
Abstract
For more than two decades, surveys of imaging technologists have consistently reported high prevalence of work-related musculoskeletal discomfort (WRMSD). Yet, workplace intervention research involving sonographers is limited. In this study, a transdisciplinary team of researchers used a participatory approach to work with diagnostic medical sonographers (DMS) and vascular technologists (VT) to identify needs and opportunities for developing new approaches to work that will reduce sonographers’ exposures to WRMSD risk factors. In this paper, we describe the approach and the resulting identified needs. We also describe the prototyping and testing of two work approaches that target specific needs of DMS and VT, respectively. We would like designers, manufacturers, engineers, and ergonomists, in collaboration with sonographers and their managers, to recognize this area of opportunity and come together to apply their knowledge of biomechanics and design in developing useful and usable workplace interventions (solutions) to reduce sonographers’ WRMSD risk factor exposure.
Introduction
For more than two decades, published studies have consistently shown that high percentages of sonographers experience musculoskeletal (MSK) symptoms associated with their work, regardless of the country in which the work is performed. A 1996 survey of sonographers in the US states of Washington and Oregon found that 66% of the 149 respondents were symptomatic. 1 In 2002, a survey involving 92% of sonographers in British Columbia (211 respondents) reported that 80% were experiencing pain at the time of the survey, the pain began after they started their sonography careers, and 68% experienced pain while working. 2 In a large survey of US and Canadian sonographers, 90% of the 2963 participants reported that they were in pain while scanning. 3 Two recent surveys of sonographers in China both found that the 12-month prevalence of MSK discomfort exceeded 98% (n=232 and 567 respondents, respectively).4,5 Factors associated with MSK pain in multiple studies include shoulder abduction, holding awkward postures for extended periods of time, applying sustained pressure with the hand-held transducer, forceful gripping of the transducer, and scanning larger patients, among other factors.2,6,7 Average push and grip forces on the transducer have been estimated to range from 8 to 80 N, depending on the scan type and location. Using an instrumented transducer, measured mean and maximum applied axial forces exerted during abdominal scans of healthy volunteers were 7.9 and 17.4 N, respectively, for volunteers with BMI in the range of 18.5-25 (healthy weight category) and 10.5 and 23.5 N, respectively, for volunteers with BMI > 25. 8 Burnett and Campbell-Kyureghyan 9 published mean estimates of about 70 N of push force during lower extremity venous scans, by employing a force-matching technique. Based on electromyographic data, Village and Trask 10 estimated that mean forces during VT scans (lower extremity, renal) on actual patients ranged from 60 to 80 N.
Recommendations for interventions to reduce exposure of sonographers to risk factors for work-related MSK symptoms have been published in peer-reviewed journals,7,11 by professional societies,12-14 and by government agencies. 15 Yet new surveys of MSK pain in sonographers continue to be published,16,17 in spite of existing intervention recommendations. This suggests that the interventions are not being adopted or are in other ways insufficient to impact the prevalence of MSK pain in sonographers.
The objective of the current study was to involve diagnostic medical sonographers (DMS) and vascular technologists (VT) in a participatory process with the following research goals: 1) discussion of challenging conditions and activities at work that the sonographers associate with physical stress and musculoskeletal discomfort; 2) joint development of ideas by the researchers and participants for new methods and devices that would be effective at reducing the physical stress. The new methods and devices had to be viewed as useful and usable by the imaging technologists, and feasible to implement by their managers. This level of intervention research is considered to be “Developmental Research” within the Intervention Research Process described by Goldenhar et al. 18 This effort was part of a larger study to involve participants and researchers in jointly developing interventions for five types of imaging technologists: DMS, VT, cardiac sonographers, 19 mammographers, 20 and radiographers.
The study was conducted in three phases: needs assessment (Phase 1), concept review (Phase 2), and prototyping efforts and pilot studies (Phase 3). This paper focuses on DMS and VT participation and addresses some of their unique needs.
Phase 1 – Needs Assessment
There were four steps in the Needs Assessment Phase of the study: 1) needs discovery via creativity-based focus group workshops with practicing DMS and VT, 2) needs analysis of the workshop data, 3) generation of intervention concepts, and 4) prioritization of intervention concepts based on feasibility and project scope. The Needs Assessment Phase (Phase 1) produced several intervention concepts that were subsequently reviewed by DMS and VT in the Concept Review Phase (Phase 2) of the study.
Needs Assessment Methods
There were 15 participants (12 women, 3 men; with 4 to 32 years of experience in sonography); each participated in one workshop. Two workshops were devoted to DMS (9 participants in total) and one to VT (6 participants). Participants completed a workbook prior to attending a workshop consisting of focus group discussion and a collaborative activity to generate intervention ideas.
Workbooks provided participants a means for describing their background, work tasks, work environment, equipment, and patients. They included several pages of questions, a two-day work diary, and a photo album to help participants show the challenging aspects of their work to the research team. Workbooks were completed in advance of the workshop to foster reflection and priming, and to prepare the participants to participate fully in the workshop. By reviewing the workbook contents prior to the session, researchers were able to include examples of each participant’s concerns in the discussion.
The process steps were identical in each workshop: introductions, review of some workbook entries and discussion of selected workbook photographs submitted by participants, (issues) card sorting and voting to identify participants’ high priority issues based on the discussion, and an activity to generate intervention ideas. The latter was a co-design activity in which these potential users were given a tool kit to facilitate creative collaboration in addressing their high priority issues. 21
Workshop data were analyzed separately for DMS and VT. Workbook entries were entered in spreadsheets for subsequent review, notes were made from audio recordings of discussions and co-design activity solution presentations, and workbook photos and co-design video presentations were all analyzed for thematic and specific content. Through detailed review of these materials (thematic analysis), a document was created for each type of sonographer, which was organized by several major categories that emerged from the data (such as Pannus support, Sonographer working posture, Patient positioning, Equipment design, etc.). Within each category, all expressed needs were documented, along with the source (workbook entry, focus group discussion, etc.), the interpretation of each expressed need, initial intervention ideas to address the need, an initial feasibility rating of prototyping and/or testing the idea, and researcher notes. VT data and DMS data were analyzed by two different pairs of researchers. Each researcher independently completed an analysis and then each pair of researchers worked together to develop an analysis for their group, which they presented to the whole research team for further analysis and final consensus.
The next step was to develop intervention categories (for example, Patient positioning, Sonographer working posture, Equipment design, Room design, etc.) along with a list of intervention concepts for each category and sonography group. Several brainstorming techniques, internet searches, and literature searches were used to generate intervention concepts.
The next step was refining and reducing the number of concepts to those that were most promising and that fell within the scope of the study. The team evaluated each concept on feasibility, extent to which the concept addressed the objectives of the study (affecting the MSK health of DMS and VT), and timeline of the project. The concepts that passed through this step were then discussed with the VT and DMS in separate concept-review sessions (Phase 2).
Needs Assessment Results
All 15 workshop participants reported experiencing work-related MSK discomfort. When asked to describe the most physically demanding exam or procedure they perform on a regular basis, and reasons that made the exams so demanding, they described exams that required repeated and/or continuous forceful pushing with the transducer, particularly involving obese patients. Estimates of percentages of their patients that were heavy or obese, as determined by the sonographers, ranged from 20% to 75% for VT and from 30% to 90% for DMS.
There was some overlap between DMS and VT and some sub-specialty-specific concerns in the main themes that emerged from the focus group discussions. Common issue-clusters across the groups (and examples of some issues) were body strain/physical demands (issues included shoulder pain and exam factors that put a strain on the body, such as handling unsteady patients or examining obese patients, applying pressure with the transducer), equipment (including transducer design, keyboard and controls design, and transducer cord management), portable exams (including issues with lack of space, scanning in awkward postures, bed-height control, and lighting controls), workflow (including time pressure and paperwork), and room and furniture design (including small exam rooms, inconvenient gel-warmer location, problems with computer workstation space and layout, furniture with limited adjustability). Transvaginal exams presented a unique cluster of issues for DMS, while VT reported unique issues associated with augmentation and reflux studies. The needs assessment analysis results appear in Table 1.
Results of Needs Assessment Analysis.
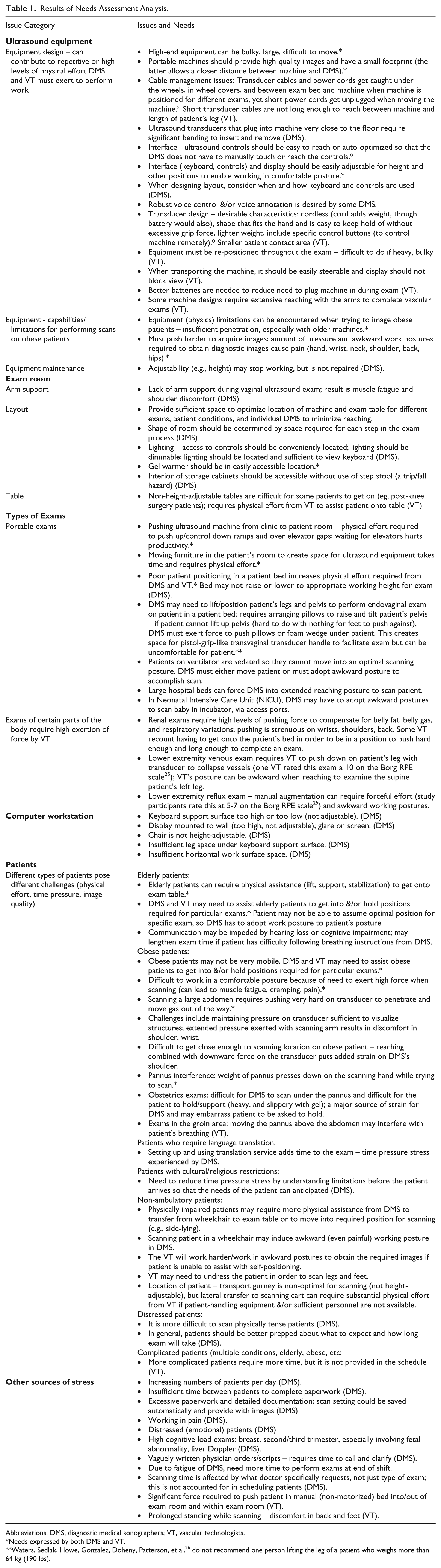
Abbreviations: DMS, diagnostic medical sonographers; VT, vascular technologists.
Needs expressed by both DMS and VT.
Waters, Sedlak, Howe, Gonzalez, Doheny, Patterson, et al. 26 do not recommend one person lifting the leg of a patient who weighs more than 64 kg (190 lbs).
Brainstorming and other idea-generating activities yielded a total of 45 intervention concepts to address the interpreted needs of the DMS and 66 for VT. After categorizing these concepts as either low-hanging fruit, blue sky, or somewhere in between, and either within the scope of the project, close, or out-of-scope, the screening analysis yielded 14 intervention concepts to present to the DMS and 15 for VT (see Tables 2 and 3).
Concepts Presented to Diagnostic Medical Sonographers in the Concept Review Session.
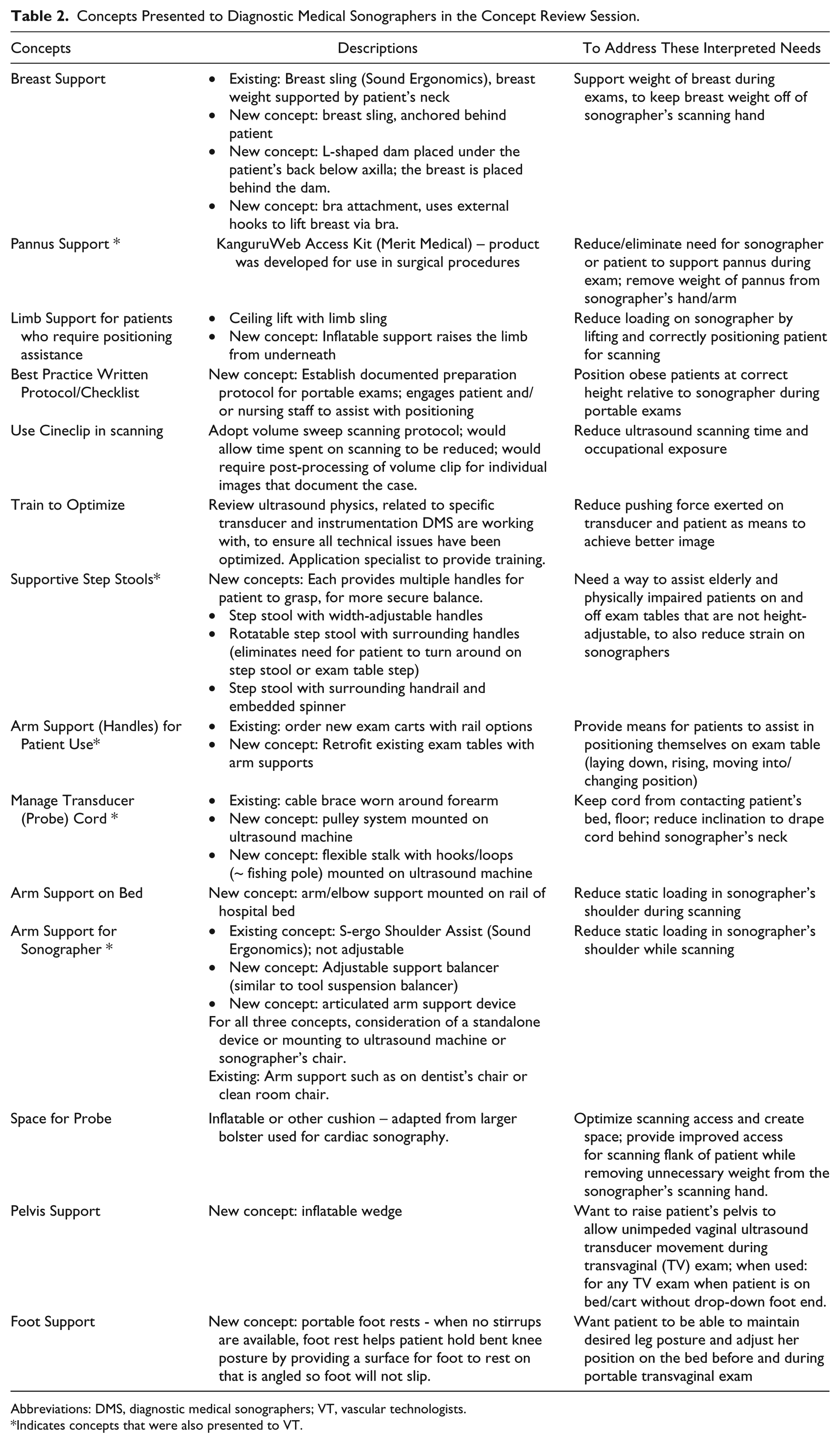
Abbreviations: DMS, diagnostic medical sonographers; VT, vascular technologists.
Indicates concepts that were also presented to VT.
Concepts Presented to Vascular Technologists in the Concept Review Session.*
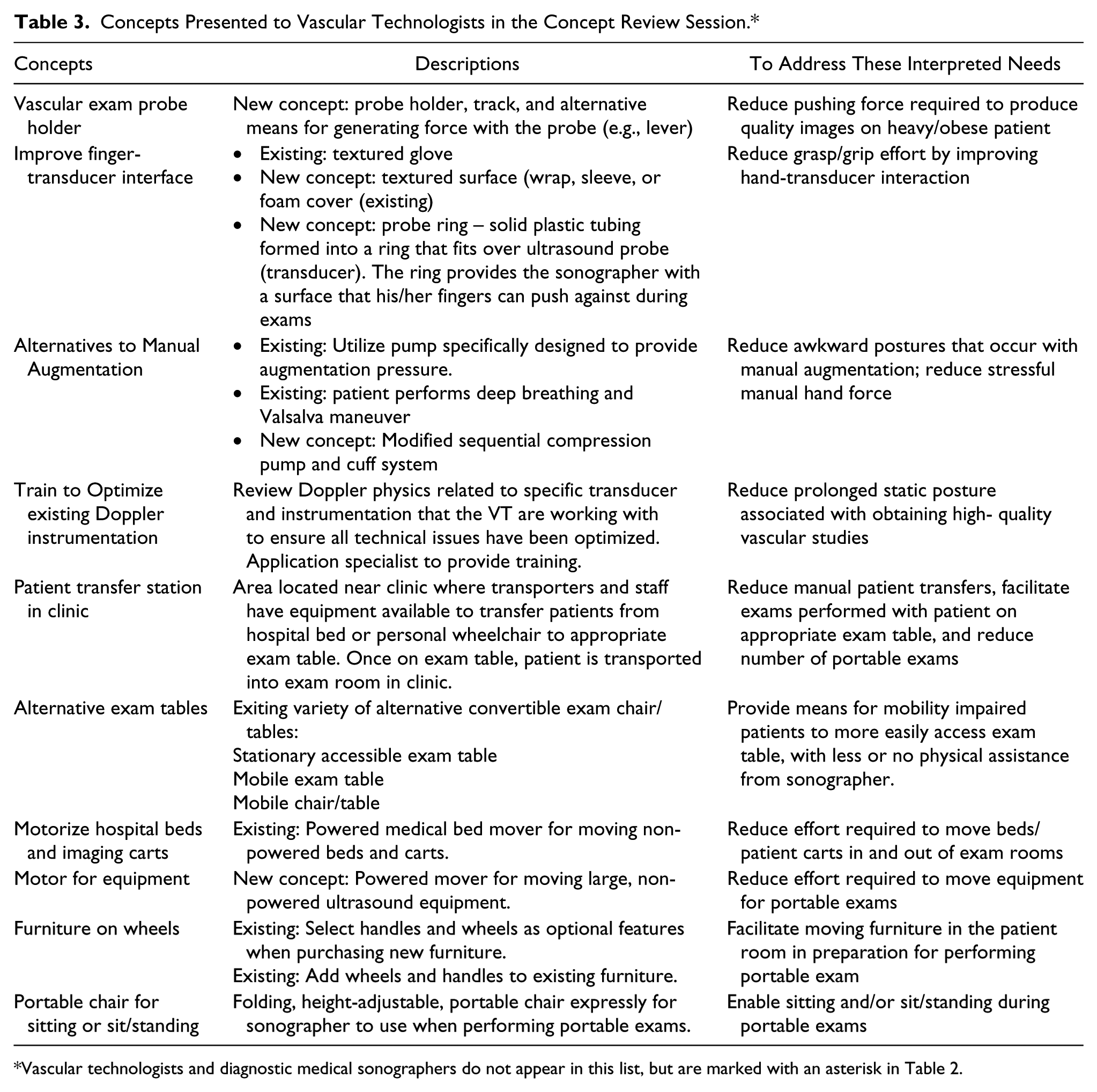
Vascular technologists and diagnostic medical sonographers do not appear in this list, but are marked with an asterisk in Table 2.
Phase 2: Concept Review
Concept Review Methods
Six DMS and 12 VT participated in this phase of the study (17 women, 1 man; 3 to 32 years of experience). Seven of the participants were new to the study.
Posters and some prototypes were presented to the participants who used evaluation forms and discussion to provide their opinions on the usability, usefulness, and desirability (UUD) of each concept, potential barriers they anticipated to using or implementing them, and suggestions for improvement. Each concept was presented separately, participants were given time to ask questions, and then time to complete their evaluation. VT reviewed 15 concepts and DMS reviewed 14. Interaction and role-playing with prototypes was encouraged. After participants completed their evaluation form, the next concept was presented.
Usability items on the evaluation form included ease of use and ease of learning to use. Usefulness addressed predicted effects on physical effort, fatigue, and efficiency of the sonographer, as well as patient comfort. Desirability addressed extent of interest in using the intervention by the study participant and his/her co-workers. Participants used a 5-point response scale (Strongly Agree to Strongly Disagree) to respond to each statement. Participants also provided an overall rating of each category, using a range of 1 (very poor) to 7 (very good). Example: “My overall rating of its potential usefulness is ____.” After reviewing all the concepts, participants were asked which concepts should continue to be developed or pursued. They were each given six green voting dots to distribute among the concept(s) they chose.
Data from the concept review sessions were analyzed separately for VT and DMS. Evaluation form data were entered in spreadsheets and median values and spreads of scores were calculated for each UUD item (statement) regarding each concept, along with the numbers of voting dots and anticipated barriers.
Concept Review Results
Results from the DMS and VT evaluation forms are summarized in Figures 1 and 2, respectively. For each concept, results include overall scores of potential usefulness, usability, and desirability (scale 1-7), the number of priority (green) voting dots received, and the number of barriers noted normalized to the number of participants.
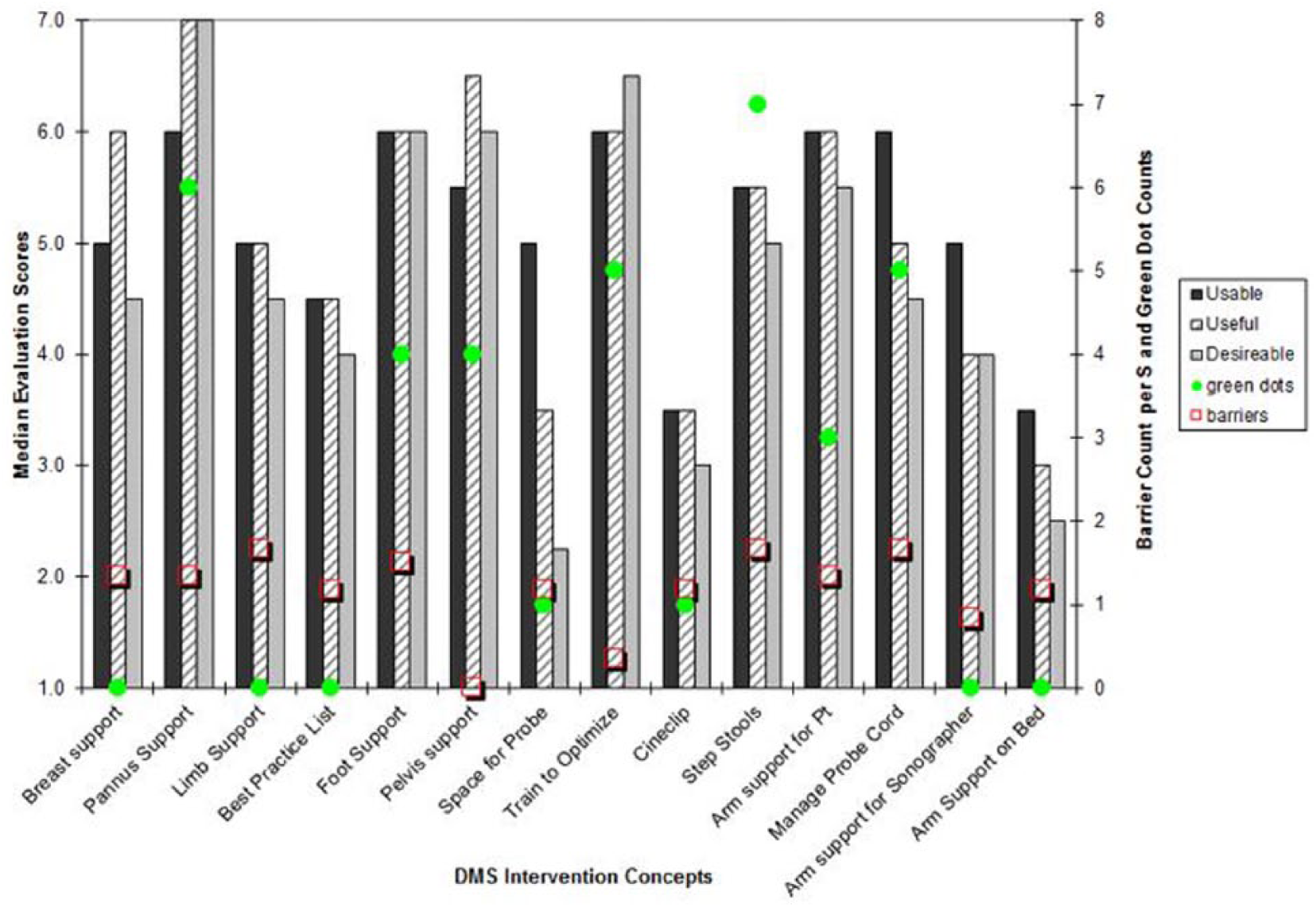
Diagnostic medical sonographers’ evaluations of intervention concepts.
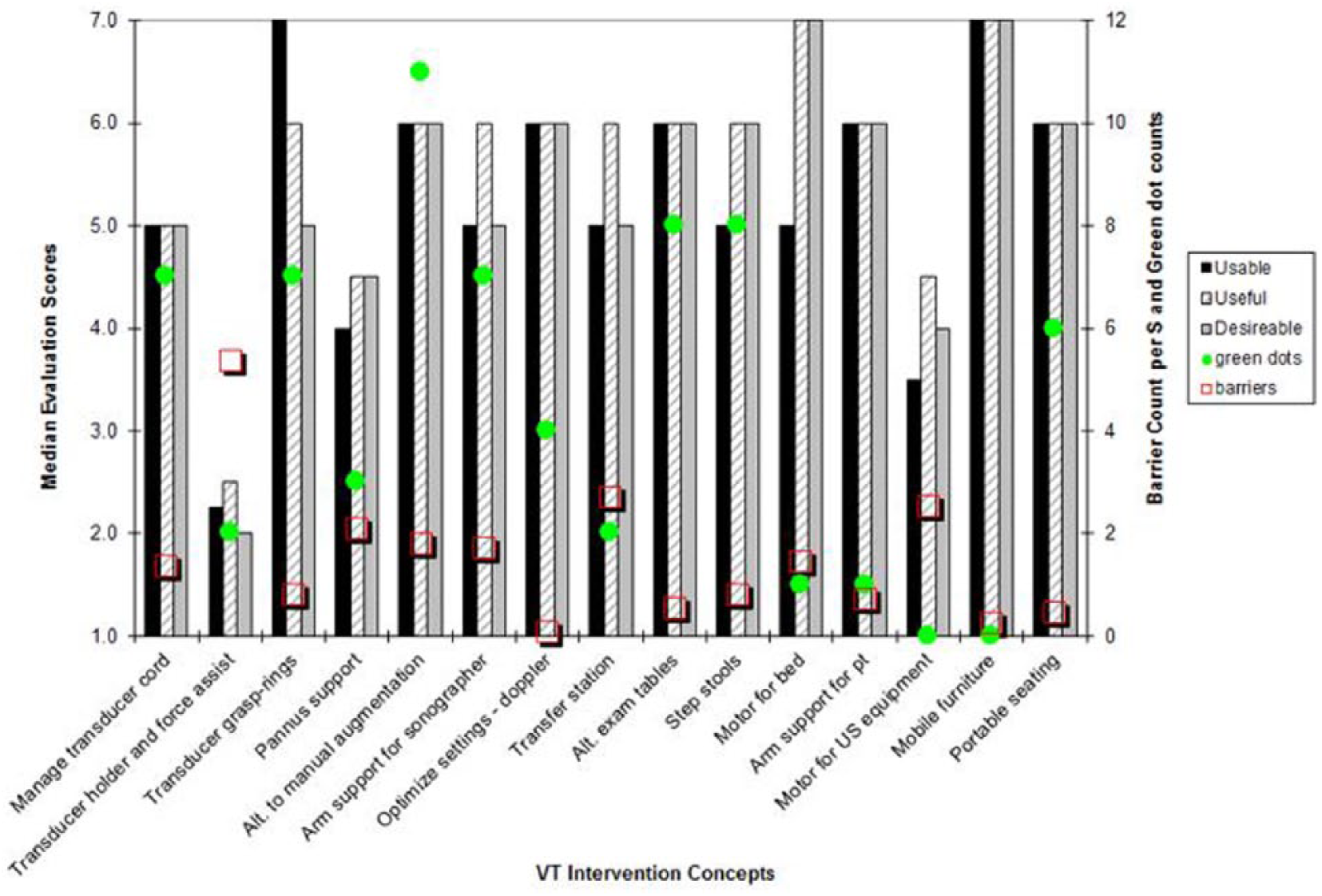
Vascular technologists’ evaluations of intervention concepts.
Although many concepts were evaluated positively by the concept review participants, after examining the results from the concept review sessions for all five groups of imaging technologists, a list of the ten most promising new concepts or underutilized existing solutions that could be examined further within the limits of the study was developed. These ten items were the focus for the remainder of the study. Further work is described concerning two of the ten most promising; each addresses a unique need for DMS and VT.
Phase 3 – Intervention Prototyping and Pilot Testing
Two of the high priority/high promise interventions, one specific to DMS and one to VT, are presented in this section. For each intervention, we begin by providing some additional context (background and specific results from the earlier phases of the project pertaining to the specific concept), before describing the particular approach taken to further investigate each concept.
Pelvis Support Intervention for DMS Patients
The need for a pelvis support was conceived to make it easier and more comfortable for a DMS to raise a patient’s pelvis, thereby allowing for unimpeded transducer movement during transvaginal exams. Often transvaginal sonographic exams are conducted on a bed/cart that does not expressly support transducer movement. As recommended by Gill 22 , “Ideally, a gynecologic table with stirrups and a break-away feature allows for easy performance of the vaginal exam. If such a table is not available, elevate the patient’s hips so that the transducer can be manipulated properly for adequate visualization of the uterus and ovaries. This can be accomplished by using sponges or a stack of sheets placed under the hips.” Unfortunately, patients who are in a patient bed or on a gurney from the Emergency Department often cannot be placed in the lithotomy position for insertion of the probe and proper scanning of the female pelvis. If the patient is not elevated and placed in the lithotomy position, the handle of the transvaginal probe is limited or blocked from proper scanning maneuvers.
In the Evans, et al. 3 study of US and Canadian sonographers and vascular technologists, of those who reported scanning in pain (89% of 2963 participants), 32% reported pain in their elbow/forearm, 50% in their wrist, and 44% in the hand/fingers. In Phase 1 of the current study, several DMS attributed discomfort, in part, to transvaginal scanning due to not having the proper positioning to insert the transducer and they reported often experiencing temporary pain when trying to obtain the best possible images under these constrained conditions. In addition to difficulties performing the scan, sonographers will attempt to elevate the patient to put her into a somewhat better position for scanning by placing several pillows under the patient. For patients that are not able to cooperate with the sonographer, the DMS may have to try to lift the patients’ legs or bottom or just push with great effort, in order to get the pillows underneath the patient. This patient handling aspect of the exam adds considerable effort and risk of injury to the sonographer. Given this injury risk and potential for inferior diagnostic image quality, the research team worked with the sonographers to identify or develop ways to properly reduce awkward postures and promote proper position of the patient for transvaginal sonography.
The idea of a portable, inflatable pelvic support wedge that could be positioned in its uninflated state under the patient, and then inflated to raise and tilt the patient’s pelvis as much or as little as needed for the exam came to the team through brainstorming sessions and was inspired by the DMS needs assessment workshop. An early conceptual prototype, an inflatable bed wedge, was shown to the DMS during the concept review session (Figure 3a, b). Even at that early stage, the pelvis support concept received high overall scores for potential usability, usefulness, and desirability (5.5, 6.5, and 6 out of 7) and no potential barriers were identified by the concept review participants.
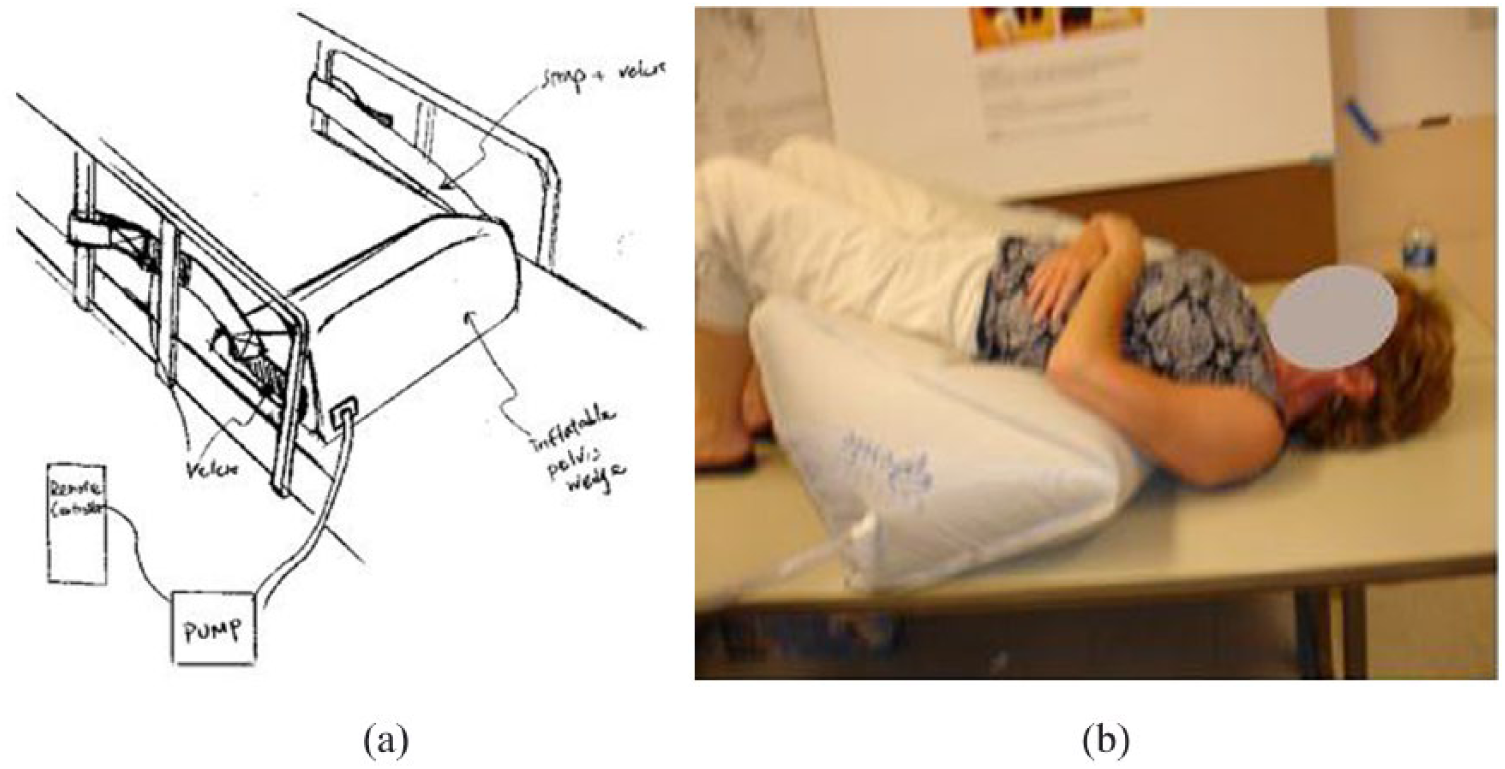
(a) Sketch of inflatable pelvic support; (b) sonographer interacting with inflatable, adjustable “bed wedge” mattress pillow during concept review session.
While at a patient handling conference, research team members began discussions with a manufacturer on development of a prototype pelvic support wedge based on a modification of an inflatable intubation wedge made by the manufacturer. Subsequently, several iterations of the pelvic support wedge were provided by the manufacturer. Each was shown to the sonographers who provided important suggestions for improvements (Figure 4a-e). Guidelines for cleaning and disinfection were also jointly developed by the research team, hospital staff, and manufacturer.

Prototype development and refinements of the inflatable pelvic support wedge.
After speaking further with our DMS partners, another potential benefit to the pelvic support wedge was recognized. In addition to the benefit of being able to properly position patients who are in a patient bed or on a gurney for a transvaginal exam, this type of pelvis support could also reduce exposure to risks associated with lateral patient transfers in an ultrasound clinic. Currently, when patients come to an outpatient clinic within a hospital for this exam, they are put on an exam cart with a drop-out foot end. For patients who arrive at the clinic on a gurney or in a hospital bed, leaving them on the bed or gurney for the exam would eliminate two lateral transfers, both of which are occasions when injuries can occur to patients and/or staff.
In making plans to test the pelvic support, the FDA determined that it was different enough from current patient positioning technologies that it would require FDA 510(k) clearance. The manufacturer did not have the personnel capacity to address this issue at the time, and so the pelvic support was not pursued further. We believe it remains a highly viable concept.
Force Augmentation Intervention for VT
Several examinations of the lower extremity performed by VT require augmentation, including vein mapping, venous duplex evaluation, and venous insufficiency evaluation. 23 Augmentation is the increase in blood flow in response to muscle contraction, either by the VT compressing the muscle or by the patient contracting the muscle. The purpose of augmentation is to demonstrate that the veins are patent and blood moves retrograde during the sonographic examination. As expressed through the workbook and workshop (Phase 1), VT concerns with augmentation included exerting the pushing force to coapt veins, particularly in obese patients, and working in awkward postures to do so (Figure 5). Subsequently, in the concept review session (Phase 2), “alternatives to manual augmentation” received the largest number of priority votes from the participants (Figure 2), and median scores of 6 for potential usability, usefulness, and desirability. Participants were shown three alternative approaches: 1. augmentation from a pump specifically for use in venous examinations (existing, but not widely used); 2. modified sequential compression pump and cuff system (a concept); and 3. patient performs deep breathing and Valsalva maneuver (can be done now; requires patient to follow instructions, and extent of compliance can affect study results). The greatest interest was in the augmentation pumps, so a pilot study was designed to investigate their usability and usefulness.

Workbook photograph provided by vascular technologist, self-titled “Poor Ergonomic Scanning”, was accompanied by written and verbal descriptions of a physically demanding exam.
Two venous augmentation pump systems were used in the study. VenaPulse Model VP-25 (ACI Medical, LLC) and E20 Rapid Cuff Inflator (D.E. Hokanson, Inc.). The objective of the testing was to assess the usability and usefulness of the devices and to determine any barriers to the adoption of one or both pieces of equipment.
A preliminary pilot study of the two devices was completed by two credentialed vascular sonographers. An imaging protocol was developed for a limited lower extremity venous study. The two sonographers worked independently with the same pseudo-patient, performing the study using both manual and powered augmentation. The images were saved on a GE Logic 9 ultrasound machine. The images were compared and graded for completeness and image quality. The image analysis demonstrated no differences between the manual and powered augmentation systems, regardless of sonographer.
Two exam rooms were set up similarly, each with a GE Logiq 9 ultrasound machine, a volunteer pseudo-patient, and both powered venous augmentation units for evaluation. Seven sonographers (2 male, 5 female; each with 2 to 25 years of professional experience) participated, individually, in the usability session. Each sonographer completed 3 scans on a single psuedo-patient: one exam with manual augmentation and the other two with augmentation, using each device. The scans followed an abbreviated Venous Duplex Examination protocol. The use order of the two devices was counter-balanced between study participants; all participants performed the manual exam first. Participants received instructions on how to use the inflation systems and were given the opportunity to practice using each system until they were comfortable with it. The choice to sit or stand to perform the exams was left to the participants; they were instructed to position themselves and the ultrasound equipment as they normally would. The VenaPulse was operated using a foot pedal, and the E20 was operated using a hand switch positioned on the ultrasound machine.
Dependent measures included usability, usefulness, and desirability (UUD) assessments from the sonographers and work posture assessments made by the research team. The UUD assessments were similar in nature to the UUD assessments provided in the concept review sessions. However, at this stage, the UUD assessment questions were specific to the features and design elements of the devices being evaluated.
The postural improvements were clearly visible when comparing the standard manual augmentation method to the inflation system method. The manual method requires the vascular technologists to extend their reach of both hands and arms to the patient’s leg as well as to grip the patient’s leg. This results in the adoption of awkward twisting postures of the torso and/or neck due to the need to continue looking at the display screen while providing the manual augmentation and scanning with the transducer, simultaneously. In comparison, the vascular technologists were able to adopt more neutral postures when using the augmentation pumps. This difference was observed regardless of whether the VT stood or sat to perform the exams. Postural assessment using the Rapid Entire Body Assessment (REBA) observational assessment tool 24 was performed on representative postures during manual and powered augmentation for VTs who chose different work postures. In each case, use of a powered augmentation device resulted in lower (better) REBA scores (Figure 6). Postural differences between the two inflation systems were not apparent. Both configurations facilitated adoption of a more neutral working posture during the exam.
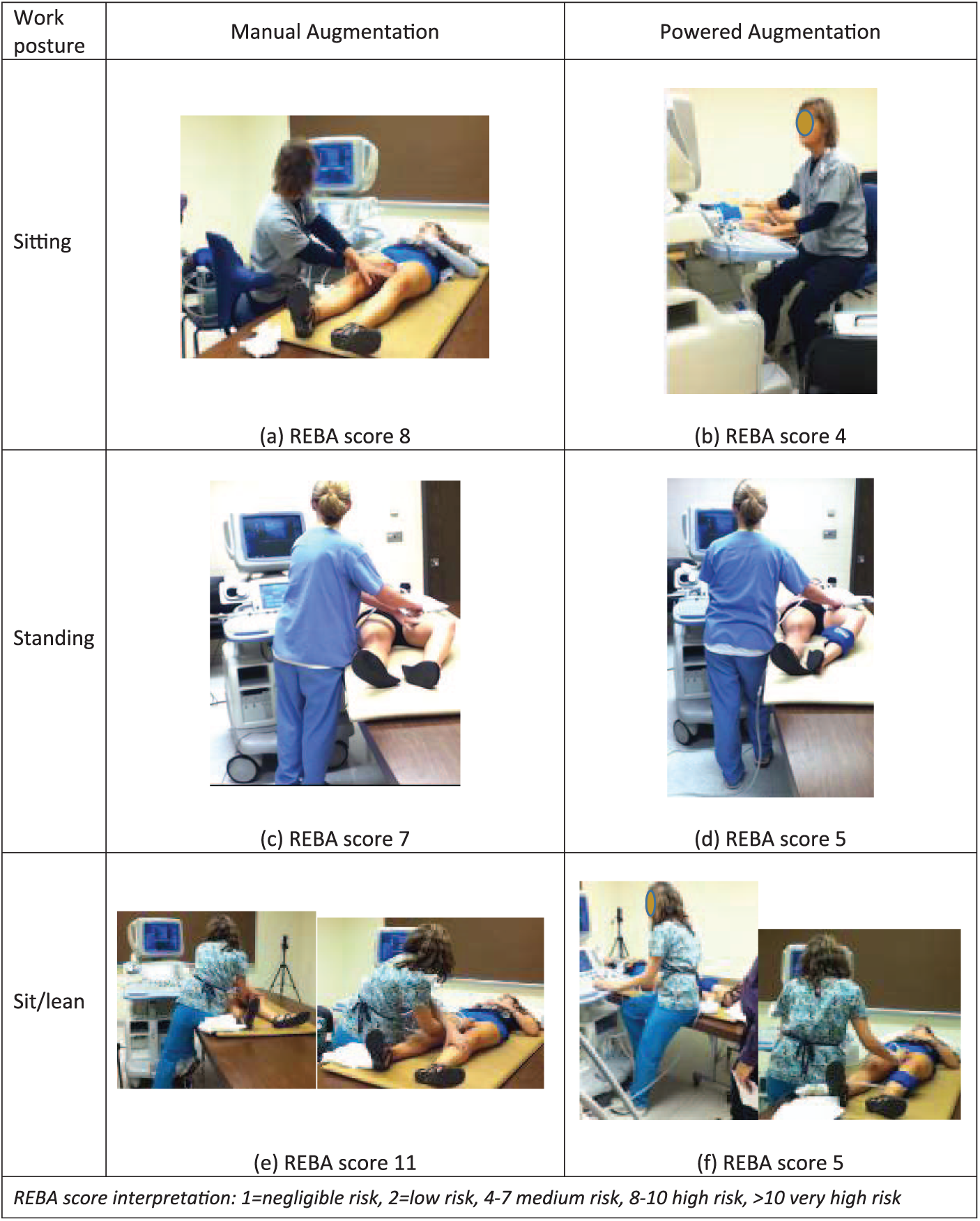
Comparison of work postures using manual (left) and powered augmentation (right).
The overall ratings of usability, usefulness, and desirability (on a scale of 1 = very poor to 7 = very good) were, respectively, 5, 5, and 4 for the E20 and 5, 6, and 5.5 for the VenaPulse. Overall, the research participants were positive about the concept of using an assistive augmentation device over standard manual augmentation (see Appendix for median scores for each of the UUD items for both devices). When comparing between the two augmentation systems, the results show that the VenaPulse inflation system was judged slightly better in term of usefulness and desirability compared to the E20 inflation system. This might be due to the fact that VenaPulse appeared to deflate more quickly than the E20. All participants rated the option to operate the VenaPulse with a hand or foot pedal control as an important feature of that device. Five of the seven participants rated the E20’s optional cycle timer that could inflate and deflate repeatedly for preset intervals as an important feature of that device. Most participants voiced concerns (barriers) about the portability of both devices, because both inflation systems are heavy, although the VenaPulse system is more compact than the E20. Both systems would be appropriate for clinic settings.
Conclusion
A primary goal of this study was to identify needs and opportunities for new approaches to reduce the exposure of diagnostic medical sonographers and vascular technologists to work-related risk factors that contribute to MSK symptoms and disorders. Another primary goal was to bring forth intervention concepts and perform usability tests of physical prototypes or existing potentially beneficial solutions that are currently underutilized. Both of these goals were accomplished, and this paper describes the results specifically for diagnostic medical sonographers and vascular technologists. Continued engagement of DMS and VT ensured that the interventions would address their specific needs and requirements. There are many remaining opportunities for development of engineering controls to reduce MSK risk factor exposure in sonographers. Through this study, we hope to encourage engineers and ergonomists to move beyond surveying sonographers about their problems and, instead, focus efforts on working with sonographers to create solutions to address their persistent problems and to continue in those intervention efforts through the entire Intervention Development Research process (Development, Implementation, and Effectiveness Research Phases). 18
Supplemental Material
JDMS-18-05-049-OR.R1_Appendix_Supplement_Online – Supplemental material for Collaborating With Sonographers and Vascular Technologists to Develop Ergonomics Interventions to Address Work-Related Musculoskeletal Disorders
Supplemental material, JDMS-18-05-049-OR.R1_Appendix_Supplement_Online for Collaborating With Sonographers and Vascular Technologists to Develop Ergonomics Interventions to Address Work-Related Musculoskeletal Disorders by Carolyn M. Sommerich, Kevin D. Evans, Steven A. Lavender, Elizabeth Sanders, Sharon Joines, Sabrina Lamar, Radin Zaid Radin Umar, Wei-Ting Yen and SangHyun Park in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
This work was supported by the National Institute for Occupational Safety and Health, under Grant R01 OH009253. We also sincerely appreciate the in-kind support provided by HoverTech International. We are grateful to all the imaging technologists who participated in this study and their managers who supported their engagement.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institute for Occupational Safety and Health, under Grant R01 OH009253.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.