
Abstract
Objective:
Ultrasonography (US) and fine-needle aspiration biopsy (FNAB) play an important role in the diagnosis of thyroid nodules. The primary aim of this study was to evaluate the relationship between American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) and the Bethesda system, based on final cytopathology.
Materials and Methods:
The cases that underwent thyroidectomy, due to a nodule, between May 2019 and May 2021 were retrospectively imaged. Of those cases, 73 patients were included in the study. The obtained data included ACR TI-RADS and the Bethesda system scores for nodules.
Results:
According to Spearman correlation, a very strong positive relationship was found between the Bethesda scoring system and ACR TI-RADS scores (ρ = 0.832, P < .0001). A 94.4% sensitivity and 65.4% specificity were found in 16 patients with a Bethesda score of 3 and TR3 based on final pathology (P < .001). And a sensitivity of 77.3% and specificity of 51.5% were found in 17 patients, with a Bethesda score 4 and TR4 (P < .001). Finally, a sensitivity of 55.6% and specificity of 50.0% were found in 17 patients with a Bethesda score 6 and TR5 (P < .001).
Conclusion:
The routine use of the ACR TI-RADS classification in thyroid nodules could be useful in preventing unnecessary FNABs. It could be effective in minimizing complications secondary to FNAB and thyroidectomy and reducing costs.
Thyroid nodules are common in the general population and up to 95% of them are cytopathologically classified as benign. Because of the increase in access to diagnostic technologies, especially ultrasonography (US), it is a clinical problem with a prevalence of up to 70% in adults. 1 After the thyroid nodule is diagnosed, unnecessary and repetitive biopsies for benign nodules should be avoided and treatment should be planned for malignant nodules. The malignancy is seen in approximately 5% of thyroid nodules, and US-guided fine-needle aspiration biopsy (FNAB) is the test used to differentiate benign or malignant nodules. 2 Recently, there has been a steady increase in the incidence of thyroid cancer worldwide, the cause of which has not been fully determined. It is thought that this increase in thyroid cancer may be due to the improvement in diagnostic methods rather than a real increase. 3
When identifying malignant nodules with FNAB, it is necessary to reduce the number of biopsies performed for benign nodules. Although FNAB has a critical role in the detection of thyroid malignancy, it is a costly and minimally invasive procedure. 4 If the number of unnecessary biopsies can be reduced, it will reduce costs, patient anxiety, risks of bleeding from the procedure, as well as the risks of discontinuing anticoagulant therapy. 5 US is widely used as a first noninvasive step and an easily accessible diagnostic method, in the detection and characterization of nodular thyroid diseases. 6 Although many suspicious findings have been obtained with US, in the evaluation of malignancy for thyroid nodules, the most accurate and effective diagnostic guidance was not fully established and until recently, had not translated to clinical practice. 7 For this reason, researchers have aimed to establish a standard reporting and data collection system by making standard US evaluations, with a consensus on thyroid nodules.6–8
Recently, several guidelines have been proposed for the risk stratification of thyroid nodules utilizing US. To this end, the Thyroid Imaging Reporting and Data System (TI-RADS) first identified divergent US patterns associated with malignancy for thyroid nodules by Horvarth et al 9 in 2009. Another study, conducted shortly after this study, proposed a similar system that classifies thyroid nodules according to 12 sonographic features. 10 The most widely used one today is the American College of Radiology (ACR) TI-RADS guideline. 11 Patients sent for a neck sonogram were evaluated with TI-RADS guideline according to the size (taller-than-wide), composition, shape, echogenicity, microcalcifications, borders, and echogenic foci of the nodule. Although these findings cause an underestimation when taken individually, the specificity of US and TI-RADS increased when more than one criterion was evaluated together. 12 The main purpose of this guideline was to determine whether the thyroid nodules require FNAB.9–12
FNAB is the next critical step in the examination of a thyroid nodule after identifying features that require biopsy with ACR TI-RADS on US. The Bethesda reporting system was used to indicate thyroid cytopathology and was developed before ACR TI-RADS to standardize thyroid cytology diagnoses. 13 According to this system, biopsy findings are optimally evaluated with clear management guidelines and associated malignancy risk. 14 Although surgery is recommended in cases where cytology is highly suspected, and sometimes in nodules with cannot be exact determined features, Bethesda category II or III nodules often require periodic follow-up with repeat FNAB and/or US procedures.13,14
Another recommended guideline for risk stratification of thyroid nodules by US is the American Thyroid Association (ATA) guideline published in 2015. 15 The risk of malignancy is <1% in pure cystic nodules, <3% in spongy nodules, and 10% to 20% in well-circumscribed hypoechoic solid nodules. Differently, in the presence of microcalcification/taller-than-wide/extrathyroidal extension, there is a risk of malignancy of around 70% to 90%. 16
The primary aim of this study was to evaluate the relationship between the ACR TI-RADS and the Bethesda reporting system, based on the final cytopathology in operated thyroid nodules. The secondary aim is to determine the usefulness of ACR TI-RADS in the diagnosis of thyroid nodules and biopsy decision in clinical practice.
Materials and Methods
This retrospective study was evaluated and approved by the institutional review board. Because human data were available, the Declaration of Helsinki was adhered to throughout the study. Written informed consent was obtained from each patient before procedures, indicating possible side effects and complications.
Patient Selection
Archived US examinations were performed for cases who underwent thyroidectomy for nodules in a tertiary center between May 2019 and May 2021. The cases with a history of subtotal thyroidectomy and/or antithyroid drug use, chronic thyroiditis, genetic syndrome, pure cystic/mixed type nodule presence, nodule size <1 cm, incomplete medical imaging-pathology data, under 18 years old, and multiple surgery were excluded from the study. As a result, 73 cases age ≥18 years with solid nodule pattern and nodule size ≥1 cm were identified and included in the study. All included cases had US data, ACR TI-RADS classification, Bethesda scoring, and final cytopathology results. In addition, 73 cases had total thyroidectomy, and no residual or recurrence was detected in the follow-up imaging and blood tests.
Thyroid Imaging and ACR TI-RADS
Preoperative B-mode US measurements and interventional radiology procedures for thyroid nodules were performed by an experienced radiologist. For each patient, TI-RADS classification (TR) was conducted for the dominant and/or suspected nodule for which FNAB was performed by the same physician. 11 Volumetric measurements were made on US images obtained in axial and sagittal planes using a 7- to 18-MHz linear transducer (Aplio 500, Tochigi, Japan) before biopsy (see Figure 1A and 1B). The formula V = π.(a.b.c)/6 (a = largest diameter, b and c = other vertical diameters in cm) was used to calculate thyroid nodule volumes. The US features of ACR TI-RADS such as composition, echogenicity, size, margin, microcalcifications, and echogenic foci were compared with the Bethesda system. 13
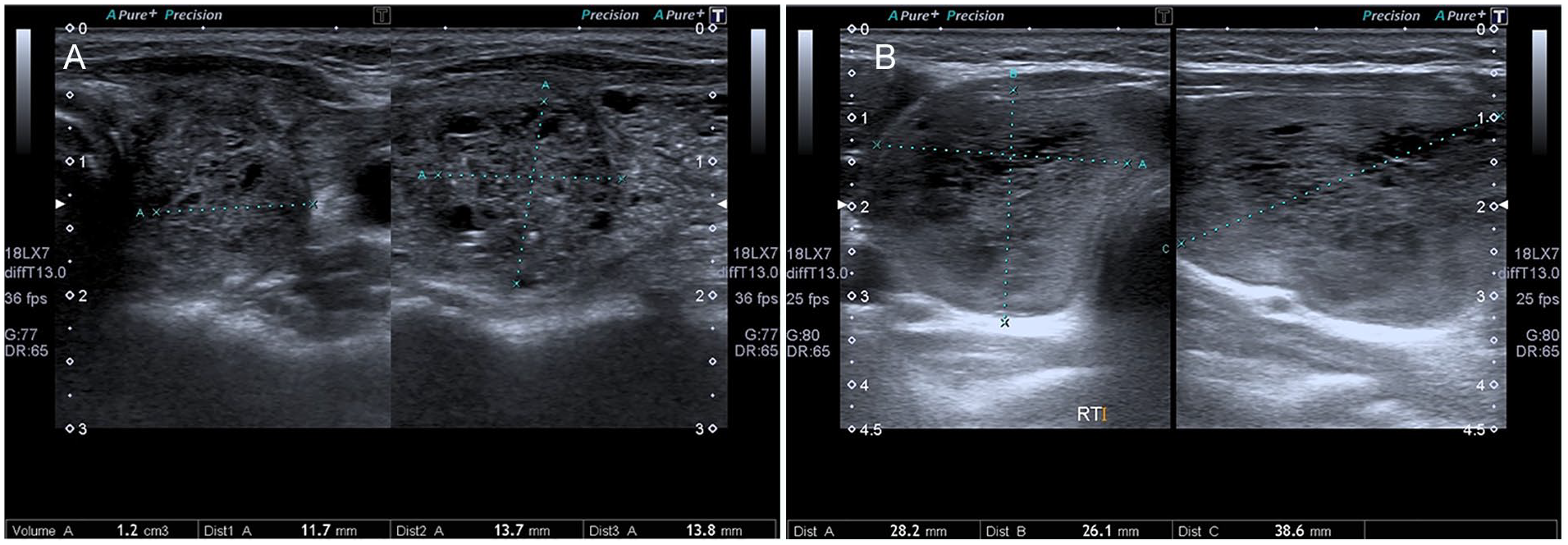
(A) A thyroid sonogram of a 46-year-old male case was evaluated before the biopsy; a suspicious nodular lesion with irregular borders, heterogeneous hypoechoic, microcalcifications and taller-than-wide size was observed in the left lobe, and was reported as TI-RADS 5. The FNAB result was Bethesda score 6 and was diagnosed as follicular carcinoma in the final pathology. (B) In the control sonogram of a 34-year-old female patient before thyroidectomy, a nodular lesion with irregular borders, heterogeneous hypoechoic, and almost solid composition was observed in the right lobe, and was reported as TR4. The FNAB result was a Bethesda score of 4 and the final pathology was diagnosed as a noncancerous lesion. FNAB, fine-needle aspiration biopsy; TI-RADS, Thyroid Imaging Reporting and Data System.
FNAB, Bethesda Scoring, and Final Pathology
FNAB was performed at least once in all cases before total thyroidectomy, and biopsy was repeated in the presence of Bethesda score 1.13,14 Total thyroidectomy was performed in 67 patients whose first biopsy and/or second biopsy result was Bethesda score ≥3. In six cases, although Bethesda score was 2, total thyroidectomy was performed due to developing significant dyspnea and dysphagia secondary to nodule compression. Bethesda scores were compared with final pathology results in all patients (see Figure 2). The samples of patients after thyroidectomy were examined and diagnosed according to the histological classification of thyroid tumors of the World Health Organization in 2017. 17

A total thyroidectomy specimen of a 52-year-old male patient is shown; there is a 12 × 16 mm nodular lesion in the inferior of the right lobe, indicated by an arrow showing extrathyroidal extension. The lesion had TR5 and a Bethesda score of 5 and was diagnosed as papillary carcinoma.
Statistical Analysis
Statistical analysis was conducted using SPSS software (SPSS version 23.0, IBM, Armonk, New York, US). Descriptive statistics (mean, standard deviation, median, maximum and minimum) were used for numerical data, and number and percentage values were used for categorical data. Kolmogorov-Smirnov test was used to determine whether the quantitative variables were normally distributed. Because the data were not normally distributed, the Mann-Whitney U test was used to compare the differences between the gender, and laterality. The statistical difference between categorical data (ACR TI-RADS and Bethesda scoring) was evaluated with chi-square test of independence and Fisher’s exact test. All analyses were performed at 95% confidence level, and P < .05 was accepted statistically significant.
Results
Of the patient cases included in the study, 28 (38.4%) were male and 45 (61.6%) were female. The median age was calculated as 45.00 (35.00–53.00) for all cases, 51.00 (36.50–58.50) in males and 41.00 (34.50–53.00) in females. In total, the minimum age was 21 and the maximum was 77, and both were female. For males, the minimum age was 23 and the maximum was 69 years. The median nodule volume was found to be 14.30 cm3 (9.04–25.55) in all cases, 13.45 cm3 (10.40–23.92) in males, and 15.60 cm3 (8.46–18.74) in females. The minimal nodule volume was 1.17 cm3 and the maximum 187.20 cm3, and both were male. In females, the minimal nodule volume was 1.49 cm3 and the maximum was 135.20 cm3. When the relationship between gender, age, and nodule volume was examined, no statistical difference was found (P = .140, P = .536).
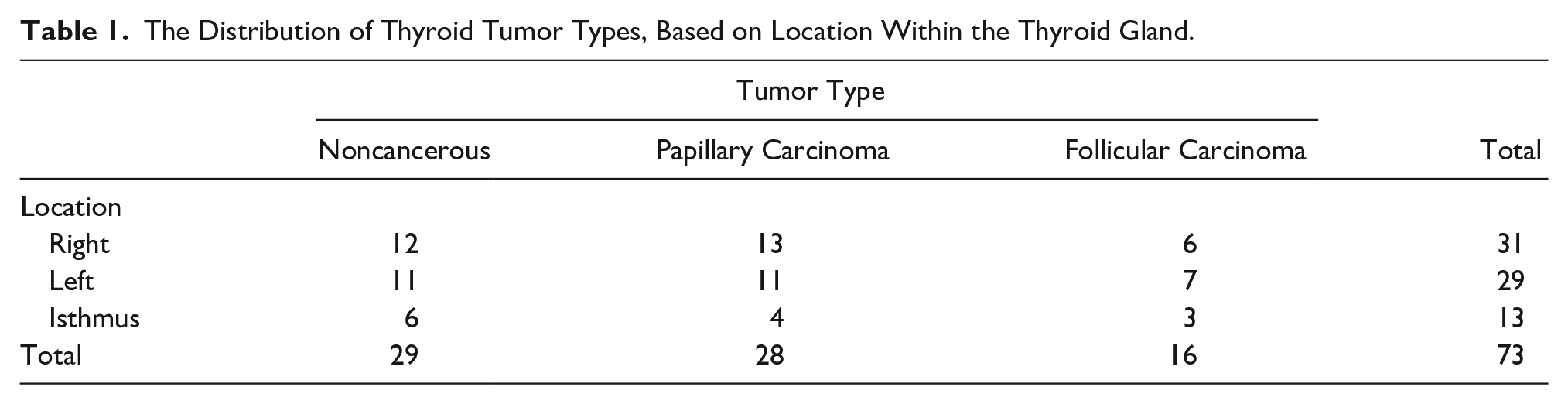
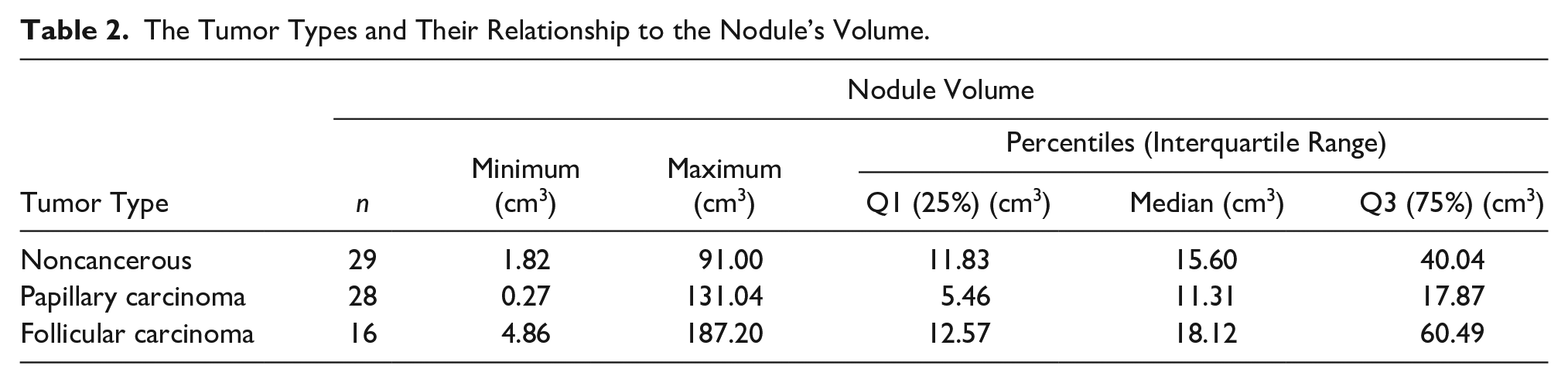
Nodular lesions with follicular adenoma, adenomatous, and diffuse hyperplasia as the final pathology result were collected under the title of noncancerous. No medullary or anaplastic carcinoma was detected in any of the 73 cases. The most commonly, noncancerous lesions (follicular adenoma, adenomatous, and diffuse hyperplasia) were present, followed by papillary and follicular carcinomas (see Table 1). There were 13 nodular lesions located in the isthmus that underwent thyroidectomy, and compared with other locations, there was statistical significance due to the number of cases (P = .026). Follicular carcinoma was less common than other lesions and there was a statistical difference (P = .038). When nodule volumes were compared according to tumor types, papillary carcinoma median nodule volume was less than other types, and there was statistical significance (P = .014) (Table 2).
The Distribution of Thyroid Tumor Types, Based on Location Within the Thyroid Gland.
The Tumor Types and Their Relationship to the Nodule’s Volume.
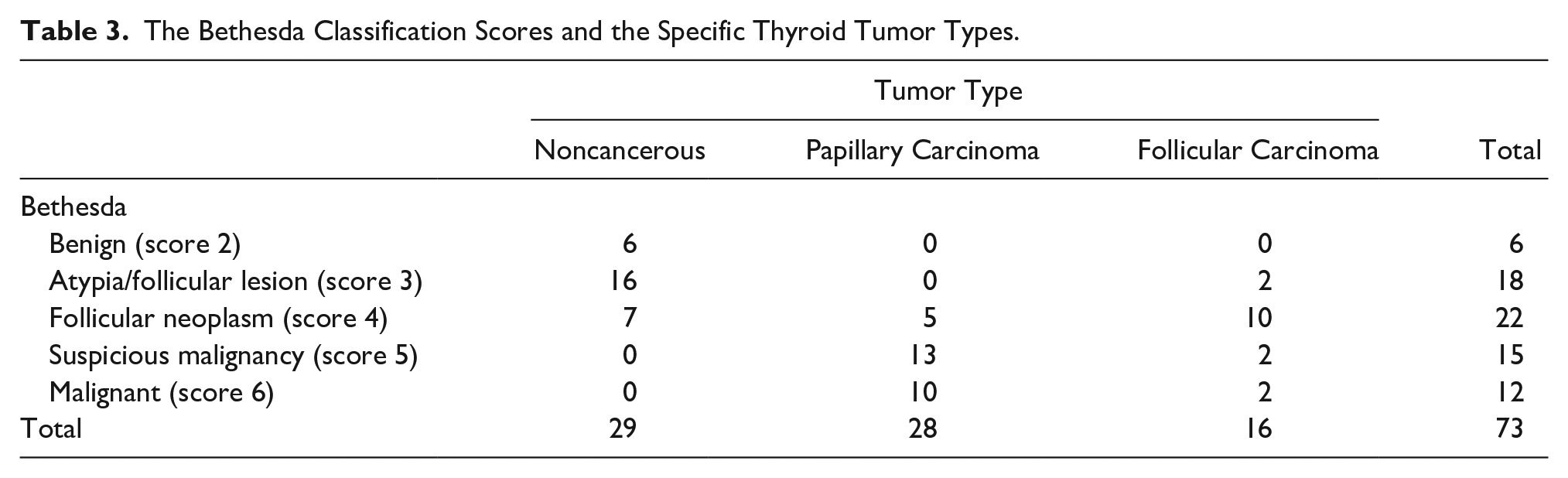
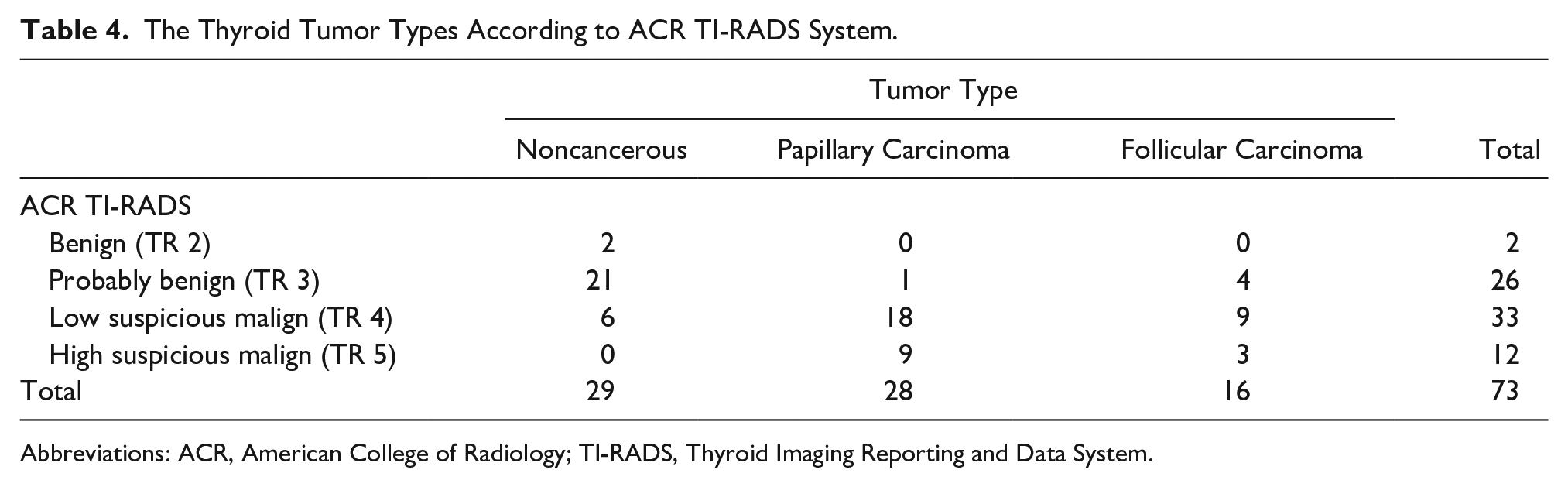
Tumor types were compared with Bethesda scoring system and 6 patients had a Bethesda score of 2 and none of them had cancer in the final pathology. Follicular carcinoma was detected in 2 cases with Bethesda score of 3, and the remaining 42 cancer cases were defined as Bethesda score 4 to 6 (see Table 3). In comparison with tumor types and ACR TI-RADS, two cases were TR2 and were detected to be noncancerous in final pathology. The final pathology of six nodular lesions diagnosed as TR4 was reported as noncancerous. Of the five cases with TR3, one had papillary carcinoma and four had follicular carcinoma. The score of 39 cancer patients was specified as TR4-5, and all 12 cases with TR5 were cancer (see Table 4).
The Bethesda Classification Scores and the Specific Thyroid Tumor Types.
The Thyroid Tumor Types According to ACR TI-RADS System.
Abbreviations: ACR, American College of Radiology; TI-RADS, Thyroid Imaging Reporting and Data System.
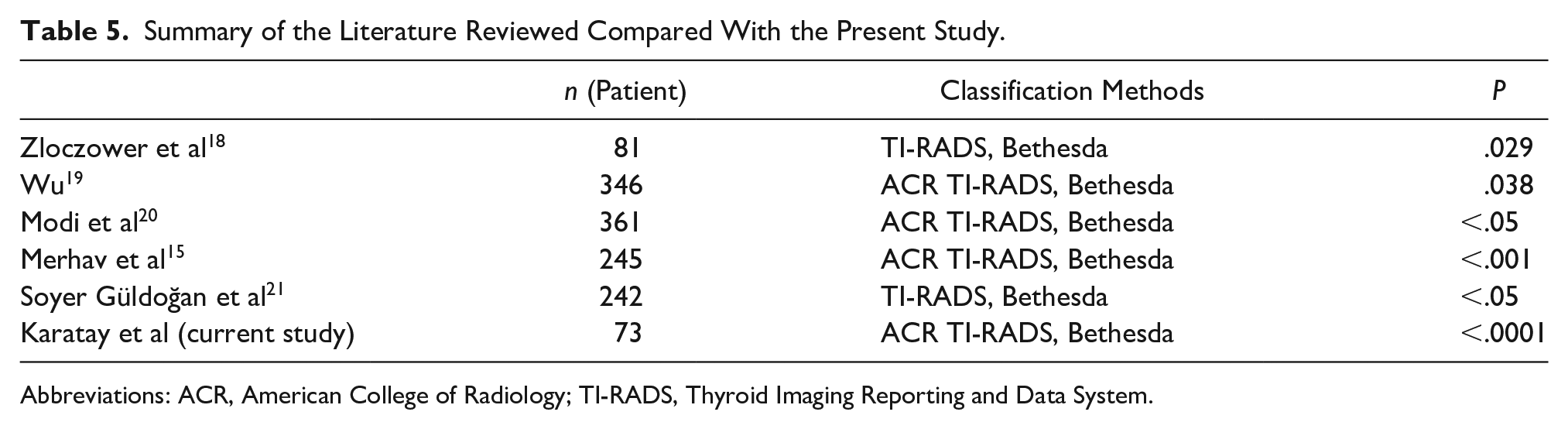
According to Spearman correlation analysis, a very strong positive relationship was found between Bethesda scoring system and ACR TI-RADS scores (ρ = 0.832, P < .0001). A 94.4% sensitivity and 65.4% specificity were found in 16 patients with Bethesda score of 3 and TR3 based on final pathology (P < .001). And a sensitivity of 77.3% and specificity of 51.5% were found in 17 patients with a Bethesda score of 4 and TR4 (P < .001). Finally, a sensitivity of 55.6% and specificity of 50.0% was found in 17 patients with a Bethesda score of 6 and TR5 (P < .001). There are only a few studies evaluating Keros types in the literature, and the present study data are compared and summarized in Table 5.
Summary of the Literature Reviewed Compared With the Present Study.
Abbreviations: ACR, American College of Radiology; TI-RADS, Thyroid Imaging Reporting and Data System.
Discussion
Previous studies have shown that the prevalence of palpable thyroid nodules is approximately 5% in the population. In addition, thyroid nodules are seen in up to 70% of adults in US examinations of the thyroid gland.1,2 The clinical significance of thyroid nodules is the need to exclude thyroid cancer, which may occur in 5% to 15% of cases, depending on age, gender, radiation exposure, and family history. 3 Although FNAB is the primary test of choice to determine the structure of nodules under US-guidance, only 5% to 15% of all nodules are malignant. Moreover, even nodules proven to be malignant by cytology, especially when smaller than 1 cm, are usually not clinically significant and show nonaggressive behavior. 4
Especially in the last 10 years, several TI-RADS systems have been developed to improve the risk stratification of thyroid nodules using US.9–11 Today, the most commonly used ACR TI-RADS identifies more clinically significant nodules to reduce unnecessary biopsies performed on benign nodules. 11 The US features suspicious for malignancy include a hypoechoic/very hypoechoic solid component, lobulated or irregular margin, extrathyroidal extension, taller-than-wide shape, and the presence of microcalcifications. 12 The US features in TI-RADS are categorized as benign (TR1-TR2), mildly suspicious (TR3), moderately suspicious for malignancy (TR4), or highly suspicious for malignancy (TR5). A malignancy risk according to ACR TI-RADS levels; TR5 is ≥20%, TR4 is 10% to 20%, and TR3 is 5%.11,12
In a study by Zloczower et al with young adults, TI-RADS and Bethesda scores were compared in 91 thyroid nodules. A greater agreement was found between the two classifications in males (87.5%) than in females (77.6%), and all operated benign nodules had lower TI-RADS and Bethesda scores. And of the eight malignant cases that underwent a surgical operation, six had high TI-RADS and five had high Bethesda scores. 18 In another study, TI-RADS was modified and classified into six categories, and TR5 was defined as suspicious and TR6 as highly suspicious malignant lesion. A moderate positive correlation was found between overall Bethesda and TR scores (r = 0.465). It was noted that modified TI-RADS correlated slightly better than ACR TI-RADS. 19 Modi et al evaluated 361 thyroid nodules classified by ACR TI-RADS and showed that this classification is more successful in detecting malignant lesions. A Bethesda score of 6 was noted in 14 cases with TR5; however, it was found that ACR TI-RADS was more successful, especially in TR4 and TR5 categories. 20
In another study, besides both of the aforementioned scoring systems, the ATA risk classification was added to the evaluation. The effectiveness of ATA and ACR TI-RADS was compared in 235 nodules according to the Bethesda scoring and it was noted that TI-RADS was more successful in reducing unnecessary biopsies. 15 Guldogan et al evaluated the effect of TI-RADS in detecting thyroid malignancies in 242 patients and found that TI-RADS criteria and FNAB results showed a significant relationship with suspicious US findings. In addition, it was stated that the effective use of TI-RADS in ultrasound follow-ups in thyroid nodules with low TR scores could prevent unnecessary biopsies and thyroidectomies. 21
What made the present study different from almost all of the other studies was that it had final pathology results as well as Bethesda scores.15,19,20 The current study has the highest positive correlation reported in the literature between the ACR TI-RADS and the Bethesda system. The reason why this very strong positive correlation (ρ = 0.832) was found between both classifications may be the intense focus on the Bethesda scoring system and the ACR TI-RADS relationship. Unlike other studies, all of the US, FNAB procedures, and thyroid surgeries were performed in the same center in this study.15,18–20
Limitations
There are a few limitations based on this cohort study, such as the design and convenient sample. The next limitation of this study was the relatively small number of male cases. An additional limitation was that the follow-up period for the patient cases was rather short. Another limitation was that there is only one TI-RADS score obtained before the biopsy for all patients. Finally, the fact that there are few studies comparing malignancy with both scoring systems can be considered an added limitation.15,18–21
Conclusion
The routine use of the ACR TI-RADS classification for thyroid nodules in daily practice could help to prevent unnecessary FNABs. In addition, it can also be effective in reducing costs by providing guidance in minimizing complications that may develop secondary to FNAB and thyroidectomy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the University of Health Sciences Ethics Committee.
Informed Consent
All patients included in this study gave written informed consent to participate in this research.