
Abstract
The objective of this study was to investigate the prevalence and clinical implications of the hyperechoic rim of liver focal solid lesions. A retrospective review was conducted of sonograms of focal liver lesions with a hyperechoic rim, as well as relative examinations such as computed tomography, magnetic resonance imaging, biopsy, resection, and histopathology reports. A cohort of 10 232 patients was found to have solid focal liver lesions (2030 malignant, 8202 benign). A hyperechoic rim was determined in 182 hemangiomas, 2 granulomas, 2 hepatocellular carcinomas (HCCs), and 4 other malignancies. There were significant differences between malignant and benign lesions (P < .001), between HCCs and hemangiomas (P < .001), between malignancies and hemangiomas (P < .001), between HCCs and granulomas (P = .044), and between other malignancies and granulomas (P = .005). There was no significant difference between liver granulomas and hemangiomas (P = .656). In this study, a hyperechoic rim in solid focal liver lesions appeared mainly in hemangiomas, granulomas, and rarely in malignant lesions.
Sonography has been globally used for the assessment of the liver, and because of these imaging evaluations, focal liver lesions have been incidentally discovered. The initial identification of a focal liver lesion is usually based on its sonographic characteristics. Typically, the rim at the periphery of focal liver lesions can present as isoechoic, hypoechoic, marked hypoechoic, and/or hyperechoic. The hyperechoic rim of a focal liver lesion has a higher echogenicity than both the internal architecture and the liver parenchyma. Previous reports have indicated that a hyperechoic rim can be noted in a liver hemangioma, regenerative cirrhosis nodule, and hepatocellular carcinoma (HCC).1–6 However, clinically, it rarely presents with other focal liver lesions, except hepatic cavernous hemangioma. Unfortunately, the distribution of a sonographic hyperechoic rim associated with a focal liver lesion remains unaddressed in the literature. It may be diagnostically helpful to deliberately analyze the sonographic appearance of a hyperechoic rim when assessing solid focal liver lesions and may also help to narrow further investigation. The objective of this study was to investigate the prevalence as well as the implications of a sonographic hyperechoic rim appearance in association with solid focal liver lesions.
Materials and Methods
Study Population
An audit of the archived medical record of patients referred for an inpatient liver sonogram was performed between January 2011 and March 2018. The patients’ data and sonographic images were obtained from the Hospital Information Systems and Picture Archiving and Communication Systems (PACS). Two sonologists, who were not responsible for interpretation of the images, collected the cases for review. If a patient received several liver sonograms, the patient was still counted as one case. The inclusion criteria included patients who underwent a liver sonogram, presence of focal lesions in the liver, and a hyperechoic rim appearance of the lesions. The exclusion criteria were patients who demonstrated cystic focal liver lesions, lesions that did not demonstrate a rim, lesions that had blurring and an ambiguous thin rim, and lesions with a hypoechoic rim. Relative study reports for computed tomography (CT), magnetic resonance imaging (MRI), biopsy, resection, and histopathology were reviewed for solid lesions with a hyperechoic rim. The images were evaluated for imaging characteristics and pathology by 1 radiologist and 2 sonologists as a panel, who had access to previous diagnoses.
Sonographic Examination
The sonographic examination was performed by 12 sonologists who had 4 to 23 years of experience. Logiq 9 (GE Healthcare, Waukesha, WI, USA), Voluson expert 730 (GE Healthcare, Piscataway, NJ, USA), HD11XE (Philips Medical Systems, Dalian, China), Sonos 5500 (Philips Medical Systems, Eindhoven, the Netherlands), Aloka ProSound α 10 (Hitachi Aloka Medical Ltd, Tokyo, Japan), Siemens Acuson S 2000 ( Siemens Medical Solutions USA, Inc, Malvern, PA, USA), and Mindray DC-8 (Mindray Medical International Limited, Senzheng, China) ultrasound systems were used, with a convex transducer with a frequency of 2 to 5 MHz. The preset was adjusted to abdominal mode, the gain of gray-scale was adjusted from 35 to 70, the time-gain-compensation was moved to the left side of the midline, and the focal zone was adjusted to the level of interest region, enabling clear display of the detecting area. The color Doppler gain was adjusted from 30 to 70, depending on the vessels detected without causing aliasing. In certain situations, harmonic imaging and the zoom feature were employed to improve sonographic quality and eliminate artifacts. The zoom feature was used to scrutinize the rims of the focal lesions for ambiguous liver lesions.
The liver was investigated carefully with duplex color Doppler, and representative images of abnormal findings were saved to the PACS. Some inclusive focal nodular entities were further evaluated using CT, MRI, and biopsy. These added diagnostics were performed for undetermined lesions as well as for diagnostically complex lesions suspicious of malignancy.
CT and MRI Examinations
A 64-multiple-detector CT scanner (LightSpeed VCT, GE Healthcare) was used for the evaluation of undetermined and/or diagnostically complex cases. A multiphase (unenhanced and/or arterial, portal venous, and delayed equilibrium phase) CT was also performed. A 1.5-T GE Signa Horizon LX, EchoSpeed MRI scanner (GE Medical Systems, Milwaukee, WI, USA) with a phased-array torso coil was used for undetermined and diagnostically complex liver lesions. The standard protocol was T2-weighted images with variable echo time, dual-echo in and out phase spoiled gradient-echo T1-weighted images, and dynamic 2D fast spoiled gradient-echo images at unenhanced, arterial, portal venous, late portal venous, and delayed phases.
Image Interpretation
The images were interpreted by 2 professionals with 4 to 26 years of imaging experience who agreed on a diagnosis or a diagnostic description. The interpretation was based on categorizing the pathology and describing the lesion as malignant, probable malignant, probable benign, or benign. In the process, if a lesion met a certain imaging criterion, a diagnosis was established; if a lesion did not meet a criterion completely, comprehensive study through combining other imaging characteristics, follow-up findings, and serum alpha fetal protein level was adopted. The criterion for an imaging diagnosis of HCC was that the nodule, in a cirrhotic liver (or normal liver background), was demonstrated to be hypervascular with washout in the portal venous phase on contrast-enhanced CT/MRI or sonogram. 7
On CT imaging, a typical liver hemangioma meets the criterion of a circumscribed hypodense lesion; on contrast-enhanced CT, the lesion presents with nodular or annular centripedal enhancement in the arterial phase, and the center part shows persistent enhancement in the portal venous and late phase. 8 The MRI diagnostic criterion for hemangioma includes early peripheral nodular enhancement, centripetal filling, and hyperintense complete fill-in in the equilibrium phase, as well as high signal intensity on T2-weighted images “bright dot” or minimal peripheral enhancement in the equilibrium phase. 9 On sonography, liver hemangiomas usually have characteristics that are nodular or mass lesions in the liver that are round, ovoid, or lobulated shaped; with hyperechoic, hypoechoic, isoechoic, and complex echoic appearance; homogeneous or heterogeneous internal architecture; circumscribed or rough rim; and with or without posterior acoustic enhancement. 10 Other descriptions, such as shape, size, thickness, thin, spicular, fuzzy, smooth, and so forth, were also documented according to the appearance of the lesions. The same metrics were applied when reviewing other liver lesions.
An institutional review board approved this retrospective study, and neither patient approval nor informed consent was required for the image review of sonography, CT, MRI, or any additional medical records. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statistical Analysis
The quantitative data were expressed as mean values ± standard deviations (mean ± SD), and percentages were used for prevalence. χ2 test (Fisher exact test) was used to evaluate the difference between liver malignancies and hemangiomas or granulomas in the prevalence of hyperechoic rim. The level of statistical significance was set at P < .05. Statistical analysis was performed using SPSS version 20 (IBM Corporation, Armonk, NY, USA).
Results
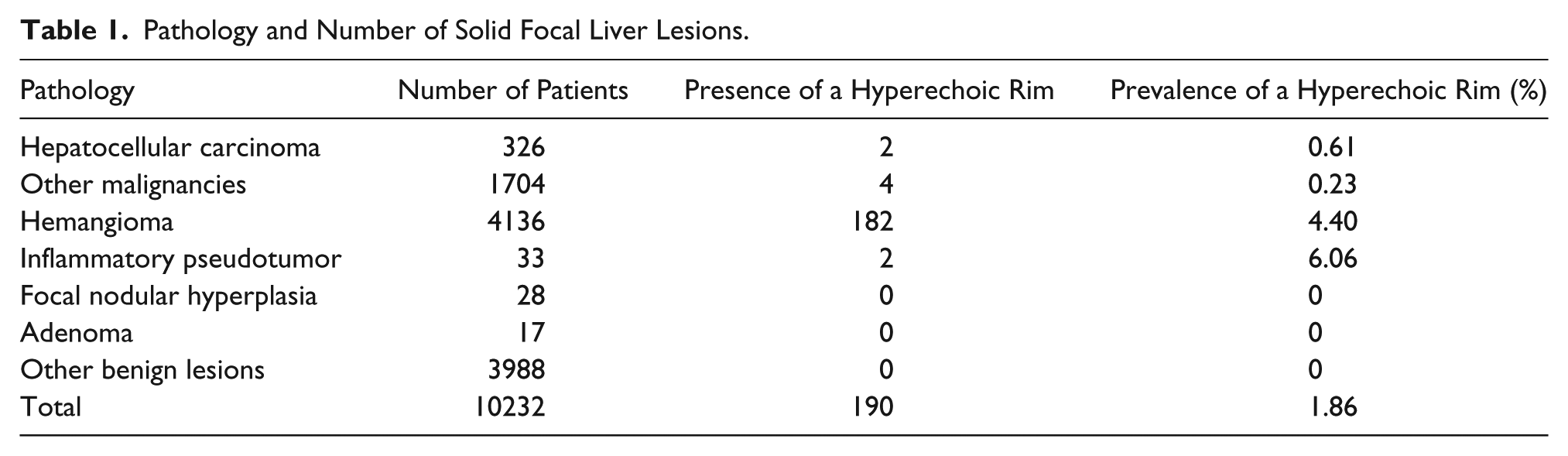
In this retrospective study, 10 232 patients were found with solid focal liver lesions, which included hemangiomas, HCC, metastatic tumors, granulomas (inflammatory pseudotumor), regenerative nodules, focal nodular hyperplasia, adenomas, focal infection, hematomas, as well as other benign and malignant lesions. Of all the patients, 2030 (1147 men, 883 women) had solid focal liver lesions that were malignant. The mean age of these patients was 62.3 years, with a range of 26 to 98 years. The remainder of the cohort, 8202 patients (4814 men, 3388 women) had benign liver lesions. The mean age of these patients was 40.8 years, with a range of 18 to 91 years. The appearance of a hyperechoic rim on the solid focal liver lesions was noted in 182 hemangiomas, 2 granulomas, 2 HCCs, and 4 other malignancies. The prevalence of hyperechoic rim around hemangiomas, granulomas, and other malignant lesions (HCC and other malignancies) was 4.4%, 6.06%, and 0.29%, respectively. The pathology and number of solid focal liver lesions are summarized in Table 1. There were significant differences between malignant lesions (HCC and other malignancies) and benign lesions (P < .001), between HCC and hemangiomas (P < .001), between malignant lesions and hemangiomas (P < .001), between HCC and inflammatory pseudotumors (P = .044), and between other malignant lesions and inflammatory pseudotumors (P = .005). There was no significant difference between inflammatory pseudotumors and hemangiomas (P = .656). A subset of 2513 patients had hepatitis virus B– or C–related chronic hepatic disease and liver focal lesions; however, there was no hyperechoic rim associated with these lesions. The hyperechoic rim in the granuloma lesions was usually round, smooth, or rough, and in the hemangioma, it was ovoid, round, slightly irregular, fuzzy, or specular. The sonographic appearance of HCC and other malignant lesions was round, regular, and smooth. Figures 1 to 3 illustrate some of the solid focal liver lesions with an associated hyperechoic rim.
Pathology and Number of Solid Focal Liver Lesions.
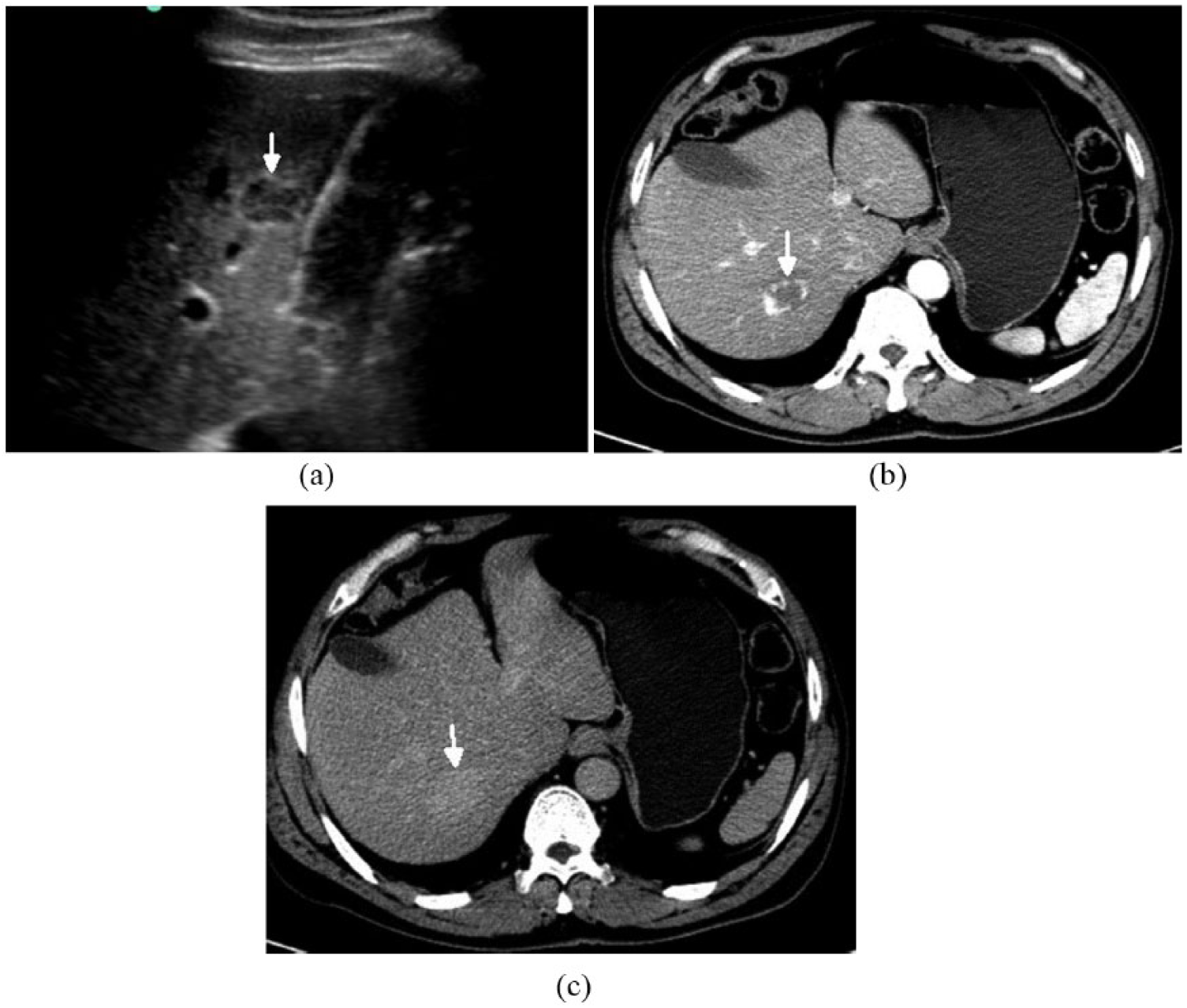
A 55-year-old man with a nodular lesion in the SVII portion of the liver. (a) On sonography, the oval-like lesion, 2.5 cm in longitudinal diameter, presented as a complex echogenicity, with hyperechoic irregular rough rim (arrow) and heterogeneous hypoechoic content. These sonographic characteristics are suggestive of a hemangioma. (b) A 55-year-old man with a nodular lesion in the SVII portion of the liver. The image obtained with contrast-enhanced computed tomography (CT) shows that the lesion presented with centripetal tiny nodular enhancement around the rim (arrow) during the arterial phase. (c) The image obtained with contrast-enhanced CT demonstrated a lesion that gradually presented with a full homogeneous enhancement, at portal venous and late phase (arrow), and the enhancement approached the parenchyma. The characteristics of contrast-enhanced CT are suggestive of a hemangioma.
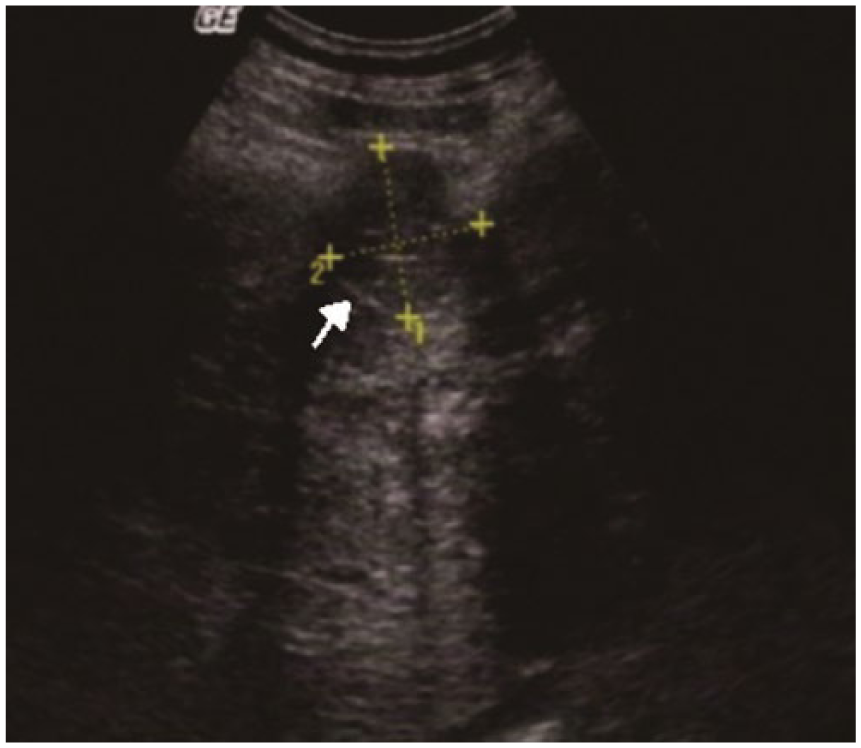
A 67-year-old man with a mass in the SVIII portion of the liver. On sonography, the round-like lesion, 8.7 cm in longitudinal diameter, presented with slight hypoechogenicity and anechoic center, with a hyperechoic smooth thin rim (arrow). On contrast-enhanced computed tomography (CT), the lesion presented classical characteristics of hepatocellular carcinoma.
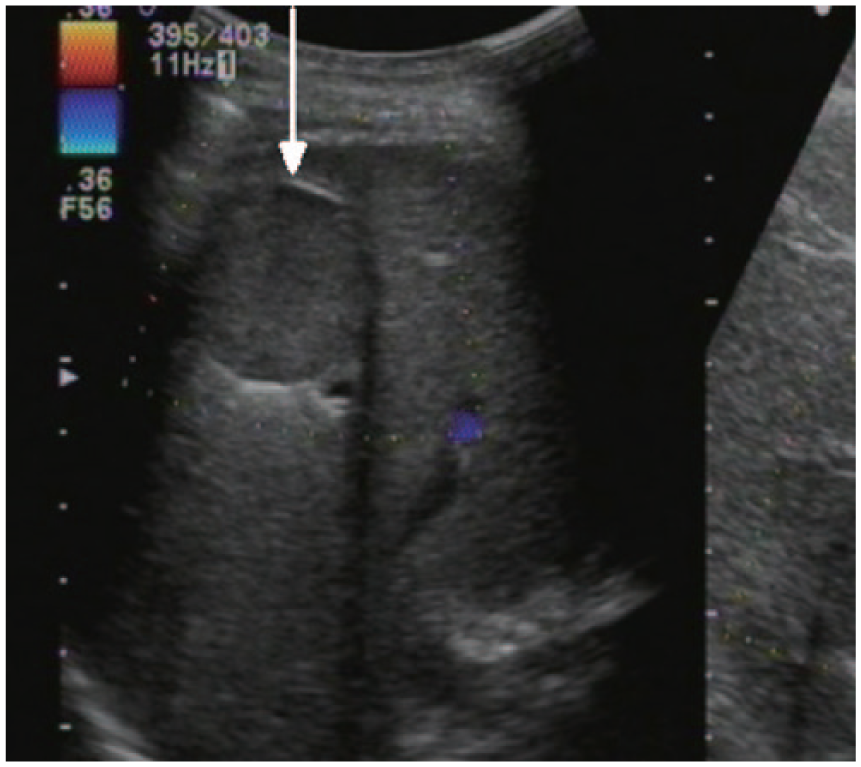
A 38-year-old man with a nodular lesion in the SV portion of the liver. On sonography, the round lesion, 2.9 cm in diameter, had a hyperechoic margin (arrow) and homogeneous slight hypoechoic content. On color Doppler imaging, there was no blood vessel detected within the lesion. The sonographic characteristics are suggestive of a benign lesion. Clinical data and computed tomography images indicated a pseudotumor (granuloma).
Discussion
The rim of a focal liver lesion has been regarded as an important characteristic to differentiate HCC compared with a hypoechoic halo around a benign lesion; however, some benign lesions have been noted with either appearance (ie, hepatic hemangioma).11–14 A hyperechoic rim has not been uniquely described as a diagnostic sign for the identification and differentiation of liver focal lesions. It is interesting to note that Kraus et al. 4 stated that a hyperechoic rim might be a potential sign for characterizing a cirrhotic nodule. A hyperechoic rim is located in the peripheral region of a solid focal liver lesion. It may also be found at the margin, the capsule or pseudocapsule, and the compression marking of a tumor. The hyperechoic band along the margin of an HCC was reported by Wakui et al. 5 The compression marking presents between a tumor, can abut the parenchyma, and is very thin, although it does not belong to the tumor. Kraus et al. 4 reported that the hyperechoic rim presented in a regenerative nodule; however, this was not noted in the present cohort. In this study cohort, 2513 chronic hepatic patients were included, and thousands of focal lesions were noted as well as a fairly large number of regenerative and dysplastic nodules. Findings of hyperechoic rim in the current study may suggest that this appearance could be used to separate benign lesions (granuloma and hemangioma) from malignant lesions, narrow the differential diagnosis, and reduce additional diagnostic interrogation. A hemangioma is a commonly encountered lesion of the liver. 15 This study did demonstrate that a hyperechoic rim at the periphery of a malignant liver lesion was rare, and it was common in hemangiomas. This may suggest that the characteristic of a hyperechoic rim could be informative in the differentiation of hemangiomas from malignant lesions.
Some authors reported that a hyperechoic rim rarely presents with a hemangioma and that a hyperechoic rim is an atypical appearance for a hemangioma.1,2 Nevertheless, Ito et al. 6 reported that hemangioma with hyperechoic rim was very common, and in that study, a hyperechoic rim accounted for 64.9% of the cases. In the present study, the appearance of a hyperechoic rim accounted for 4.40%. It may be that the discrepancy in the prevalence of a hyperechoic rim appearance across different studies may be due to different patient samples. In this study, the hyperechoic rim appearance with a hemangioma was usually rough and fuzzy in appearance, and in malignant lesions, it was usually smooth sonographically. A hyperechoic rim appearance presented mainly in hemangiomas and inflammatory lesions and rarely presented in HCC or other malignant lesions in this cohort. This cohort result may suggest that a hyperechoic rim, together with other characteristics, may be useful in narrowing the differential diagnosis. This may be especially true for irregularly shaped lesions with a rough hyperechoic rim, which is highly suggestive of a hemangioma. This study demonstrated that a hyperechoic rim was not found in other benign focal lesions, except with either a hemangioma or granuloma. This might suggest that this sonographic appearance could be used to differentiate hemangioma and granuloma from other benign focal lesions.
Inflammatory pseudotumor (granuloma) of the liver is rare, but it is difficult to distinguish sonographically from a malignant tumor.16–18 In this condition, if the hyperechoic rim is present and the sonologist detects that a hyperechoic rim is one of the characteristics of the granuloma, it will be helpful in characterizing the lesion.
Limitations
The first limitation of this cohort study was that it employed a retrospective study design that relied on only those delicate features of the lesions that were imaged, therefore potentially compromising the robustness of the study. In addition, there were no histopathological studies on the nature of the hyperechoic rim, and the development mechanism of this appearance has not been clarified.
Conclusion
A hyperechoic rim may present with a dominant appearance sonographically in benign focal liver lesions, including hemangiomas and granulomas. This appearance may be very rare in HCC and other liver malignancies. The findings of this study suggest that if a solid focal liver lesion has a hyperechoic rim, a hemangioma or inflammatory pseudotumor may be considered. The diagnostic awareness of this sonographic appearance may be helpful in daily practice and increase confidence in the sonographic interpretation of these lesions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.