
Abstract
Objective:
This study aimed to determine whether there was a difference in reported pain and perceived pain levels in different sonography specialties.
Materials and Methods:
An online survey was sent to 28 302 sonographers by the American Registry of Diagnostic Medical Sonography (ARDMS). Sonographers had to be registered and located within the United States to meet inclusion criteria.
Results:
There were 7993 sonographers who completed the questionnaire. The percentage of sonographers who reported scanning in pain across all specialties was 66.25%, with an average pain level of 4.0. The highest pain and injury levels were reported in the cardiac, vascular, and obstetrics/gynecology specialties. Sonographers scanning greater than 18 scans per day or greater than 30 minutes had the highest levels of perceived pain.
Conclusion:
According to these study results, reported pain in sonographers is decreasing. Certain specialties within sonography are more prone to injury and higher pain levels.
Sonographers face an increased risk of musculoskeletal disorders due to the physical demands of the profession. The first American publication describing the risk of occupational injury to the shoulders of sonographers was published in 1985. 1 The next decade of research showed increases in carpal tunnel syndrome, shoulder injuries, and other musculoskeletal injuries related to the physical demands of the profession.2,3 Pike et al 4 published the first staggering statistic that greater than 80% of sonographers scan in pain. Consequent research showed pain levels to be between 75% and 90%.5–8
The cost of work-related musculoskeletal disorders (WRMSDs) is high—20 billion in direct worker’s compensation costs and another estimated $100 billion in indirect costs such as lost revenue, training, and replacement. 9 Murphey and Coffin 10 have estimated the cost of lost revenue due to sonographer injury to be $40 000–$96 000 monthly. Muir et al 11 estimated the direct cost to employers for an injured sonographer to be over $120 000. Sound Ergonomics 10 reports that hiring replacement staff costs health care facilities $130 000–$166 000 per year, not including the $10 500 it costs to recruit and hire a new sonographer. With chargeable income in each sonography room of $22 000 per week, the cost of injury could cost health care facilities $1.17 billion per year in lost revenue. 10
Sonographers may choose to practice in a variety of technical specialties. These specialties may expose the sonographer to unknown risks of WRMSDs. In the obstetrics and gynecology (Ob/gyn) sonography specialty, 65.6% of respondents reported pain compared to 86% of cardiac sonographers.12,13 A study by Bagley et al 14 found that there was no statistical difference in specialties (general, cardiac, Ob/gyn, vascular) of those sonographers who reported pain. To date, no research was located on the difference in perceived pain levels among sonography specialties.
Work-related musculoskeletal injuries are prevalent across all specialties within the sonographer population, yet many sonographers are fearful of reporting their injuries to management. Sonographers historically felt that injury was part of their job. 15 A similar thought process still prevails today, with 57% of injured sonographers not reporting their injury to management. 14
Many reduction tactics have been recommended to reduce WRMSDs. However, the differences between specialties are significant, and thus the recommendations for each specialty may need to be different. The purpose of this research study was to answer the following research questions: (1) Is there a difference in pain levels in sonographers in different specialties? (2) Do certain specialties within sonography have higher injury rates?
Materials and Methods
This research was conducted using an online survey instrument (SurveyMonkey). After obtaining institutional review board approval, the American Registry of Diagnostic Medical Sonography (ARDMS) sent out an e-mail to sonographers located within the United States. Inclusion criteria included registered ARDMS sonographer in abdomen, Ob/gyn, vascular, or adult echocardiography and located in the United States. Approximately 28 302 sonographers met these criteria and therefore were sent the link to access the electronic survey. Once the link was opened, sonographers were then able to consent to the survey and complete the questionnaire. The survey remained open for 14 consecutive days. Once the 14 days were over, completed surveys were analyzed by the researcher.
Statistical Analysis
A power analysis was conducted to calculate the minimum sample size. For a total population of sonographers at 28 302, a confidence level of 95%, and a confidence interval of 5%, the minimum number of participants calculated was 382. Responses were downloaded and analyzed using Microsoft Excel and IBM SPSS Statistical software (version 26). Regression analysis and a Student’s t-test were used to analyze the data. A confidence interval of 95% and a threshold probability value of P ≤ 0.5 were established prior to indicate statistical significance.
Results
A total of 7993 participants met the inclusion criteria and fully completed the questionnaire. Of the respondents, 11% identified as the male gender (n = 882) and 89% as the female gender (n = 7054). Males reported their primary specialty as being cardiac, abdominal, and vascular compared to the females who selected Ob/gyn and abdominal specialties. A statistically significant number of male counterparts practiced in vascular and cardiac specialties compared to their female counterparts. A statistically significantly higher number of males reported that they did not scan in pain compared to females, 44% to 32.4% (P < .05). Of those reporting they scanned in pain, the average reported pain level was 3.51 compared to 4.32 in females. Males reported a statistically significant lower amount of pain in the shoulder, neck, and low back compared to female sonographers (P < .05) (Table 1)
Comparison of Participants by Gender.
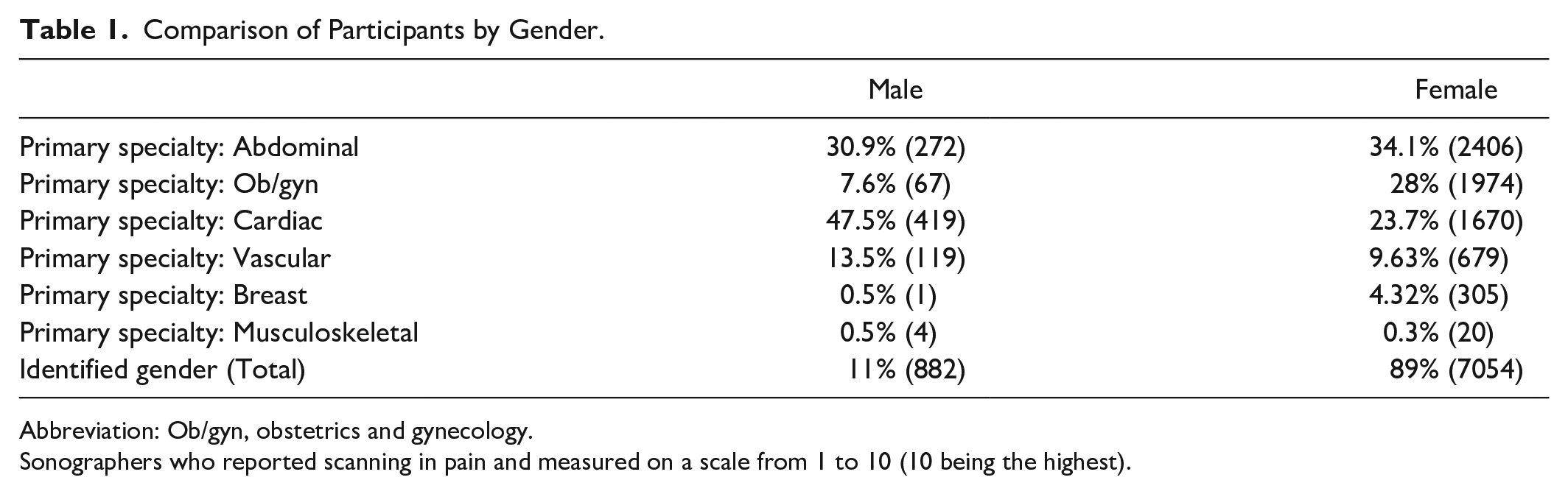
Abbreviation: Ob/gyn, obstetrics and gynecology.
Sonographers who reported scanning in pain and measured on a scale from 1 to 10 (10 being the highest).
The age ranges of sonographers included the following: 5% aged 20–29 years (n = 403), 21% aged 30–39 years (n = 1716), 25% aged 40–49 years (n = 2002), and 48% aged >50 years (n = 3861). Sonographers in the age groups of 30–39 and 40–49 years reported a statistically significant higher amount that scanned in pain compared to those sonographers above the age of 50 years (P < .05). There was no significant statistical difference in the level of pain between ages. Those aged above 50 years reported a statistically significant increase in sustaining a WRMSD (P < .05).
Data were assessed to determine differences between sonographic specialties (Table 2). The highest percentage of respondents reported primarily scanning abdominal examinations (33.72%, n = 2696), followed by cardiac (26.25%, n = 2098), ob/gyn (25.75%, n = 2058), vascular (10.11%, n = 808), breast (3.84%, n = 307), and musculoskeletal (0.33%, n = 26). The specialties were assessed to determine any significant statistical differences between the groups. Ob/gyn, cardiac, and vascular specialties all reported a higher number of sonographers scanning in pain, a statistically significant finding compared to abdominal or breast sonographers (P < .05). The highest levels of reported pain were in the ob/gyn and vascular specializations at 4.46 and 4.30, respectively. Musculoskeletal and breast specialties had the lowest reported levels of perceived pain at 3.54 and 3.99. All specializations reported a statistically significant increase in the number of work-related musculoskeletal injuries compared to breast sonographers (P < .05). Ob/gyn, cardiac, and vascular sonographers all reported the highest number of work-related injuries (Figure 1).
Reported Pain by Primary Specialty.
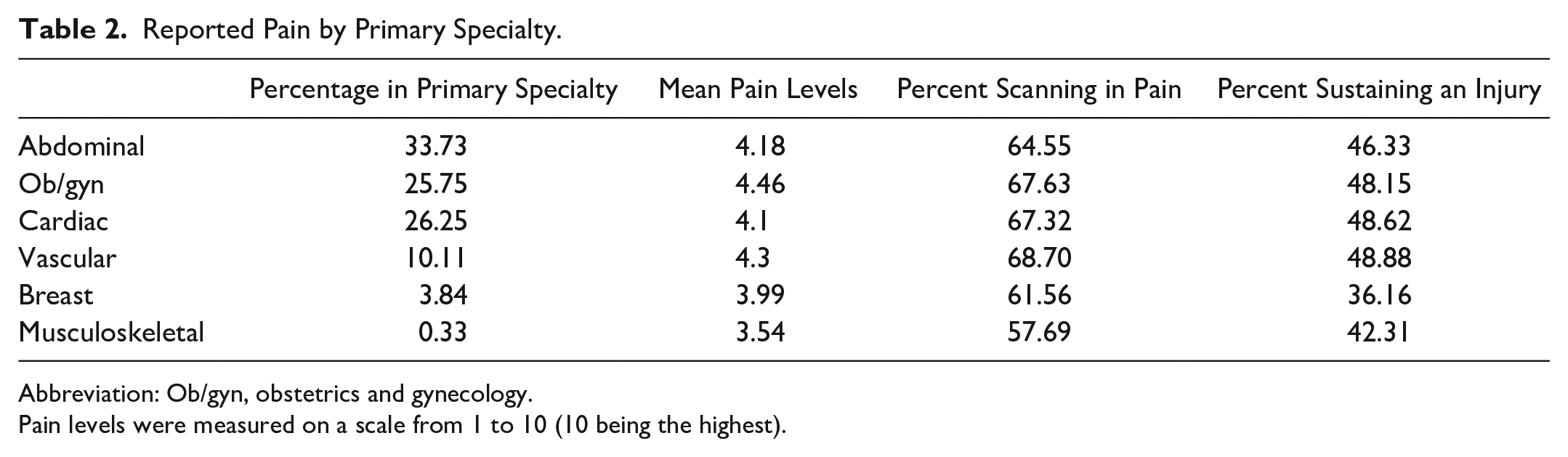
Abbreviation: Ob/gyn, obstetrics and gynecology.
Pain levels were measured on a scale from 1 to 10 (10 being the highest).
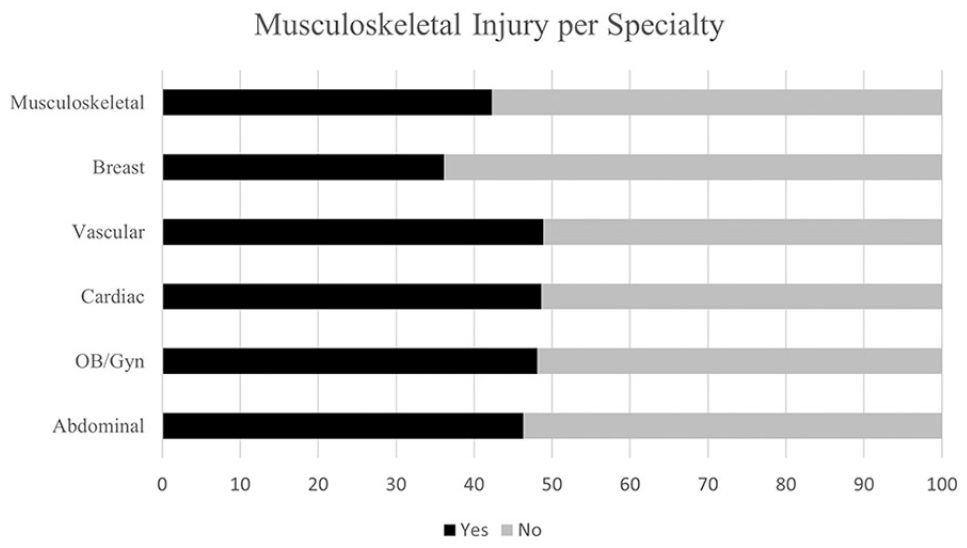
Responses by specialty to “During your career, have you ever sustained a work-realted musculoskeletal injury?“ (n=7980).
Locations of pain according to primary sonographic specialty were also evaluated (Table 3). A statistically higher percentage of ob/gyn sonographers reported pain in the hand and wrist compared to all other specialties at 51.46%. In addition, ob/gyn sonographers reported a significantly lower amount of low back pain (28.48%) compared to all other specialties. Differences in pain for the shoulder and neck were not significant across specialties.
Location(s) of Reported Pain by Primary Specialty.
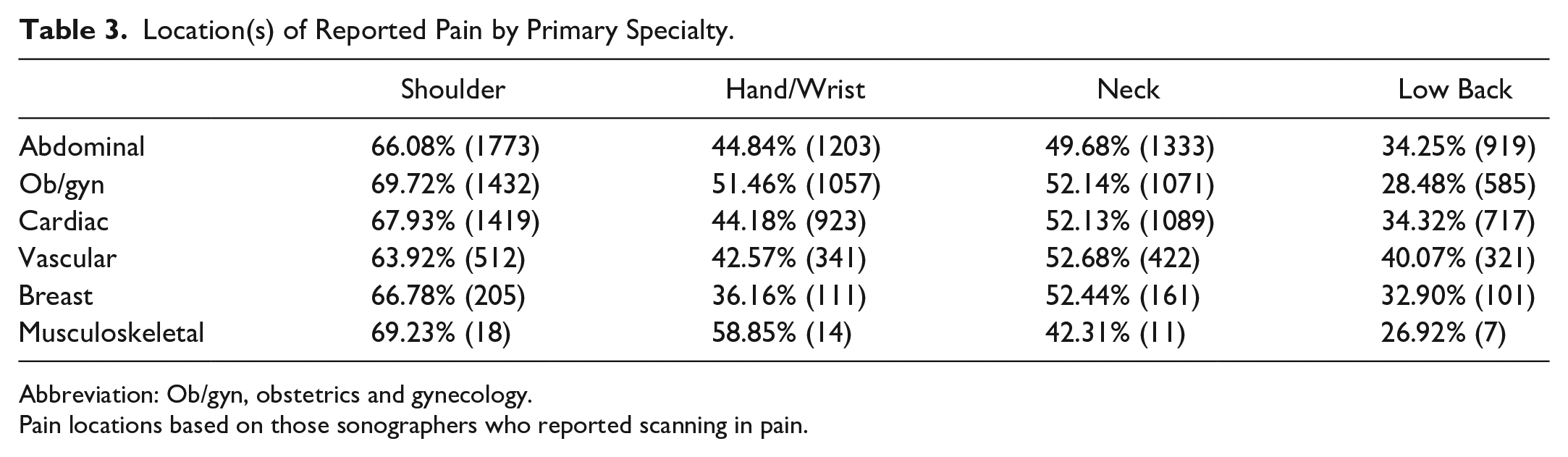
Abbreviation: Ob/gyn, obstetrics and gynecology.
Pain locations based on those sonographers who reported scanning in pain.
Data were analyzed using a multiple linear regression model to determine whether age, years of experience, number of scans (examinations), average length of the scans (examinations), and sonography primary specialty were predictors of pain. All the dependent variables were statistically significant except sonographic specialty. Age, years of experience, number of scans (examinations), and the average length of the scans (examinations) can all predict whether a sonographer will be scanning in pain. However, the sonographic specialty cannot predict whether a sonographer will be scanning in pain.
Perceived pain levels, average time per scan, and average scans (examinations) per shift were analyzed to determine any statistical significance between the variables. The highest percentage of sonographers reported scanning between 25 and 30 minutes per examination (28.49%), followed by those scanning more than 30 minutes (24.22%), scanning 15–20 minutes (19.54%), 10–15 minutes (6.26%), and <10 minutes (0.67%). The average scans per shift were reported as 6–8 (34.55%), 9–11 (33.86%), 12–14 (17.9%), 15–18 (6.03%), 1–5 (5.66%), and >18 (2.0%). Cardiac sonographers reported a statistically significant longer amount of time spent scanning compared to all specialties and lower number of scans completed per shift (6–8 scans). The ob/gyn sonographers similarly reported a statistically significant longer amount of time spent scanning compared to all specialties except cardiac, but a higher number of scans completed per shift (>9 scans) compared to vascular and cardiac specialties (P < .05). Finally, perceived pain was reported highest is sonographers scanning greater than 18 scans per day at a pain level of 5.03 and highest in those who reported scan times greater than 30 minutes (Figure 2).
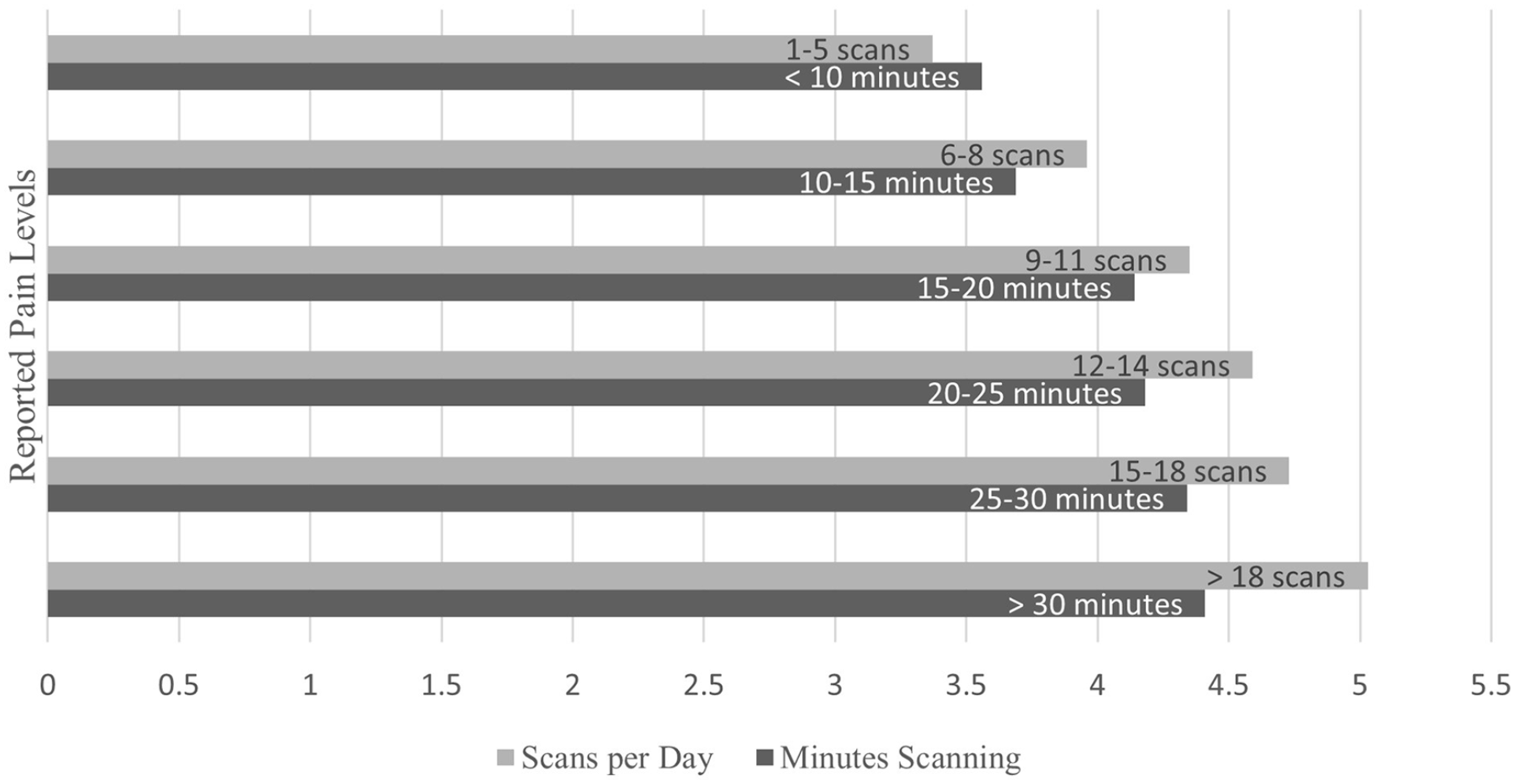
Pain levels by number and length of scans. Pain levels were measured on a scale from 1 to 10 (10 being the highest). Ob/gyn, obstetrics and gynecology.
Discussion
The results of the study suggest that there are certain specialty examinations within sonography that are more painful to complete. Those vascular, cardiac, and ob/gyn sonographers responding had greater reporting of scanning in pain (68.7%, 67.2%, and 67.32% respectively). The findings were similar to Bagley et al 14 that 66.67% of ob/gyn sonographers surveyed reported scanning in pain. Vascular and cardiac sonographers reported a higher number who scanned in pain compared to previous research. 14 Wang et al 19 have described the increased risk of pain in the ob/gyn specialty due to the extended times needed to complete a detailed obstetric sonogram. Distractions are also common in the obstetric specialty due to the nature of the examination that allows for extra observers, children, electronic devices, and the social bonding component of the ultrasound experience. 16 These distractions may lead to longer examination times and thus increase perceived pain levels.
Research has shown the number of sonographers scanning in pain to be between 75% and 90%,6–8 although a small-scale study demonstrated a reduction in reported pain at 53% compared to the previous research. 14 The number of sonographers who reported scanning in pain across all specialties was 66.25%, with an average pain level of 4.0. There have been multiple efforts in the sonography community to reduce musculoskeletal injury and pain, including ergonomic techniques, physical activity, and stretching programs.17,18 The results of this research could demonstrate that ergonomic awareness, intervention, and reporting have improved sonographers’ reported pain.
The number of sonographers who reported scanning pain is much lower than the expected 90% previously documented. 19 Sixty-six percent of sonographers across all specialties reported scanning in pain. A possible explanation for this large difference could be the sample population that was surveyed. The sample population in previous research studies was obtained by surveying a society of sonographers requiring a paid membership. The ARDMS assisted in sending out this survey to all registered sonographers. The difference in the sampled population could explain the reported pain difference, in addition to the increasing awareness and interventions sonographers are utilizing. The Industry Standards for the Prevention of Work Related Musculoskeletal Disorders in Sonography released by the Society of Diagnostic Medical Sonography (SDMS) could also be responsible for this reduction in reported pain by providing employers, manufacturers, sonographers, health care organizations, and educational programs factors that they can address. 20 Although this research hat less sonographers are scanning in pain is promising, there is still 66% of sonographers who did report scanning in pain. Sonographers should continue to advocate for their safety and make ergonomic adjustments with each patient to reduce their own personal risk of injury.
Perceived pain levels have not been well researched prior to this study. All respondents were asked to rate their pain level on a scale from 1 to 10: 1 representing no pain and 10 representing pain that is constant and debilitating inside and outside of work. The data concluded that perceived pain levels in vascular and ob/gyn specialties were higher than in other specialties. Ob/gyn sonographers reported pain levels at 4.46, while vascular sonographers reported their pain levels at an average of 4.30. In all, 2.2% of vascular and ob/gyn sonographers reported their pain level to be 10. Perceived pain levels were highest among sonographers who scanned greater than 30 minutes per scan and those who reported the highest number of examinations per day. Previous research has shown that risk factors to develop WRMSD included performing greater than 100 scans per month, longer scan times (exceeding 25 minutes), female sex, and a prolonged strong handgrip. 3 These risk factors are prevalent within ob/gyn and vascular examinations. To the author’s best knowledge, no research has been conducted to best reduce WRMSD by sonographic specialty. Different muscle groups, positioning, and ergonomic techniques are needed depending on the type of examination being performed. Ob/gyn and vascular sonographers reported the most worrisome data and therefore should be focused on specifically to help reduce pain and WRMSDs within their respective specialties.
Previous research has shown the most common location(s) of reported pain to be in the shoulder, hand/wrist, neck, and low back.19,14,21 Hand and wrist pain within the ob/gyn specialty was a particularly alarming finding in this study. Ob/gyn sonographers reported the highest percentage of pain to be located within the wrist and hand when compared with other specialties. Wang et al 19 identified unique risks that obstetric sonographers face, including the complex, time-consuming nature of an obstetric sonogram and the larger, heavier 3D probe. Similar to previously mentioned findings, ob/gyn sonographers must optimize their work environment specifically for the unique nature of their examinations.
Reporting Injuries to Management
Although sonographers frequently reported work-related injuries, many did not report these injuries to management. Bagley et al 14 demonstrated the disconnect between administration and sonographers, where sonographers felt they were unable to report injuries and pain levels to superiors. Many sonographers testified they did not report any injury to management. 14 Zhang et al 21 found that 31% of injured sonographers were absent from work. This research study found that 49.6% of sonographers who were injured never reported their injury to management. This suggests that sonographers are scanning in pain, adding to their injuries, and not getting the compensation and help that they need.
Limitations
The quantitative nature of this survey instrument provided a limited nature of feedback. Participants were asked to self-rate pain on a 10-point scale. Not every participant would quantify their pain the same. The survey instrument did not ask questions about hours per shift or allow sonographers to pick more than one primary specialty.
Future research is needed to determine what has attributed to the decrease in pain and the cause of increased pain and injury in ob/gyn, vascular, and cardiac sonographic clinics. Specialty-specific research is needed to determine which interventions and ergonomic training are most effective in each respective specialty. More research is also needed on injury reporting and whether injuries in public or private sector health care systems are more or less likely to be reported.
Conclusion
This research study has shown a decrease in the number of sonographers who are scanning in pain and allowed sonographers across multiple specialties the ability to assign their pain a numerical level. Although a decrease, 66% of sonographers are still reporting that they scan in pain. The trend must continue to decrease pain and injury rates within the profession and improve overall ergonomics to keep decreasing the number of sonographers scanning in pain.
Sonographers who practice primarily in vascular, cardiac, and ob/gyn specialties reported the most significant pain levels and injury rates. Sonographers who are scanning more examinations a day and for longer periods of time also reported the highest pain levels. Given the unique nature of ob/gyn, vascular, and cardiac sonography examinations, consideration should be given to how to reduce injuries in each respective specialty. Much work has been done by the sonography community to reduce pain and injury rates, but more attention is needed to address specialty-specific ergonomic needs and interventions.
Footnotes
Ethics Approval
Ethical approval for this study was obtained from California Intercontinental University IRB approval number 40920200001.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because this study is on humans.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.