
Abstract
The objective was to establish normal thyroid volume in healthy infants and children, in a select Nigerian population. Using a portable ultrasound equipment with a 7.5-MHz transducer, 500 apparently healthy pediatric patients were sonographically evaluated. The volume for each thyroid lobe was obtained, as well as the summation of both left and right thyroid volumes, which represented the total volume. The mean and median thyroid volumes for the subgroups were 0.69 ± 0.38 cm3/0.7 cm3 (<1 year), 1.50 ± 0.68 cm3/1.4 cm3 (1–5 years), 2.75 ± 0.94 cm3/2.6 cm3 (6–10 years), 4.47 ± 2.83 cm3/3.7 cm3 (11–15 years), and 7.47 ± 4.81 cm3/5.9 cm3 (16 and 17 years). There was a significant difference (P = .000) between the population studied and the World Health Organization/International Council for Control of Iodine Deficiency Disorders reference values. The baseline values derived for thyroid dimensions may form the basis for thyroid screening in these asymptomatic children.
Although inspection and palpation are traditionally used to classify a goiter, the sensitivity and specificity have been rated poorly. This technique has been shown to be imprecise, with relatively high interobserver variation, when evaluating a low to moderate goiter.1–3
Evaluation of thyroid volume using sonography was reported to be accurate and precise. 4 It is noninvasive, rapid, inexpensive, and without discomfort to the patient and the examiner. It presents a prompt and cost-efficient means of assessing the thyroid gland for the purposes of monitoring the progress of a clinical condition and treatment outcome.5,6
The use of portable ultrasound equipment has made the use of sonographic evaluations very feasible, even in remote areas. 7 An ultrasound transducer frequency of 6.5 to 10 MHz is desirable for detailed sonographic textural evaluation and volume assessment of the thyroid gland.4,7,8 A previous study among a Nigerian population used 3.5-MHz transducers with a stand-off pad and therefore have image quality limitations. 9
Background
The World Health Organization (WHO) 10 has reported normal thyroid volume among European children to range from 5.4 to 16 mL (males) and 5.0 to 16.1 mL (females) for children aged 6 to 15 years. 10 However, previous researchers had expressed concern on the limitation of using the WHO recommended reference values and suggested the use of local reference values in the screening of children to exclude thyroid enlargement. 11
Nigeria is rated sufficient in the WHO/UNICEF/International Council for Control of Iodine Deficiency Disorders (ICCIDD) distribution of iodine deficiency disorder (IDD) areas in Africa. 12 This favorable ranking is because the National Agency for Food and Drug Administration and Control (NAFDAC) has greatly promoted salt iodization using a public campaign. In addition, the influx of Western diets into the country has exposed lots of families to consumption of a high level of iodized salt and iodine-containing food. 13
Some studies in Nigeria had assessed the thyroid volume in healthy adult populations,5,9 as well as school-age children.8,14 However there is paucity of studies that assessed thyroid volumes among preschool-age children, which was the purpose for executing this study. The values obtained from this study provide data that are more comprehensive for screening infants, children, and teenagers for thyroid enlargement.
Materials and Methods
In a cross-sectional prospective survey study and using a multistage sampling method, 500 infants and children within an age range of 3 months to 17 years were selected from some crèche, nursery, primary, and secondary schools within the Akwa-Ibom state in Nigeria. The purpose and procedure for the investigation were explained to the parents and teachers. Informed consent was obtained directly from the parents of the participating children through the parent-teacher association of the schools. Ethical approval was obtained from Ethical Committee of University of Uyo Teaching Hospital and written permission obtained from the relevant educational agencies.
A pediatrician screened the subjects to exclude medical conditions that would affect the results. The sonographic scanning protocol was developed and checked by a sonographer and a radiologist to establish the measurement technique and address the interobserver variability. The height and weight of the subjects were obtained to the nearest 0.1 cm and 0.1 kg, respectively. Body surface area (BSA) (m2) was calculated with the following formula 15 : BSA = √[height (cm) × weight (kg)/3600].
The selected infants and children were scanned within a period of 11 months. A parent, child minder, or a school teacher was allowed to serve as chaperon during the scanning process. No prior subject preparation was required. A single expert examiner performed thyroid volume measurement using a portable Kaimax 2200G ultrasound machine with a 7.5-MHz transducer (manufactured in China in 2011).
The subjects were examined in a supine position with a pillow placed under their shoulders to hyperextend the neck. Neonates were held and maintained in the above position by an adult. Acoustic gel was applied over the thyroid area. Transducer was placed directly on the skin over the thyroid gland. 5 On a longitudinal image, the maximum craniocaudal and anteroposterior diameters represented length (L) and depth (D) or thickness, while the maximum mediolateral diameter from a transverse image represented width (W). 16 The volume for each thyroid lobe was obtained using the following formula 15 : L × D × W × 0.479. The volume of the right and left lobes was summed manually to obtain the total thyroid volume (Tvol). 17
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 16 (SPSS, Inc., an IBM Company, Chicago, IL). Descriptive statistics used include median, range, mean, and standard deviation (SD). Inferential statistics used include Student t test to test the difference in mean and median values. A Pearson correlation coefficient was used to show relationships between the Tvol and age, height, weight, and BSA. A P value of less than .05 was determined as significant.
Results
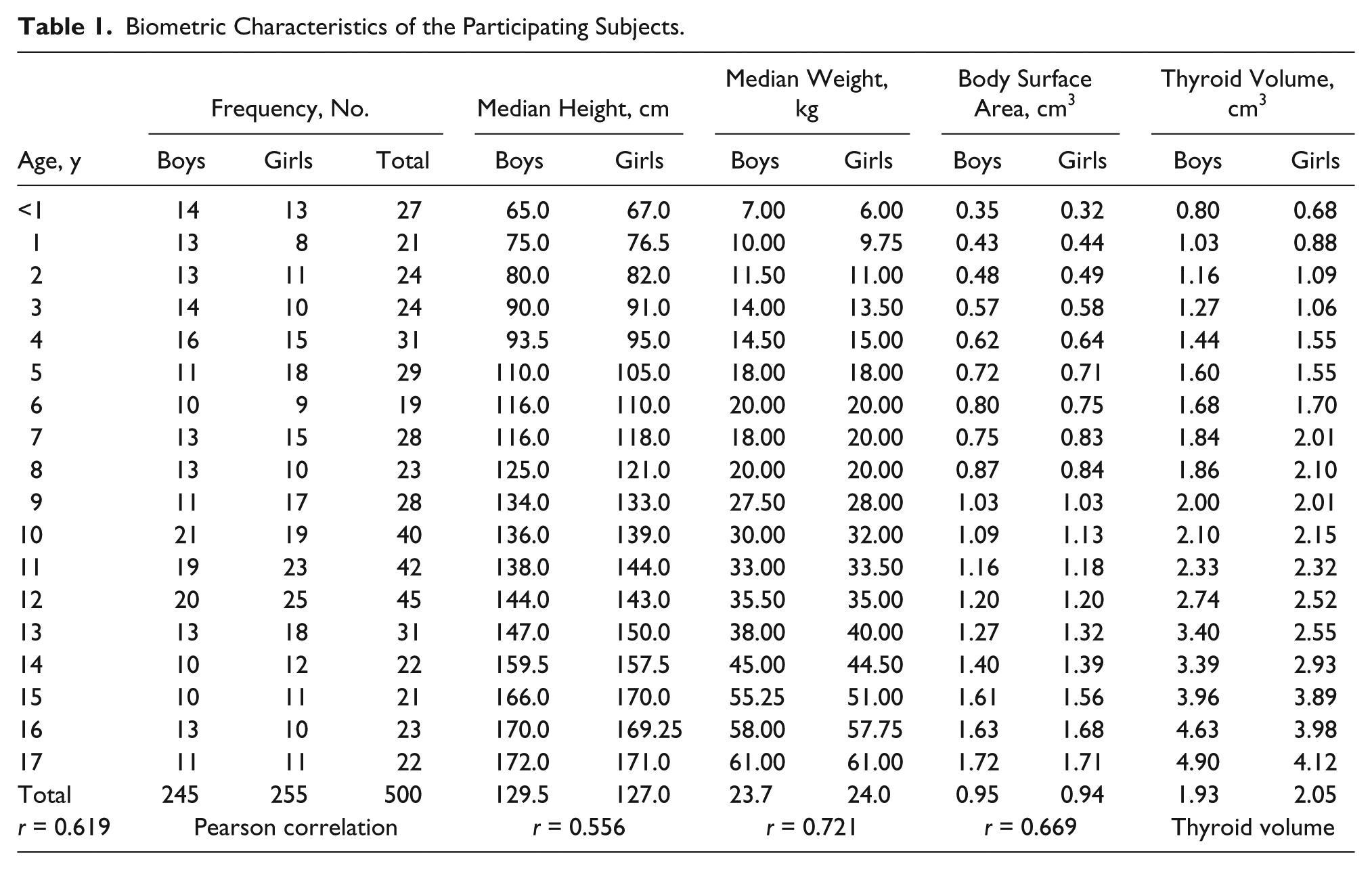
In all, 245 males (48.8%) and 255 females (51.2%) were sonographically examined. The highest frequency of the children studied fell within the 12-year age group (n = 45; 9%), while the 6-year age group showed the least frequency (n = 19; 3.8%). There was a proportionate increase in height, weight, and BSA with thyroid volume. The median BSA for males (0.95) was higher than for females (0.94), but the thyroid volume in males was slightly lower (1.93 cm3) than that of females (2.05 cm3) (see Table 1). Statistically, there was no sex difference in thyroid volume as well as between the right and left lobes.
Biometric Characteristics of the Participating Subjects.
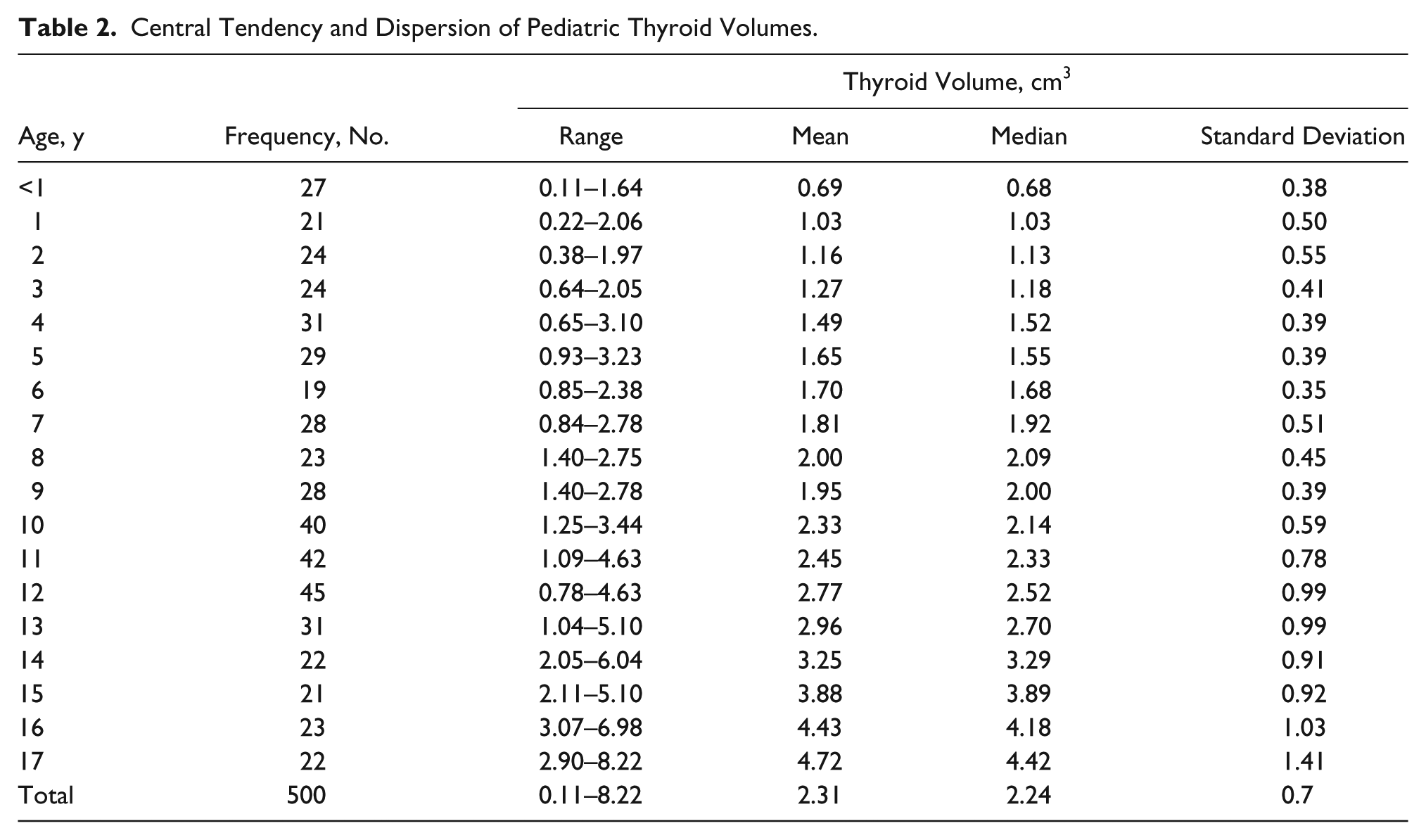
The thyroid volume range for the preschool age children (0–5 years) was 0.11 to 3.23 cm3 while the range for the school-age children (>5 years) was 0.85 to 8.22 cm3. The mean thyroid volume for the study population was 2.31 ± 0.7 cm3 (see Table 2). A Pearson correlation showed a highly significant relationship between the thyroid volume and age, height, weight, and BSA. A linear relationship between thyroid volume and all the anthropometric parameters was also observed (see Table 3).
Central Tendency and Dispersion of Pediatric Thyroid Volumes.
Correlation of Mean Pediatric Thyroid Volume With Age, Height, Weight, and BSA.
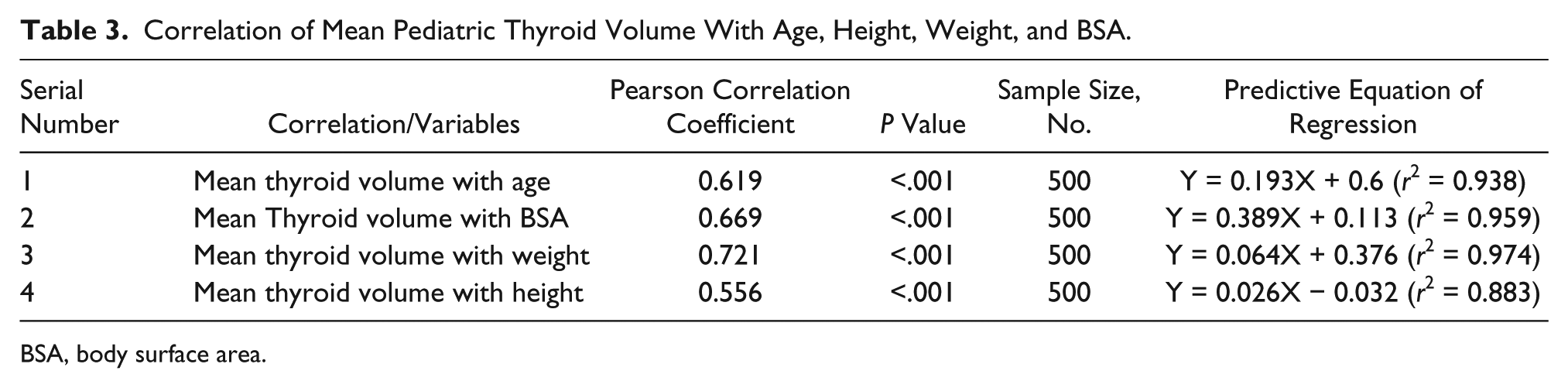
BSA, body surface area.
The thyroid volume from this research is comparable to another work in this locality and was well below the normal value recommended by the WHO (see Table 4). A nomogram was derived using the 75th percentile of the study population (see Figure 1).
Comparison of Pediatric Thyroid Volumes.
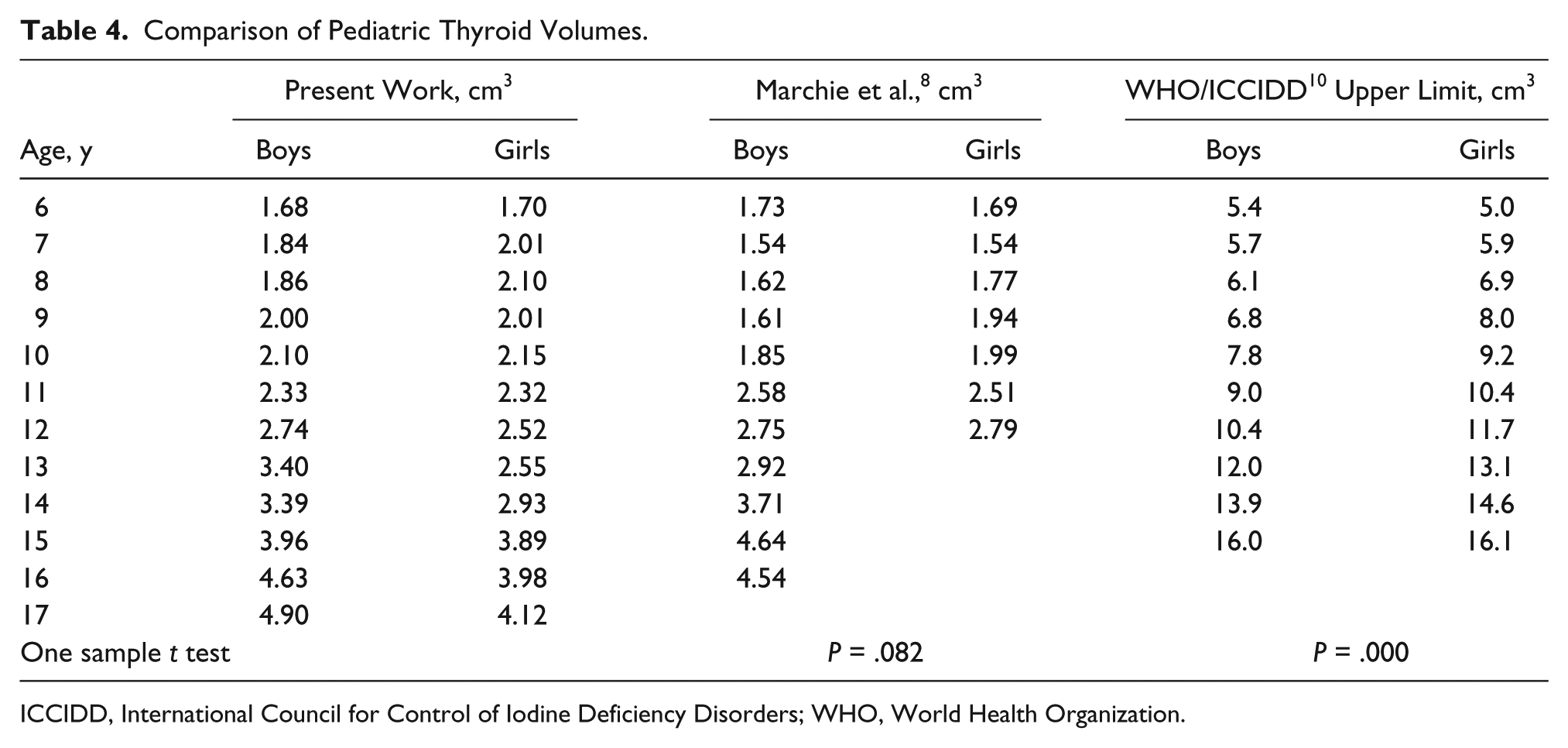
ICCIDD, International Council for Control of Iodine Deficiency Disorders; WHO, World Health Organization.
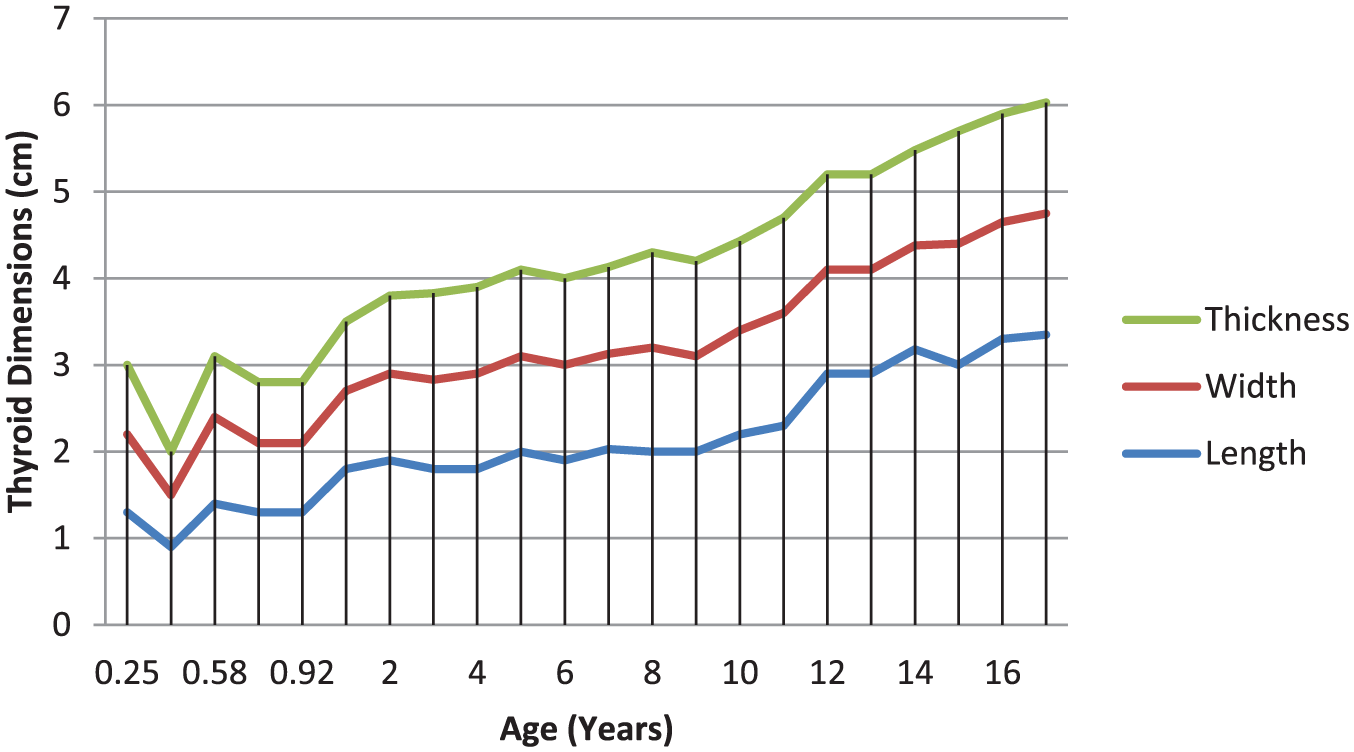
Pediatric thyroid length, width, and thickness (depth) compared to age from 75th percentile in the study.
Discussion
Iodine deficiency disorder (IDD) is a global public health problem and represents the main cause of preventable mental retardation and permanent brain damage to the fetus, infant, and adolescent throughout childhood. Thyroid gland enlargement as a result of iodine deficiency presents as a goiter.8,18 Volumetric evaluation of the thyroid gland is based on the use of an ellipsoid model where the height, width, and depth of each lobe are measured and multiplied. The obtained result is then multiplied by a correction factor. 10
This study established a range and mean thyroid volume of 0.11 to 6.04 cm3 and 2.31 ± 0.7 cm3, respectively, in infants and children in this specific population. The mean thyroid volume in this study was similar to that obtained by Marchie et al. 8 among school-age children in Benin City, Nigeria (Table 4). It is possible that geographical, cultural, and dietary factors may have contributed to this similarity. 8
There was significant difference (P < .05) in the present study values compared with the upper limit of normal thyroid volume in the WHO reference values based on European schoolchildren. This dissimilarity was noted in previous studies.7,8,19 There may be a need to carry out a multinational study on thyroid volume measurement without emphasis on race/ethnicity, using standardized measurement techniques and the same transducer frequency. Healthy subjects without a goiter or abnormal thyroid function tests will be included. The reference values obtained from the study could possibly apply to all races and ethnic groups.
Thyroid volume was observed to increase with age in both sexes. This is in agreement with previous studies.4,8 Pearson correlation showed a highly significant relationship between the thyroid volume and age (r = 0.619), height (r = 0.556), weight (r = 0.721), and BSA (r = 0.669). This finding agrees with previous studies.4,7,8
There was no significant difference in thyroid sizes between the two sexes in the present study. This, however, varies with what was observed in some other studies.11,20 Apparently, nonexistence of a significant difference in BSA between the sexes in the present study may have accounted for this. Previous studies had shown age and BSA to be the best predictors of thyroid gland volume.1,21
Conclusion
Thyroid size has been noted to vary with geographical location as well as cultural, racial, and nutritional differences. There are no documented values of thyroid volume among Nigerian preschool children, although values for school-age children have been obtained from two different locations in Nigeria. Normative values of thyroid volume by sonography have been established for infants and children younger than 18 years in our locality. These values will be invaluable in establishing a cutoff level when screening for a goiter.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.