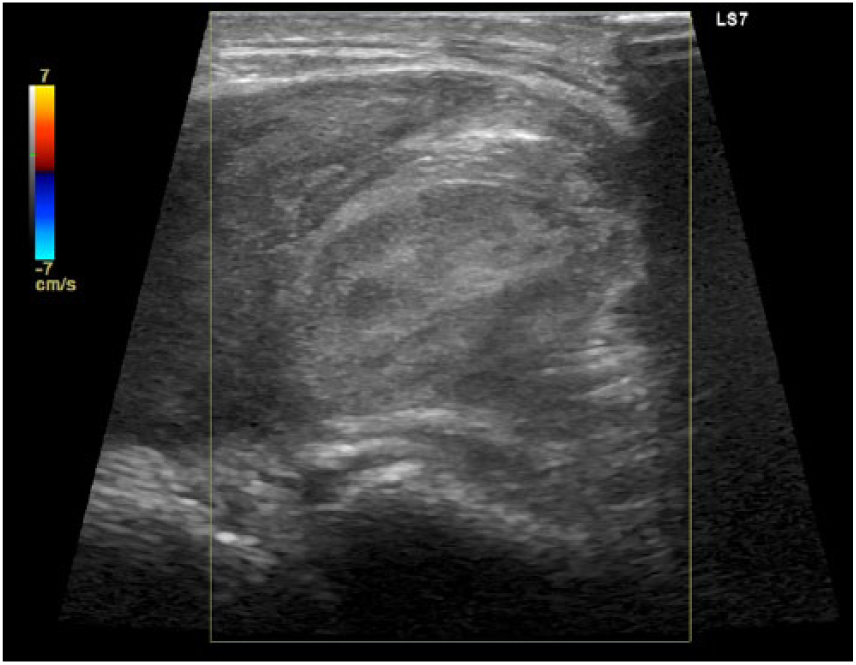
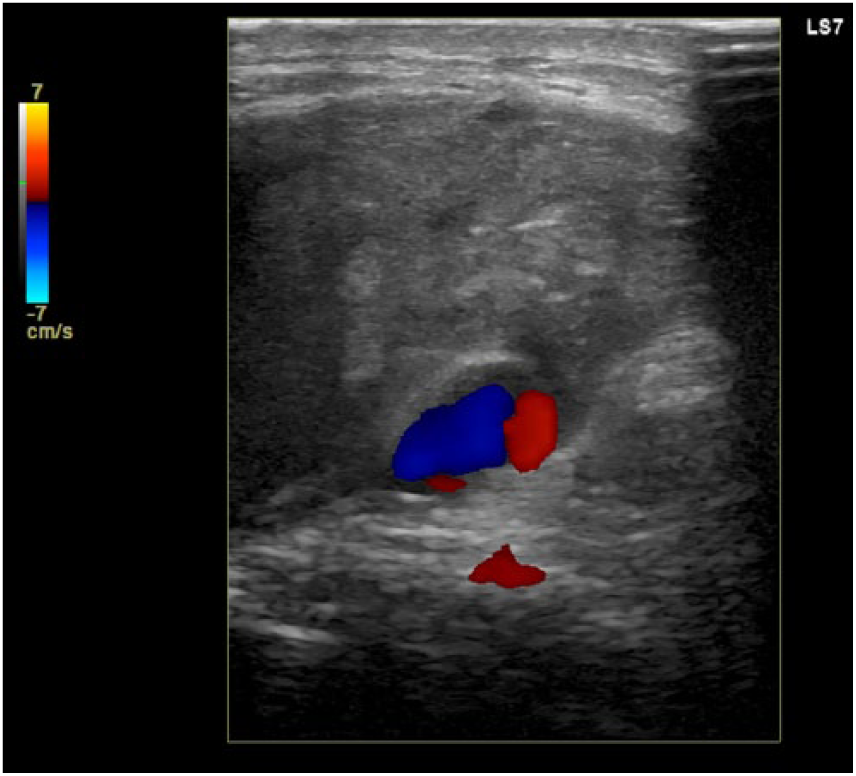
A high-frequency linear probe was used to evaluate the lateral left ankle in multiple planes in B-mode with and without color Doppler. The duplex sonographic examination confirmed a large, complex hematoma on the anterolateral left ankle with a partially thrombosed, pulsating pseudoaneurysm. A feeder vessel was identified pumping arterial blood into the pseudoaneurysm sac, a patent portion of the pseudoaneurysm, measuring 1.1 × 0.9 × 0.6 cm. The entire area, hematoma and patency combined, measured 1.8 × 1.6 × 1.9 cm (Figure 5). Doppler sonographic interrogation visualized a swirling flow pattern within the patent portion of the pseudoaneurysm demonstrating a “yin-yang sign” (Figure 6). The feeder vessel had a high-resistance waveform, and aliasing was seen at the neck of the pseudoaneurysm (Figure 7). Pulsed-wave Doppler tracings taken from the center of the patent portion demonstrated bidirectional flow during swirling pulsation and silence of flow during the diastolic period (Figure 8). The initial reading of the sonographic images concluded that the feeder vessel was likely a branch of the peroneal artery; later imaging confirmed that the injury was actually to a branch of the anterior tibial artery. Treating physicians determined that immediate intervention was not recommended due to the tendency of pseudoaneurysms to resolve on their own. It was decided to follow the injury with serial sonographic examinations to track the healing process.
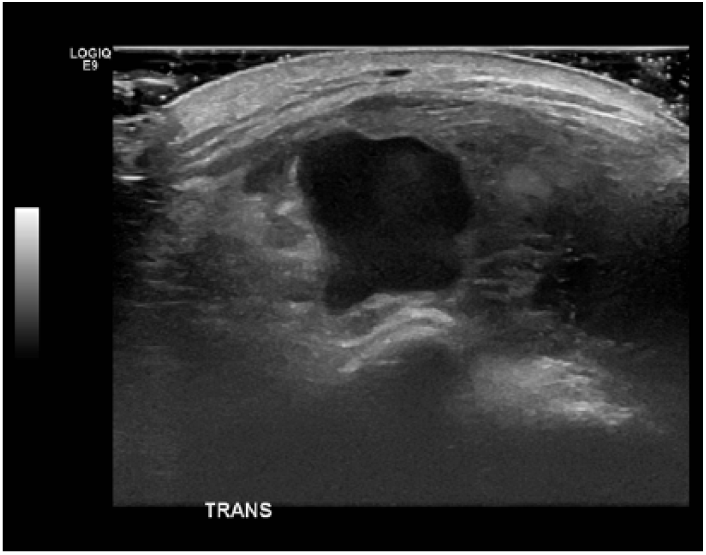
Transverse gray-scale sonogram of the anterolateral left ankle demonstrating the large patent portion of the pseudoaneurysm.
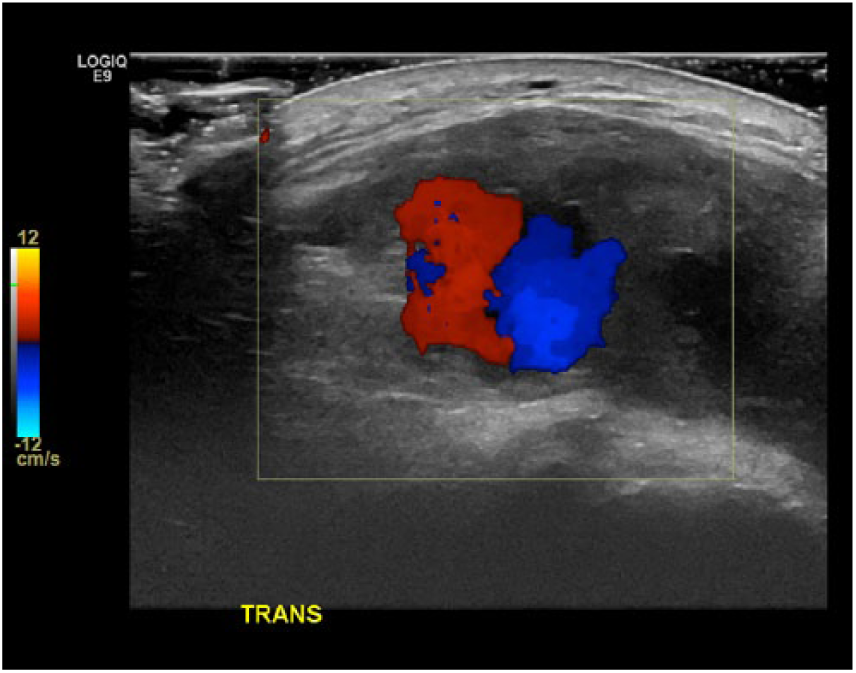
Transverse color Doppler sonogram of the anterolateral left ankle demonstrating the “yin-yang sign” within the patent portion of the pseudoaneurysm.
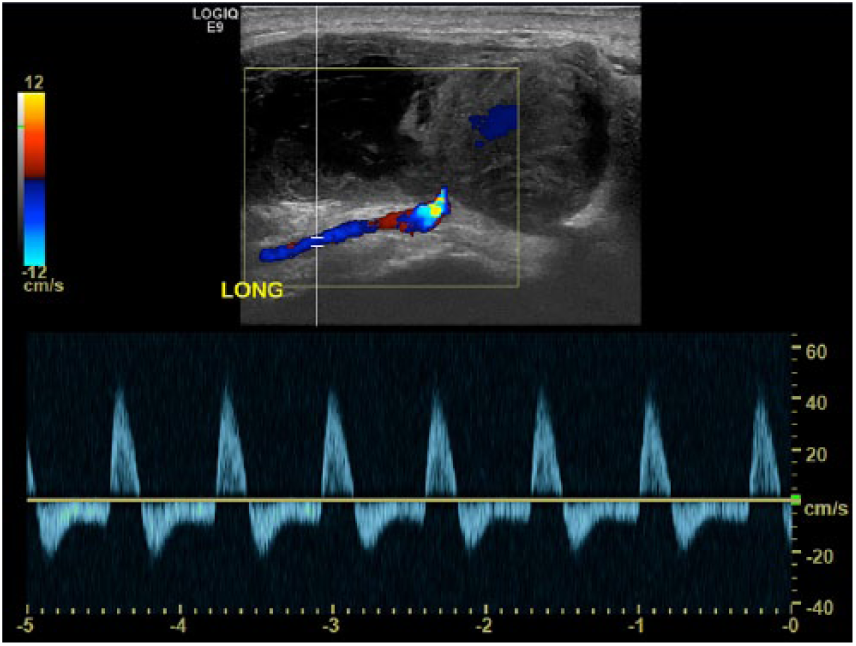
Longitudinal pulsed-wave Doppler sonogram of the anterolateral left ankle demonstrating the high-resistance wave form in the feeder vessel and color Doppler aliasing at the neck of the pseudoaneurysm.
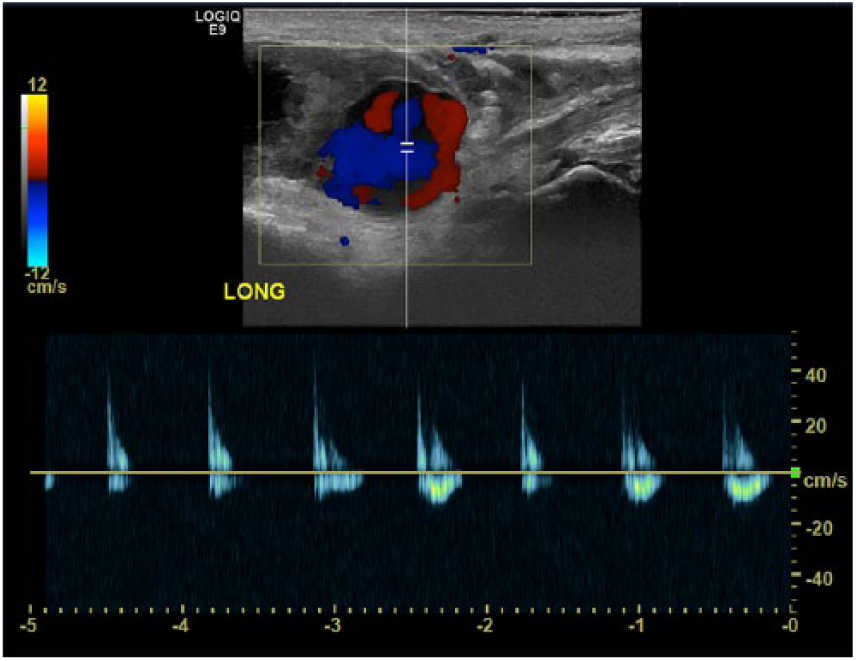
Longitudinal pulsed-wave Doppler sonogram of the anterolateral left ankle demonstrating bidirectional flow in systole and silence of flow in diastole within the patent portion of the pseudoaneurysm.
The patient remained in the hospital for pain control and monitoring and was reevaluated with sonography seven days after the initial injury occurred. The follow-up duplex sonogram found a persistent patent arterial pseudoaneurysm with surrounding hematoma measuring larger than the original scan: 2.1 × 1.8 × 2.2 cm. Alternative treatment options were discussed with orthopedic surgery, interventional radiology, and cardiovascular surgery. A final decision was made to discharge the patient with more pain medication, a boot, and a watch-and-wait strategy.
The patient returned to the hospital 18 days following the initial injury for a follow-up duplex sonographic examination. The patient was still immobilizing the left foot and ankle with utilization of a boot and crutches. He noted that his pain had improved, the blisters on his ankle had drained and were healing, but that the swelling persisted. Duplex sonography imaging identified that the hematoma was slightly larger, measuring 2.1 × 1.9 × 2.6 cm. There was also an increase in size of the nonthrombosed pseudoaneurysm patency measuring 1.9 × 1.4 × 1.4 cm (initially 1.1 × 0.9 × 0.6 cm). Treating physicians discussed the potential need for vascular surgery, but no specialized team for such procedures was present at the pediatric hospital.
Twenty-one days following the initial injury, an interventional radiology procedure for pseudoaneurysm compression and thrombin injection was completed at the neck of the pseudoaneurysm. Sonography-guided compression was employed for 30 minutes at the neck of the pseudoaneurysm. Following compression, increased echogenicity was seen throughout the pseudoaneurysm compared to precompression, but persistent flow was detected. Five hundred units (0.5 mL) of thrombin were then injected into the patent portion of the pseudoaneurysm. After the injection, no residual flow was detected with Doppler sonography.
The patient arrived for a follow-up sonographic examination the next day. Recurrence of the patent pseudoaneurysm was identified with similar measurements as the previous duplex sonograms. Turbulent flow within the patent portion and a to-and-fro pattern in the neck were again documented.
Twenty-two days following the initial injury, a repeat interventional radiology procedure for pseudoaneurysm thrombin injection was completed. The pseudoaneurysm was patent before the thrombin injection (Figure 9). One hundred units (0.1 mL) of thrombin was injected into the pseudoaneurysm (Figure 10), which then appeared completely thrombosed (Figure 11). Sonographic imaging was completed 30 minutes after injection, which identified a small recanalized sac (Figure 12). An additional 100 units (0.1 mL) of thrombin was injected. Sonographic imaging 20 minutes later showed no recanalization. The procedure was determined to be technically successful, and a follow-up duplex sonographic examination was scheduled for the following day.
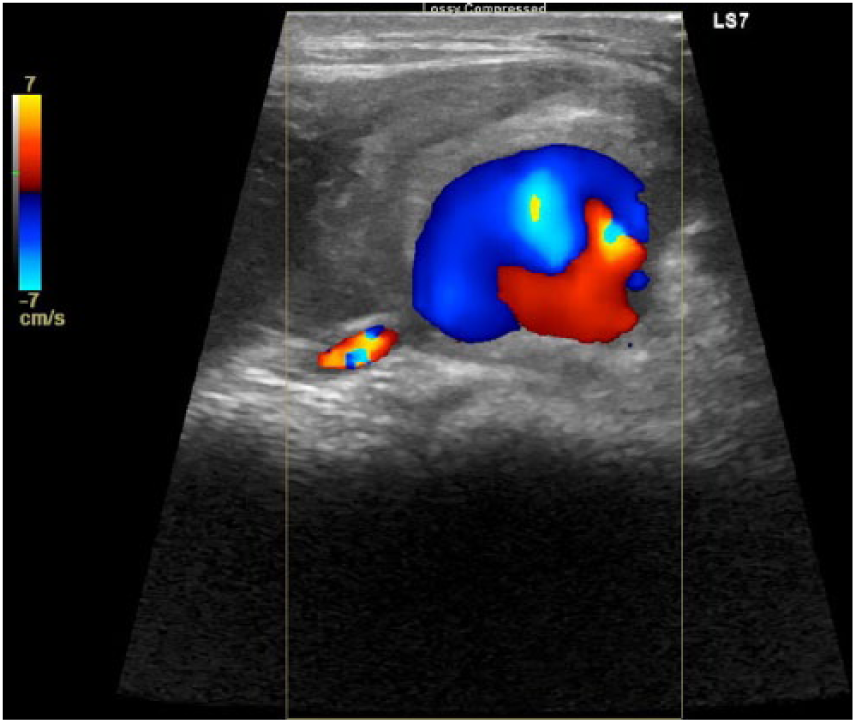
Longitudinal color Doppler sonogram of the patent pseudoaneurysm before thrombin injection.
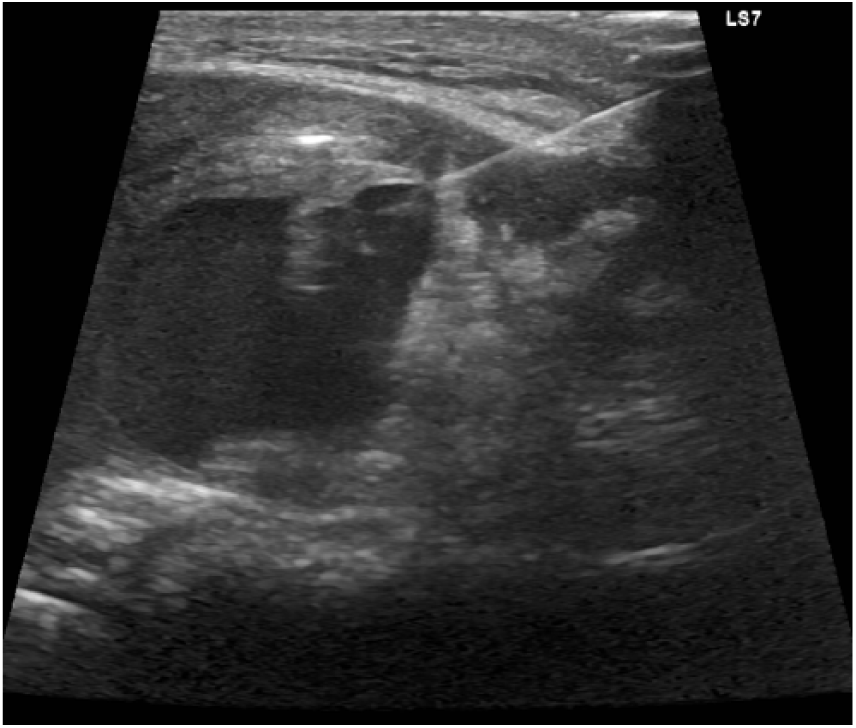
Longitudinal gray-scale sonogram of the needle injecting thrombin into the patent pseudoaneurysm.
Longitudinal color Doppler sonogram of completely thrombosed pseudoaneurysm after thrombin injection.
Longitudinal color Doppler sonogram demonstrating recanalized pseudoaneurysm sac 30 minutes after thrombin injection.
When the patient presented for the follow-up sonogram, a persistent turbulent pseudoaneurysm sac was identified, partially thrombosed, but still patent. The blood flow patterns continued to demonstrate to-and-fro flow in the neck. Twenty-three days following the initial injury, the patient had a computed tomography angiography (CTA) scan completed to make plans for continued treatment. The results of the scan reconfirmed an injury to the anterior tibial artery at the level of the lateral malleolus, redemonstrating a pseudoaneurysm and large surrounding hematoma along the lateral aspect of the left ankle. The patient was then transferred to an adult hospital to receive further care from a specialized vascular surgery team.
Twenty-four days following the initial injury, the patient underwent a vascular surgery to ligate the proximal and distal anterior tibial artery. The vessel was still bleeding postsurgery, and another operation was scheduled for the following day. An angiogram was completed of the anterior tibial artery to confirm that the vessel was still patent before the second operation began. On the 25th day following the initial injury, the patient was ultimately treated with coil embolization of the anterior tibial artery. The posterior tibial artery pulse was palpable postsurgery, blood flow to the foot was maintained, and the pseudoaneurysm was successfully treated.
Discussion
A pseudoaneurysm, following injury or surgery of the foot and ankle, is very rare. 1 The most common causes of pseudoaneurysm in the foot and ankle are arterial catheterization and trauma. 2 A pseudoaneurysm develops when a defect in all three layers of the arterial wall fail to heal, resulting in blood flow outside of the artery and into surrounding soft tissue.1,3,4 The affected soft tissue then forms a fibrous capsule around the defect, which contains blood flowing outside the damaged vessel. 4 A pseudoaneurysm is structurally different from a true aneurysm, which is characterized by dilatation of a vessel wall with all three layers of the vessel intact. 4 Pseudoaneurysm of the anterior tibial artery due to blunt trauma injury of the ankle is uncommon, but other cases may be found in the literature.1,2,4 The mechanism of injury is assumed to be compression of the vessel against bony structures in the ankle during impact as well as stretching of the vessel during inversion or eversion.1,5 Most injuries to the anterior tibial artery are described after interventional procedures such as ankle arthroscopy. 1 Other recorded causes of pseudoaneurysm include penetrating trauma, fracture, or iatrogenic injury during other procedures. 6 Clinical diagnosis of vessel damage is often made relatively long after the initial injury because suspicion is low due to the rarity of pseudoaneurysm formation in these cases. 6 Because of a typical delay in diagnosis, treatment is also delayed, making potential complications more dangerous. 6
The symptoms and clinical presentation that are usually reported with pseudoaneurysms include a distinct palpable mass with or without pulsatility or bruits, soft tissue swelling, mass effect, neurologic deficits, pain and tenderness, local ischemia of the distal foot, and compartment syndrome.1,3,6,7 The delay in diagnosis is particularly risky due to the ability of untreated pseudoaneurysms to expand. 2 Untreated pseudoaneurysms are at risk for hemorrhage, arterial thrombosis, and distal embolism, as well as neurologic damage and ischemia to nonperfused tissues.2,6
Multiple imaging modalities can be used to identify and diagnose pseudoaneurysms. CTA is the imaging gold standard, due to its ability to provide global anatomical information for treatment, but duplex sonography permits the most rapid, dynamic, and exact diagnosis.1,3,6,7 Duplex sonography allows for identification of thrombus echogenicity, bleeding fluctuations, and the classic pseudoaneurysm signs of pulsatile and turbulent flow. 3 CTA and duplex sonographic imaging are the most commonly used modalities; MRI, magnetic resonance angiography, and angiography are also typical imaging tests ordered when a pseudoaneurysm is suspected.1,2,3,6,8 Duplex sonographic interrogation of a pseudoaneurysm will detect a defect in the arterial wall, a neck from the artery feeding a cystic outpouching (pseudoaneurysm sac) into the surrounding soft tissue, and both inflow and outflow of the pseudoaneurysm sac with the classic “yin-yang sign.” 8
Many differential diagnoses may be considered with trauma injuries to the ankle before and after imaging. Before imaging, ankle sprain, fracture, compartment syndrome, and necrotizing fasciitis may be considered, as seen in this case. 3 Hematoma, abscess, arteriovenous fistula, soft tissue tumor, and a cyst are included in potential diagnoses when interrogated with sonography.3,6,7
Once a pseudoaneurysm is confirmed, it is necessary to promptly select treatment due to the instable nature of a pseudoaneurysm; the fibrotic capsule of a pseudoaneurysm is weaker than a vascular wall and is at a greater risk for rupture. 3 Treatment depends on the location and extent of vascular damage, but many of the same options are routinely considered. More conservative treatment options for pseudoaneurysm repair tend to be the first options taken, followed by more invasive techniques when initial attempts fail. Conservative treatment options include monitoring for self-resolution, sonography-guided compression, and sonography-guided thrombin injection.1,2,4,6–8 Sonography-guided compression is completed at the neck of the pseudoaneurysm and typically consists of 10-minute intervals for 20 to 30 minutes or until occlusion is achieved. 3 Sonography-guided thrombin injection is a common first option as well and many times is combined with sonographic compression, as seen in this case. 3 Resection of the pseudoaneurysm with vein grafting or endovascular stenting, ligation, and percutaneous endovascular coil embolization are more serious surgical treatments selected cautiously due to the bleeding risk of a pseudoaneurysm.1,2,4,6–8 Follow-up appointments and imaging are scheduled to ensure treatment options continue to be successful and appropriate healing processes take place.
Conclusion
Pseudoaneurysms of the foot and ankle are uncommon consequences of injury but have been reported in the literature. Diagnoses of pseudoaneurysms of the ankle are often delayed due to differential diagnoses, including ankle sprain, compartment syndrome, and other masses. Early diagnosis is essential for the avoidance of complications associated with pseudoaneurysms. Duplex sonography allows for targeted examinations to be completed quickly and provides excellent diagnostic information with lower costs and no ionizing energy. Injuries, such as the one described in this case, are often initially interrogated with radiographic images or MRI. A sonographic imaging approach may save time, continued pain, and damage for many patients whose treatment plans could benefit from the use of duplex sonography early in their care. Although conservative treatment methods are often selected first, surgical treatment should not be rejected; as demonstrated in this case, it may be required for repair of the injury. This case highlights the importance of early diagnosis with duplex sonography and treatment for an unusual complication of a common ankle sprain.
Footnotes
Acknowledgements
The authors thank Jonathan D. Samet, MD, Merima Karastanovic, MS, RT (R) (MR), and Thea Thommen, RDMS, RVT, for their time, assistance, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.