
Abstract
Background:
Malposition may occur during peripherally inserted central catheter insertion. Accurately measuring the length of a peripherally inserted central catheter is crucial to preventing malposition, including “long peripherally inserted central catheter placement,” in which the tip of a peripherally inserted central catheter is deeper than the target position. The traditional method of measuring peripherally inserted central catheter length involves measuring from the insertion site to the parasternal notch and down to the third or fourth intercostal space, which may result in overestimation because of the thickness of the pectoralis major and anterior chest wall. To avoid this overestimation, the authors developed and tested a modified method for reducing long peripherally inserted central catheter placement.
Methods:
This study employed a retrospective design. Chest X-rays were used to examine the peripherally inserted central catheter tip positions in 48 patients in the medical intensive care unit who had undergone peripherally inserted central catheter insertion. The traditional and modified measurement methods were used to measure the peripherally inserted central catheter length in 17 and 31 patients, respectively. Fisher’s exact test was used to examine between-group differences in the incidence of different types of peripherally inserted central catheter malposition.
Results:
The peripherally inserted central catheter tip position was near the target position in five patients (29.41%) in the traditional measurement group and 17 patients (54.84%) in the modified measurement group (p = 0.132), whereas long peripherally inserted central catheter placement occurred in six patients (35.29%) in the traditional measurement group and one patient (3.23%) in the modified measurement group (p = 0.006). However, the incidence of other types of peripherally inserted central catheter malposition did not differ significantly between the groups.
Conclusions:
The results of this study that the proposed modified measurement method may be able to reduce the incidence of long peripherally inserted central catheter placement among medical intensive care unit patients. The method must be further evaluated in prospective studies and studies with larger sample sizes in the future.
Introduction
Peripherally inserted central catheters (PICCs) have been widely used for vascular access since the 1980s. In the treatment of critically ill patients, PICCs can be used to measure central venous pressure and administer drugs and nutrition. 1 Compared with centrally inserted central catheters (CICCs), PICCs are associated with fewer complications, including fewer bloodstream infections. 2 PICCs can be inserted using aseptic techniques by trained nurses and physicians. 3 PICCs can also be placed by technicians, and PICC insertion by technicians has the same safety as insertion by radiologists. 4 In a study by Lee et al., 5 the author used the blind pushing technique for inserting PICCs and determined that the blind pushing technique is associated with a lower incidence of upper-extremity deep vein thrombosis and other complications compared with conventional PICC placement techniques.
In intensive care units (ICUs), PICCs are often used for central venous access. PICCs are safer and are associated with lower rates of infection than traditional central venous catheters (CVCs), especially when used long term. 6 Most ICU patients require intravenous fluids and antibiotics, and the use of devices that provide stable and long-term venous access is crucial in the treatment of such patients. However, blind or ultrasonography-guided bedside PICC insertion can lead to catheter tip malposition and procedure-related complications. 7 Additional methods for reducing the risk of tip malposition during PICC insertion, especially when performed without fluoroscopy, are necessary.
Intravenous electrocardiogram (ECG) monitoring could be used to guide catheter positioning during PICC insertion because a high P-wave amplitude can be observed when the tip of a PICC is at the superior vena cava (SVC)–right atrium junction. 8 To facilitate CVC insertion, researchers developed an accelerated Seldinger technique, which was determined to be faster and easier than the modified Seldinger technique. 9 However, PICC malposition still occurs when this technique is used. In our experience of placing PICCs for ICU patients, doctors have frequently encountered “long PICC placement,” in which the tip of a PICC is deeper than the target position. The traditional measuring method involves using a ruler to measure along the body’s surface. However, this method may result in overestimation when measuring women with prominent breast tissue or patients with prominent soft tissues in the chest wall. To address this problem, the authors developed a modified method for measuring PICC length in the ICU. The present study showed that the proposed method can effectively reduce the incidence of long PICC placement.
Patients and methods
Patients
This retrospective cohort study was conducted in the intensive care unit of Kaohsiung Medical University Chung-Ho Memorial Hospital in Taiwan from January 2019 to December 2020. During this period, data of patients who meet the PICC indication criteria and consent to PICC placement will be included, whereas those who do not will be excluded. A total of 48 patients who had undergone PICC insertion for the following indications: (1) vascular access; administration of (2) total parenteral nutrition (TPN), (3) vasopressors, (4) chemotherapy; or (5) long-term administration of antibiotics were enrolled. Contraindications for PICC insertion include the following: (1) small basilic and brachial arm vein diameters, (2) the need for femoral access because of a mediastinal or SVC syndrome, (3) particular conditions of the arms (e.g., paresis, local skin infections, presence of devices from orthopedic procedures with a block of the arm, local severe burns, or prior removal of the axillary lymphatic nodes), and (4) severe renal impairment associated with a potential indication for dialysis and the need to preserve the deep veins of the arms for potential placement of an arteriovenous fistula. 10 Patients were given PICC insertion when they exhibited the indication for PICC use and did not have any contraindications. In this study, none of the PICCs were the initial devices for the patients. Critically ill patients in the intensive care unit primarily received CICC as their central venous catheter. The patients included in this study were those who had achieved stability in their medical condition or had transitioned to palliative care before PICC insertion.
PICC insertion procedure
The PICCs were inserted by critical care physicians under ultrasound guidance and standard sterile conditions. Five French (Fr) double-lumen Power PICCs (Bard Access Systems) were used in this study. A Bard Site Rite 5 Sonogram Machine Ultrasound System (Bard Access Systems) was used to examine the vein at the insertion point. A Site~Rite* Needle Guide was used to guide the needle. Since this study involves patients in critical care, most of whom have swollen soft tissues and lower blood pressure, it is challenging to assess blood reflux without maintaining a negative pressure situation. Therefore, the authors utilized a T-connect to sustain negative pressure. Furthermore, the premise of this study is to offer novice practitioners a more accessible training approach. Critical care physicians inserted each catheter using the modified Seldinger technique and used a T-connector to maintain negative pressure during puncture and facilitate the insertion of the guidewire. First, the operator connected the needle to the T-connector. After the operator inserted the needle into the skin, the assistant maintained negative pressure from the syringe through the T-connector. After drawing blood from the target vein, the operator removed the T-connector from the needle and inserted the guidewire (Figure 1).
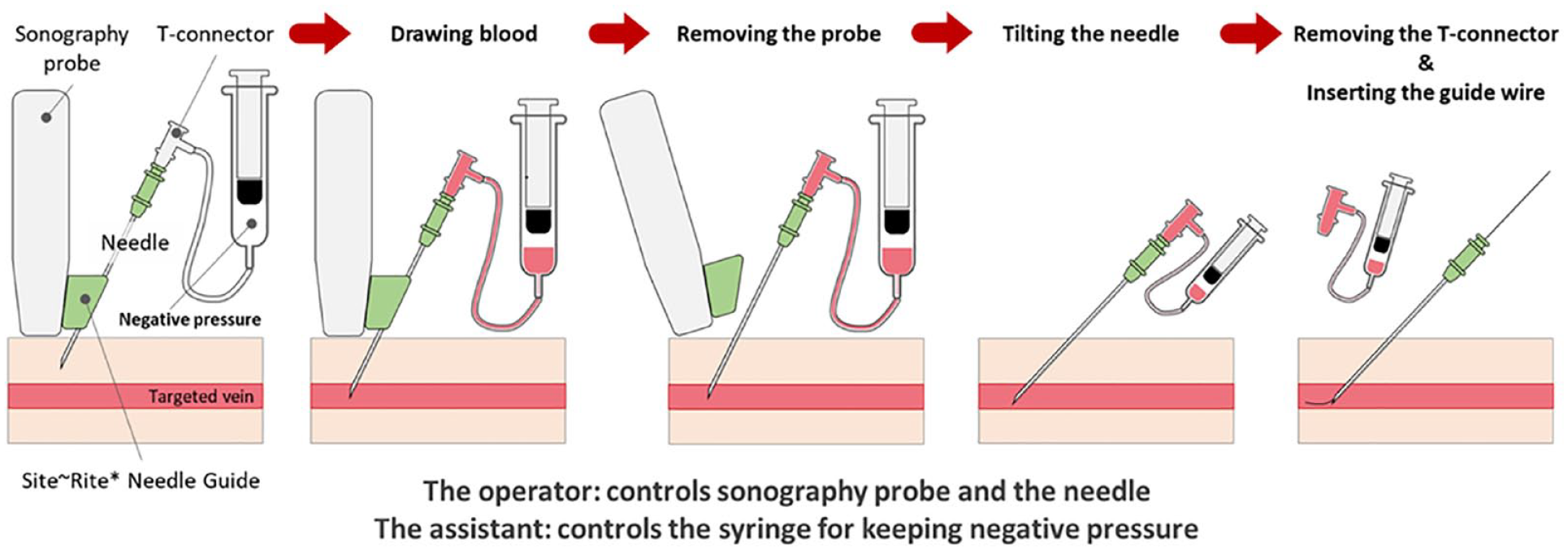
Connecting the T-connector with the needle and syringe to maintain negative pressure during puncture.
Long PICC placement is common. To address this problem, the authors developed the modified method of measuring the length of a PICC presented herein. The traditional measurement method involves measuring from the insertion site to the parasternal notch and down to the third or fourth intercostal space. This method may result in an overestimation of the length of a PICC because of the thickness of the pectoralis major and anterior chest wall. To avoid this overestimation, the authors separated the total length from the insertion site to the parasternal notch into two segments: segment 1, which stretches from insertion site to the medial wall of the axilla, and segment 2, which stretches from the end of segment 1 to the surface of the pectoralis major and terminates at the parasternal notch (Figure 2).

Modified method of measuring PICC length. The total length from the insertion site to the junction of the subclavian vein and SVC should be equal to the sum of the lengths of segments 1 and 2. Compared with the traditional measurement method, the modified measurement method is more efficient and precise.
After placing a PICC, the operator flushed the PICC with 10 mL of saline, disinfected the skin around the insertion site, and covered the insertion site with 3 M Tegaderm Transparent Film Dressing. Chest radiography was used to examine the position of the tip of the PICC.
X-ray examination of PICC tips
According to the recommendations of the infusion nurses society, the tip of a central venous catheter should be located at the lower third of the SVC, close to the entrance to the right atrium. 11 In this study, chest X-ray images were used to determine the position of the tip of each PICC. The carina was used as an anatomical landmark, and 1.6–4 cm under the carina was considered the optimal position for the PICC tip. 12 Each chest X-ray was independently verified by Wei-An Chang, one of the authors.
Data collection
The variances gathered in this study encompassed a range of factors, including gender, age, sequential organ failure assessment (SOFA) scores, 13 Acute Physiology and Chronic Health Evaluation (APACHE) II scores, 14 duration of PICC placement, insertion arm side, punctured vein, purpose of PICC insertion, reasons for PICC removal, and PICC malposition types. Data were collected by performing a patient chart review.
Statistical analysis
Fisher’s exact test was used to evaluate between-group differences. 15 The significance level was set at p < 0.05.
Ethics approval and consent to participate
This is a retrospective study. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUHIRB-E(I)-20220063). The IRB waived the requirement of obtaining informed consent from the patients because of the retrospective study design.
Results
From 1 June 2019 to 31 December 2020, 48 mobile ICU patients who had undergone PICC insertion were enrolled in this retrospective study. The sample comprised 30 men (62.5%) and 18 women (37.5%) with a median age of 62 years (interquartile range (IQR) = 28–91). The median SOFA and APACHE II scores were 7 (IQR = 6–10) and 20 (IQR = 25–27), respectively. The median duration of PICC insertion was 19 days (IQR = 9.75–30 days). The most commonly punctured vein was the basilic vein (n = 27, 56.25%), followed by the cephalic vein (n = 28, 37.5%). The most common purpose of PICC insertion was vascular access (n = 28, 58.33%); some of the other patients required PICCs to receive TPN (n = 9, 18.75%) or vasopressors (n = 8, 16.67%). Death was the most common reason for PICC removal (n = 25, 52.08%), followed by patient discharge; other reasons included occlusion (n = 4, 8.33%) and infection (n = 1, 2.08; Table 1).
Patient characteristics.

IQR: interquartile range; PICC: peripherally inserted central catheter; SOFA: sequential organ failure assessment; APACHE II: acute physiology and chronic health evaluation II.
PICC malposition was noted on the chest X-rays of 26 of the 48 patients. PICC malposition types discussed in this article are primary malposition. The most common type of malposition was malposition at the jugular vein (n = 9, 34.62%), followed by long PICC placement (n = 7, 26.92%; Table 2). One malposition at the jugular vein and one at the subclavian vein were automatically corrected without additional intervention. One patient exhibited axillary stenosis; a radiologist was consulted for the reinsertion of the PICC.
PICC malposition types.

PICC: peripherally inserted central catheter.
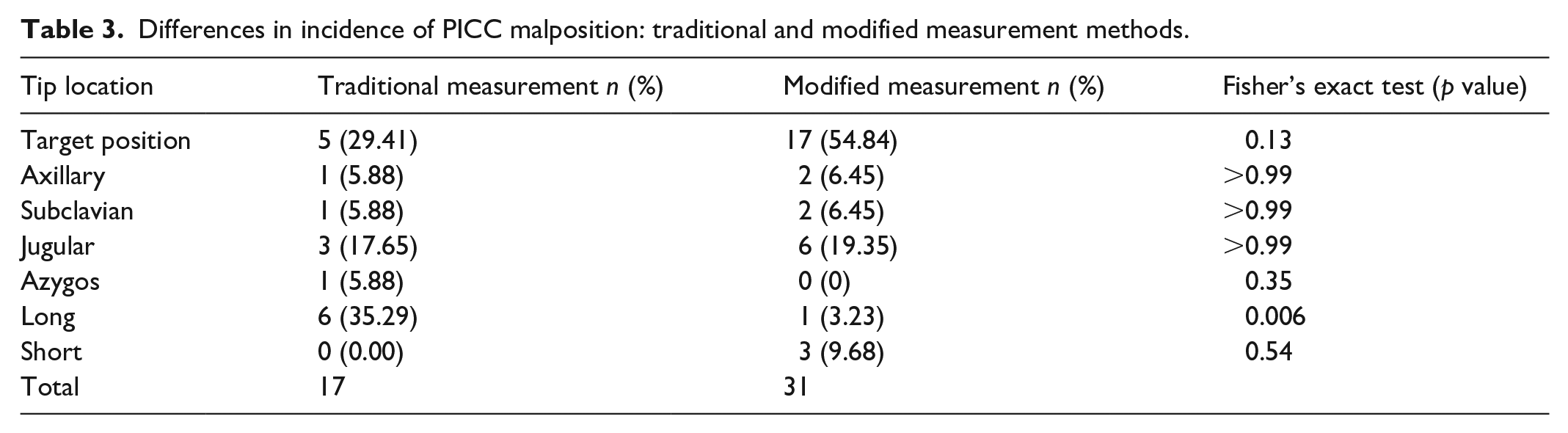
The traditional method and modified method were used to measure PICC length in 17 and 31 patients, respectively. The PICC tip position was near the target position in five patients (29.41%) in the traditional measurement group and 17 patients (54.84%) in the modified measurement group (p = 0.13), whereas long PICC placement occurred in six patients (35.29%) in the traditional measurement group and one patient (3.23%) in the modified measurement group (p = 0.006; Table 3). These results indicate that the modified method of measuring PICC length could reduce the incidence of long PICC placement.
Differences in incidence of PICC malposition: traditional and modified measurement methods.
Discussion
PICCs may serve as a relevant alternative to CICCs for patients who require medium-term parenteral support. 16 Polyurethane power-injectable PICCs may have benefits for patients requiring critical care. 10 Although infections associated with PICC insertion have been reported, the risk of bloodstream infections associated with PICCs is not higher than that associated with conventional central catheters. Therefore, PICCs are still generally considered safe. 2
Despite the relative safety of PICCs, tip malposition may occur during PICC insertion. Therefore, real-time ultrasound guidance is crucial during such procedures. 17 ECG has been widely used to confirm the PICC tip location. A study investigating the accuracy and advantages of ECG in PICC tip localization shows a significant improvement in the accuracy of the catheter tip position (RR: 1.17, 95% CI: 1.04–1.32, N = 3194) for participants in the ECG group compared to those in the landmark group. 18 Fluoroscopy (if available) and ECG-guided PICC tip location techniques can be used to determine the position of a PICC tip. ECG-guided PICC tip location is convenient and does not require patients to be exposed to radiation.19,20 The traditional PICC placement method still has some limitations, including its difficulty and the risk of air embolism and excessive bleeding. The accelerated Seldinger technique is convenient and can be used to avoid these problems. The traditional measurement method measures along the patient’s body surface. This approach might lead to overestimation when measuring patients with prominent breast tissue or prominent chest wall soft tissues. Therefore, this modified method was used to measure the length of PICC in this study. The result showed that the incidence of long PICC placement is 35.29% in the traditional measurement group and 3.23% in the modified method group (p = 0.006).
After a central venous access device is placed, the tip position must be examined. The Food and Drug Administration suggested that the tip of a central venous catheter must be in the lower third of the SVC and above the cavoatrial junction. 21 Catheter malposition is categorized as “primary” when it occurs during insertion and as “secondary” when the catheter tip spontaneously migrates in the weeks to months following insertion. 10 A high proportion (63%) of incidents of PICC malposition occur after blind placement of a catheter. 22 The risk of PICC malposition is reportedly higher when a PICC is placed in the right upper limb than when it is placed in the left upper limb. The highest risk of malposition is associated with cephalic vein puncture, followed by brachial vein puncture. The risk of vein puncture in the lower part of the elbow is higher than the risk of vein puncture in the upper part of the elbow. The left upper limb, specifically the upper part of the elbow joint, is considered the optimal puncture site, and the basilic vein is the first-choice vein for PICC insertion. 23 In one randomized controlled trial, the incidences of PICC tip malposition in the ipsilateral internal jugular vein, subclavian vein, brachiocephalic vein, axillary vein, and distal position (right atrium and beyond) were 7.4%, 8.7%, 9.4%, 2.7%, and 7.4%, respectively. 24 Several studies have reported that tip malposition may lead to catheter malfunction. 25 In this study, it was observed that the tip position of the PICC was located in the internal jugular vein in 19.35% of patients. This may be attributed to the angle of the vein. Due to the limited mobility of patients in the ICU, most of the insertions were performed at the bedside. As a result, without the assistance of fluoroscopy during the procedure, it was only after the placement was completed and a chest X-ray was taken that the tip’s location in the internal jugular vein was discovered.
A catheter tip position higher than 4 cm above the cavoatrial junction (i.e., in the middle or upper third of the SVC or in the brachiocephalic vein) is associated with a significantly higher risk of catheter malfunction and a higher risk of venous thrombosis relative to a lower position in the SVC or close to the cavoatrial junction. 26 Using a Sherlock 3CG Diamond Tip Confirmation System and an intracavity ECG guidance system in combination is an effective approach to detecting the stylet of a PICC catheter and confirming the final position of the PICC tip. 27 However, not every hospital has access to these systems. The modified measurement method proposed herein can help hospitals without effective devices for examining the position of the tip of a PICC during the placement procedure to minimize the rate of long PICC placement. Furthermore, the PICC used in the medical intensive care unit needs to be measured for its length before placement. If the initial length measurement is inaccurate, it is still possible to have an excessive or insufficient extracorporeal portion of the PICC after placement, even when confirming the tip position after insertion. Therefore, this modified method may potentially improve this condition.
Limitations
Nevertheless, this study has some limitations. This is a single-center study. The number of patients enrolled was relatively small, and the study employed a retrospective design. Power analysis for sample size calculation was not done in this study. The proposed method should be further evaluated in larger studies and prospective studies in the future.
Conclusion
The present study showed that the modified measurement method may be able to reduce the incidence of long PICC placement among ICU patients. The traditional measurement method measures along the patient’s body surface. This approach might lead to overestimation when measuring patients with prominent breast tissue or prominent chest wall soft tissues. The measurement method employed in this study could effectively address this issue in a simple and efficient method. The main limitation of this study is its small sample size. Additional studies with larger sample sizes are required to further evaluate the benefits of the modified measurement method proposed herein.
Footnotes
Acknowledgements
The authors would like to thank the Department of Medical Research of Kaohsiung Medical University Chung-Ho Memorial Hospital. This manuscript was edited by Wallace Academic Editing.
Authors’ contributions
Conceptualization: W.-A.C.; formal analysis: C.-M.C., C.-H.C., C.-C.S., M.-J.T.; investigation: T.-C.Y., C.-M.C., C.-H.C., C.-C.S., M.-J.T., W.-A.C.; writing—original draft preparation: W.-A.C. and T.-C.Y.; writing—review and editing: W.-A.C. All authors have read and agreed to the published version of the manuscript.
Availability of data and materials
All of the material is owned by the authors and/or no permissions are required. The results/data/figures in this manuscript have not been published elsewhere, nor are they under consideration by another publisher.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the support of research grants from the Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUH110-0M09).
Trial registration
Not applicable.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.