
Abstract
Oncocytic neoplasms of the head and neck arise from a dysfunction of the mitochondria. These cells are often called Hürthle cells and recognized as one of the rarest forms of thyroid cancer. Diagnostic imaging is usually performed by sonography with a fine-needle aspiration following the sonogram. A case is presented of an oncocytic neoplasm that was initially identified sonographically. The mass was then characterized using the thyroid imaging reporting and data system, followed by a fine-needle aspiration and gene expression classifier to obtain additional information about the diagnosis. The use of sonography followed by biopsy helped to determine the proper treatment of the neoplasm in the thyroid gland.
Keywords
An oncocytic neoplasm of the thyroid, also known as Hürthle cell neoplasm, is a rare type that only accounts for 3% to 5% of thyroid cancers. 1 This unusual finding is considered a variant of follicular carcinoma according to the World Health Organization (WHO). 1 The presence of oncocytic neoplasms is identified by their distinct characteristic of mitochondrial hyperplasia due to mitochondrial dysfunction. 2 These Hürthle cells can appear in many places around the head and neck, including the thyroid, lymph nodes, and salivary glands. This case presents a large oncocytic neoplasm in the right lobe of the thyroid gland. Sonography provided visualization and the ability to classify its suspicion, and a fine-needle aspiration (FNA) was used to confirm diagnosis.
Case Report
A 71-year-old Caucasian man presented to the sonography department after a physician noted a palpable, supple right-sided neck mass. The patient denied any symptoms. The mass was not identified in a physical performed by a different physician seven months prior. Thyroid function laboratory tests were performed and were within normal limits. A sonogram was then performed using a GE LOGIQ E9 ultrasound equipment (General Healthcare, Chicago, IL) and a linear 15-MHz transducer.
The thyroid sonogram revealed a complex lobulated nodule within the right lobe under the palpable lump. The right thyroid gland measured 6.07 × 3.46 cm in the longitudinal plane (Figure 1). The nodule measured 4.84 × 4.15 × 3.54 cm (Figure 2). The superior and inferior portions of the right lobe demonstrated echogenic calcified areas with posterior shadowing (Figures 3 and 4). Color Doppler was used on both the right and left sides of the thyroid to compare the vascularity, demonstrating hypervascularity of the right side (Figures 5 and 6). Color Doppler of the right lobe nodule showed anechoic areas with no flow and posterior enhancement, providing evidence of cystic areas inside the solid nodule (Figure 6).
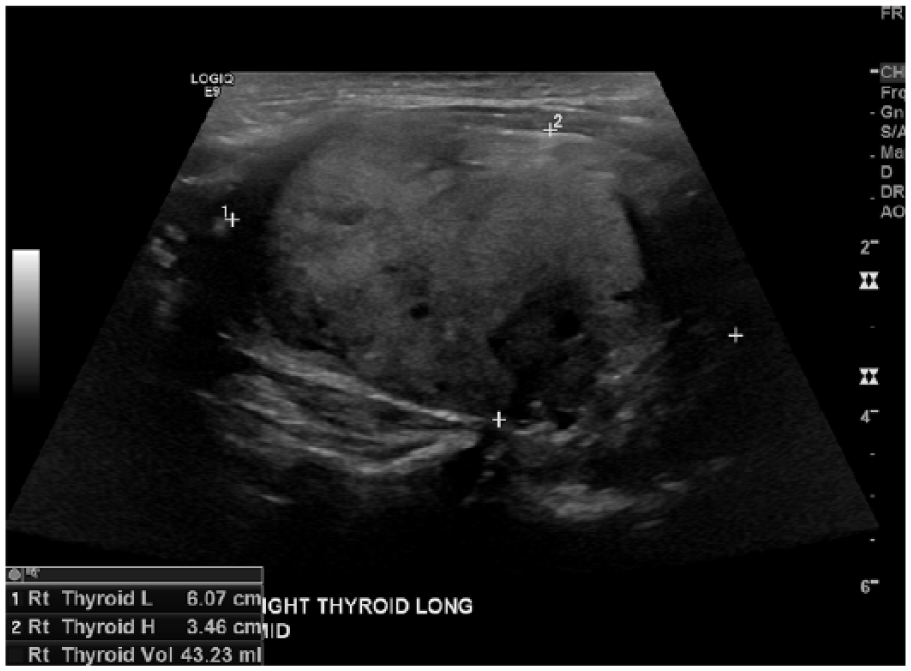
Longitudinal gray-scale sonogram of the right lobe of the thyroid gland in the midportion measuring 6.07 × 3.46 cm and containing the suspicious nodule.
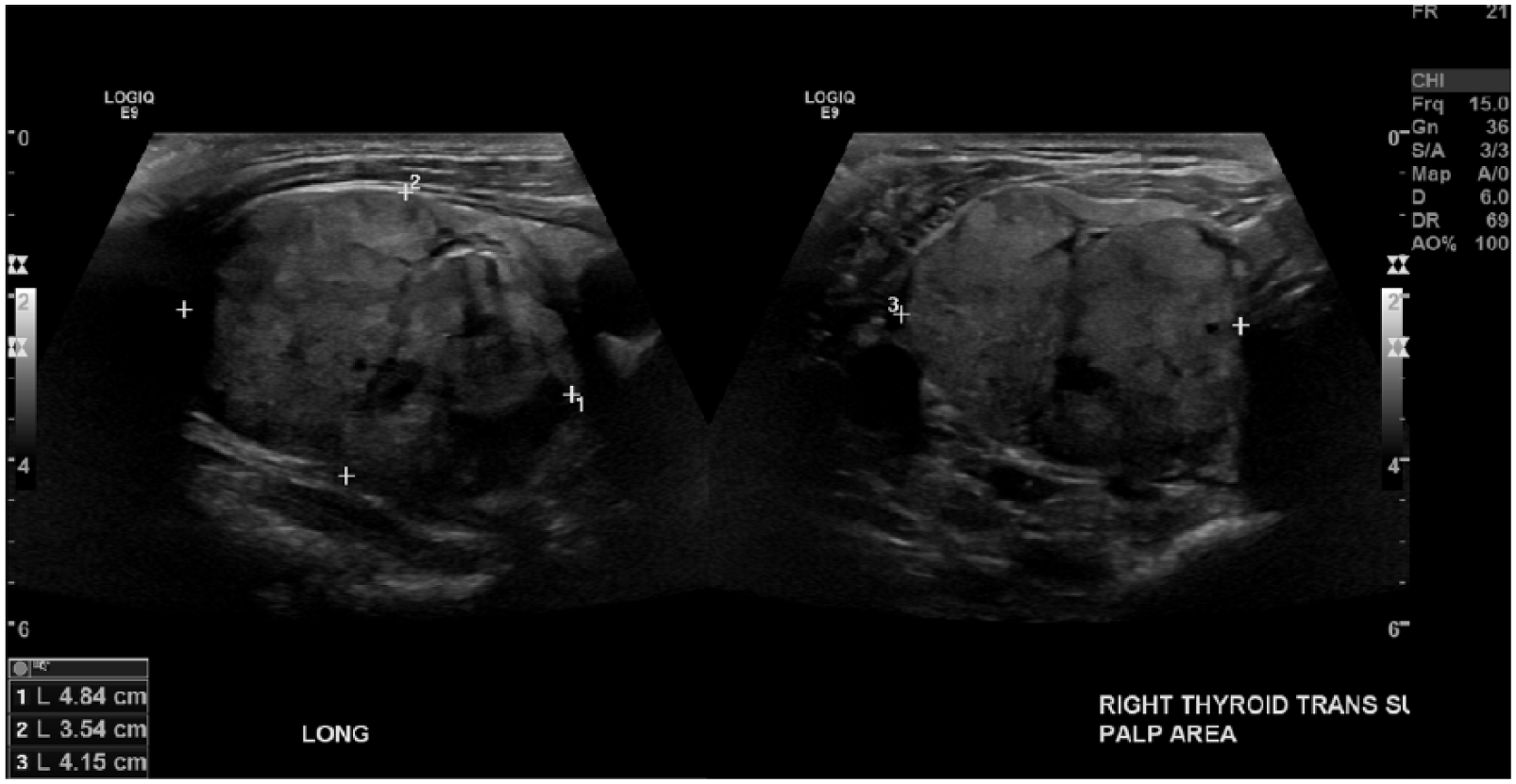
Longitudinal and transverse gray-scale sonograms of the right lobe of the thyroid gland in the midportion showing a suspicious complex nodule measuring 4.84 × 4.15 × 3.54 cm.
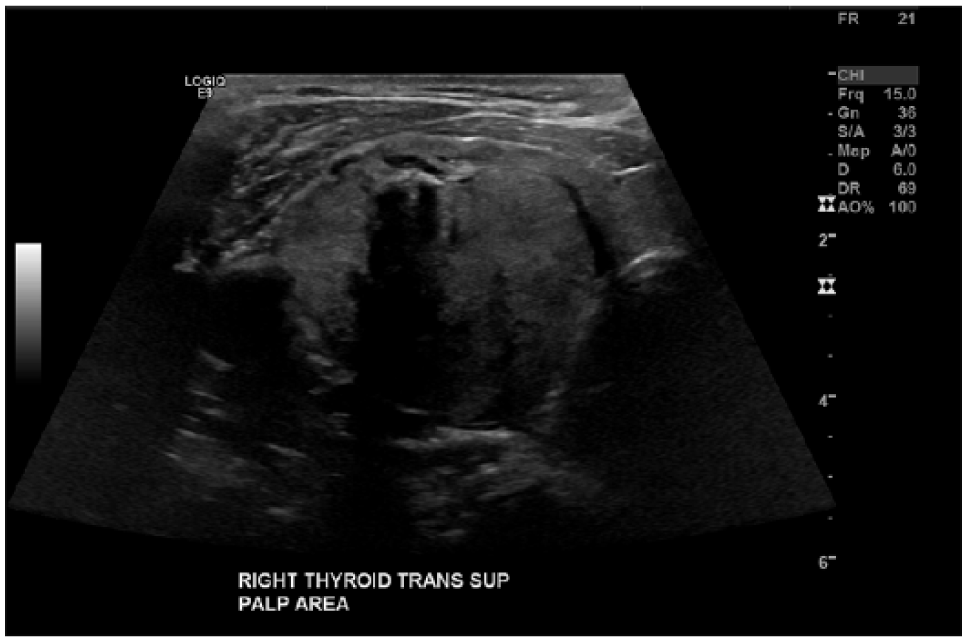
Transverse gray-scale sonogram of the superior portion of the right lobe of the thyroid gland displaying a complex nodule with posterior shadowing behind a calcified area within the nodule.
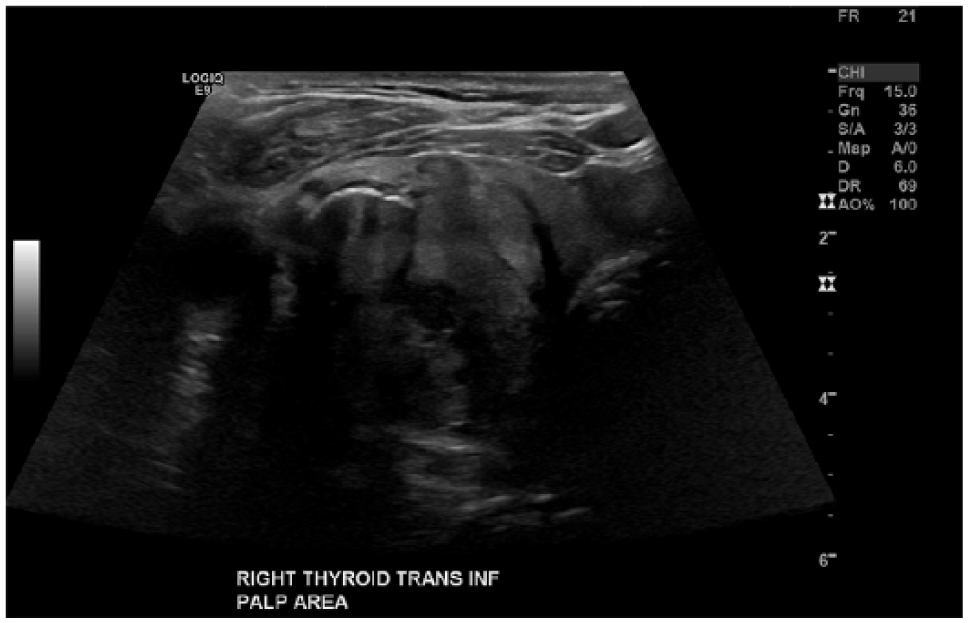
Transverse gray-scale sonogram of the inferior portion of the right lobe of the thyroid gland showing the nodule with another calcified area with posterior shadowing.
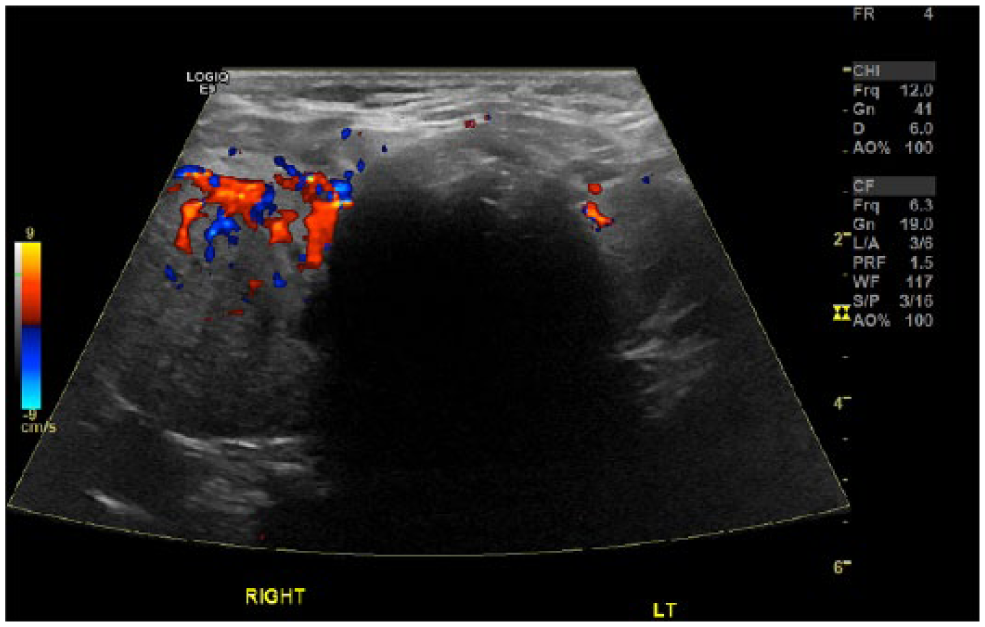
Transverse color Doppler image of the entire thyroid gland for comparison of the size and vascularity of the right lobe of the thyroid gland to the left lobe demonstrating hypervascularity of the right lobe.
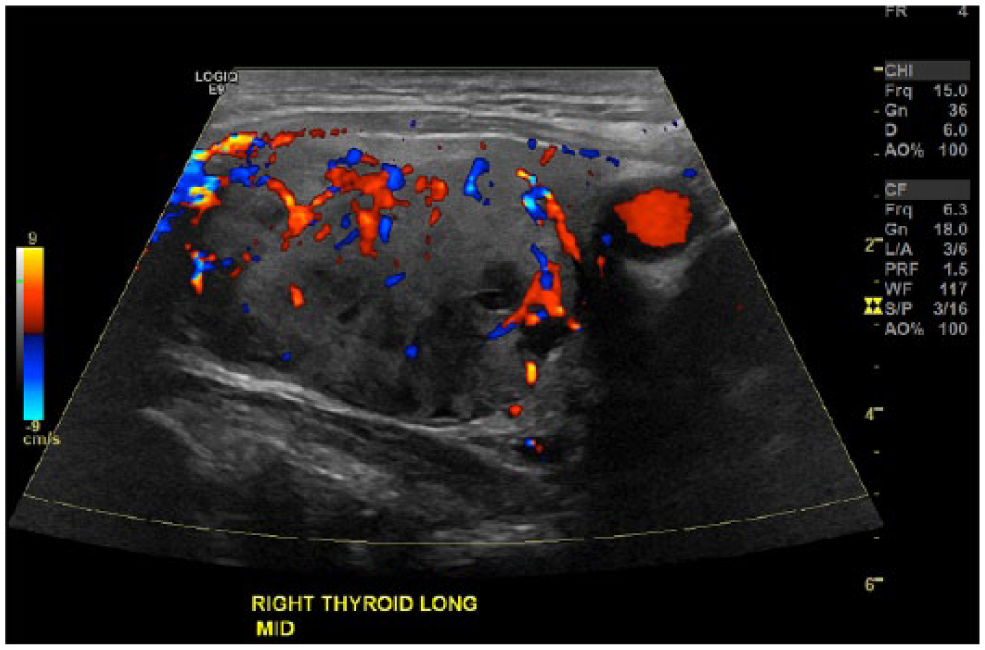
Longitudinal color Doppler image of the right lobe of the thyroid gland in the midportion showing hypervascularity and lack of flow in cystic areas with posterior enhancement in the complex nodule.
Using the images from the sonogram, the radiologist assigned this nodule as a category 4 using the thyroid imaging reporting and data system (TI-RADS). Because nodules assigned anything over a category 3 are automatically recommended for an FNA if the mass is greater than 2.5 cm, no other imaging modalities were used following the sonogram. An FNA was performed, finding cytology consistent with oncocytic neoplasm, or Hürthle cells. A gene expression classifier was also suggested, and an N-ras mutation conveyed a 50% chance of these cells being malignant.
Following these results, the patient was encouraged to undergo a right thyroid lobectomy as the next course of action. This operation occurred approximately one month after the initial sonogram was performed. After the surgery, the results of the pathology report confirmed the diagnosis of a 4.6-cm oncocytic neoplasm that was encapsulated and angioinvasive, as well as a 0.2-cm papillary carcinoma. Given the histological diagnosis and size of the cancer, it was recommended that the patient undergo a complete thyroidectomy, which was discussed during a follow-up appointment along with discussion of starting thyroid hormone replacement therapy.
Discussion
Arising from epithelial cells, Hürthle cell carcinoma is among the rarest forms of cancer in the thyroid gland and is considered a variant of follicular carcinoma. 1 The word oncocyte comes from the Greek word swell, which is the main characteristic of this cell due to the aberrant accumulation of mitochondria. Only if the nodule is found to comprise more than 50% oncocytic cells can it be called an oncocytic tumor, or Hürthle cell carcinoma. 3 While the direct etiology of this carcinoma is unknown, the findings are consistent with an alteration of the nuclear genetic material and mitochondrial DNA. 2 These cells are likely to metastasize to the lungs, bones, liver, and lymphatic system. 2 Hürthle cell is diagnosed as malignant with the identification of capsular and/or vascular invasion. 2
The mean age for oncocytic carcinomas is 54.3 years. 1 This carcinoma represents approximately 3% to 5% of all thyroid neoplasms, with an average tumor size of 41.8 mm. 1 The female to male ratio for this carcinoma is 3.6:1, respectively. 1 No symptoms are apparent for this carcinoma, which gives the cancer years to slowly grow before feeling or noticing abnormalities. 3 Symptoms that may develop later with this cancer are compression of adjacent structures in the neck causing neck pressure and dysphagia. 3
Upon noticing a palpable lump in the neck, a sonogram is usually the first imaging modality of choice. The sonographic appearance of an oncocytic neoplasm is a complex lobulated nodule with microcalcifications and hypervascularity replacing normal thyroid tissue. The sonographic characteristics and size of the nodule are then categorized using TI-RADS. 4 This classification system takes into account composition, echogenicity, shape, margins, and echogenic foci. 4 Points are assigned to the nodule in each of the five categories, with suspicious findings given additional points. 4 The American College of Radiology created this point system to accurately grade the nodule as benign, not suspicious, mildly suspicious, moderately suspicious, or highly suspicious for malignancy. 4 The higher the points assigned, the higher the suspicion for malignancy. If a nodule measures greater than 2.5 cm and assigned three points or more, it is considered mildly suspicious and an FNA is recommended. 4
An FNA biopsy is used as a safe way to gain information about the cytology or cell biology of abnormal tissue inside the body. This procedure is usually performed under sonographic guidance to ensure accurate placement of the biopsy needle. The cells are then examined by a cytopathologist to help make a more specific diagnosis. In cases that appear to be more suspicious for malignancy, a gene expression classifier (GEC) will be used with the cells obtained from the FNA. 5 The GEC is a preoperative test that assigns the cells a percentage of how likely they are to be benign or malignant based on the genes and appearence. 5 One thing that must be considered when dealing with nodules that are suspicious for Hürthle cell is that an FNA cannot definitively diagnose Hürthle or oncocytic cells. 5 This diagnosis is only a prediction based on its appearance and the results from the FNA and GEC. 5 Oncocytic cells are only conclusively diagnosed after evaluation of the nodule by a pathologist after a lobectomy or complete thyroidectomy.
Hürthle cell carcinoma is removed via surgery as its first course of action. 1 The extent of the nodule’s invasion into the thyroid tissue directly determines the prognosis of the oncocytic carcinoma following removal. 2 If the histological findings confirm cancer following a thyroid lobectomy, a complete thyroidectomy should be preformed. 3 Following the resection of the thyroid, patients are placed on thyroid hormone replacement therapy. 3 These medications replace the hormones lost from the resection that the body would have manufactured itself. Recurrence rates for Hürthle cell carcinoma are 14% to 44%. 3 Thyroid hormone replacement therapy is known to lower these recurrence rates by inhibiting tumor growth through negative feedback on the pituitary gland. 6
Conclusion
Oncocytic neoplasms, also called Hürthle cell neoplasms, are among the rarest types of cancers to invade the head and neck, including the thyroid, salivary glands, and lymph nodes. 3 Surgical resection of the cells remains the primary treatment option when malignancy is suspected. 1 This case demonstrates the important role sonography plays in properly classifying and diagnosing nodules in the thyroid for further consideration and guidance during an FNA. Detecting and diagnosing these cell types promptly are critical to the prognosis of the patient.
Footnotes
Acknowledgements
The authors thank Anne Trent, RDMS, RVT, and Mark Tinsley, RDMS, RVT, for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.