
Abstract
Objectives:
It is important to know the range of normal vertebral artery (VA) flow volume. Diminished VA flow volume is associated with vertebrobasilar insufficiency. The study aim was to investigate the relationship between the posterior communicating artery (PCoA) calibration and the VA flow parameters, in patients with no underlying cerebrovascular disease, below 50 years of age.
Materials and Methods:
The study population consisted of 102 cases below 50 years of age. The basilar artery (BA), internal carotid artery (ICA), and the PCoA calibrations were measured with magnetic resonance angiography. The VA flow parameters (maximum systolic velocity, end-diastolic velocity, mean velocity, VA flow volume, and VA calibration) were measured with duplex sonography.
Results:
There was no statistically significant difference between these two imaging groups, in terms of VA Vmax, VA flow volumes, VA calibrations, and BA calibrations. However, the mean right ICA and mean left ICA calibrations were significantly higher in group 2 than group 1 (P < .01). There was no significant correlation between mean PCoA calibration and mean Vmax, mean calibration, and the total flow volume of vertebral arteries.
Conclusion:
The findings indicate that the VA flow rate may be relatively maintained, regardless of PCoA measurements in this study.
Keywords
Vertebrobasilar insufficiency (VBI) is a pathology that develops due to hemodynamic changes resulting from a decrease in vertebrobasilar arterial system flow. Vertigo is the most important symptom of VBI. 1 However, there may be other causes of vertigo, especially in the inner ear diseases (atherosclerosis, cholesteatomas, tumors).2–4 Cerebral perfusion decreasing below a critical level is important as it can cause neurological findings. A decrease in cerebral blood flow below 10 mL/100 g to brain tissue results in an infarction. 5 The vascular flow volume (FV) is also an important parameter in the evaluation of vertebral artery (VA) hemodynamics and vertebrobasilar perfusion. 6 Duplex sonography (DS) is an inexpensive, noninvasive modality for the evaluation of extracranial carotid and vertebral arteries. 7 Some studies have found a significant reduction in blood flow and vessel diameter in VBI patients, compared with control patients, based on both right and left circulation. 8 There are reports that it can be between 100 and 300 mL/min in hemodynamically normal individuals. 9 It is important to know the range of the normal VA volume and its change due to collaterals such as the posterior communicating artery (PCoA). However, since the brain has a complex blood supply system, particularly the circle of Willis (COW), which can rely on collateral flow, up to a point, as occlusive disease progresses, within a single vessel. The COW plays an important role in the redistribution of blood to intracranial arteries. 10 The relationship between the PCoA and VA flow parameters has not been well studied. Hong and Hendrikse suggested that there may be a significant decrease in vertebrobasilar system flow in patients, with a fetal-type COW formation.7,10 In that study, it was difficult to relate VBI with the decrease in VA volume. To be able to diagnose VBI, the development of PCoA should also be considered in the evaluation. The aim of this research was to investigate the relationship between PCoA calibration and VA flow parameters, in patients below the age of 50 years, with no underlying cerebrovascular disease.
Materials and Methods
Patient Selection
This prospective study was approved by the Clinical Research Ethics Committee of the host university (study number 01/III—01/03/2018). All subjects signed an informed consent. One hundred and two patients, below 50 years of age, were referred for magnetic resonance angiography (MRA), during June 2018 and September 2019. The purpose of the referral was to investigate the patient’s headache. To minimize possible atherosclerosis, the inclusion criteria were to consent patients below 50 years of age. The following were exclusion criteria: patient cases of VBI due to significant hemodynamic stenosis in the carotid and vertebral arteries, patients with vasculitis, patients with a history of a previous cerebrovascular attack, and patients with arteriovenous malformation in the brain.
MRA Examination and Measurements
Magnetic resonance angiography images were taken with a 3T magnetic resonance system using a 16-channel head-dedicated coil (Siemens Skyra, Erlangen, Germany). The MRA was performed with a 3D time-of-flight method. The examination parameters were TR 21 ms, TE 3.43 ms, FA 18°, and NEX 1 matrix 320 × 275. The MRA images were examined at a Syngovia workstation (Siemens, Germany). Source images and maximum intensity projection (MIP) images were evaluated together. The intracranial internal carotid arteries (ICAs), basilar artery (BA), and PCoA’s calibrations were recorded (Figure 1). Measurements were made on the axial MIP and axial source images. The ICA measurements were performed from the cavernous segment, and BA calibration was performed caudally to the superior cerebellar artery branch. The PCoA calibrations were performed in the middle segment between posterior cerebral artery (PCA) and ICA (Figure 2). For each case, the PCoA calibrations on both sides were summed and divided into two to find the mean PCoA value for each case [(right PCoA + left PCoA)/2]. Then the mean PCoA calibrations of the cases were summed and divided by the number of cases (∑ average PCoA calibration/102) to find the mean PCoA calibration (mPCoAC) of all cases. The cut-off (mPCoAC) used to separate group 1 and group 2 was calculated as 0.95 mm Those below the mPCoAC value were determined as group 1 and those above were determined as group 2.
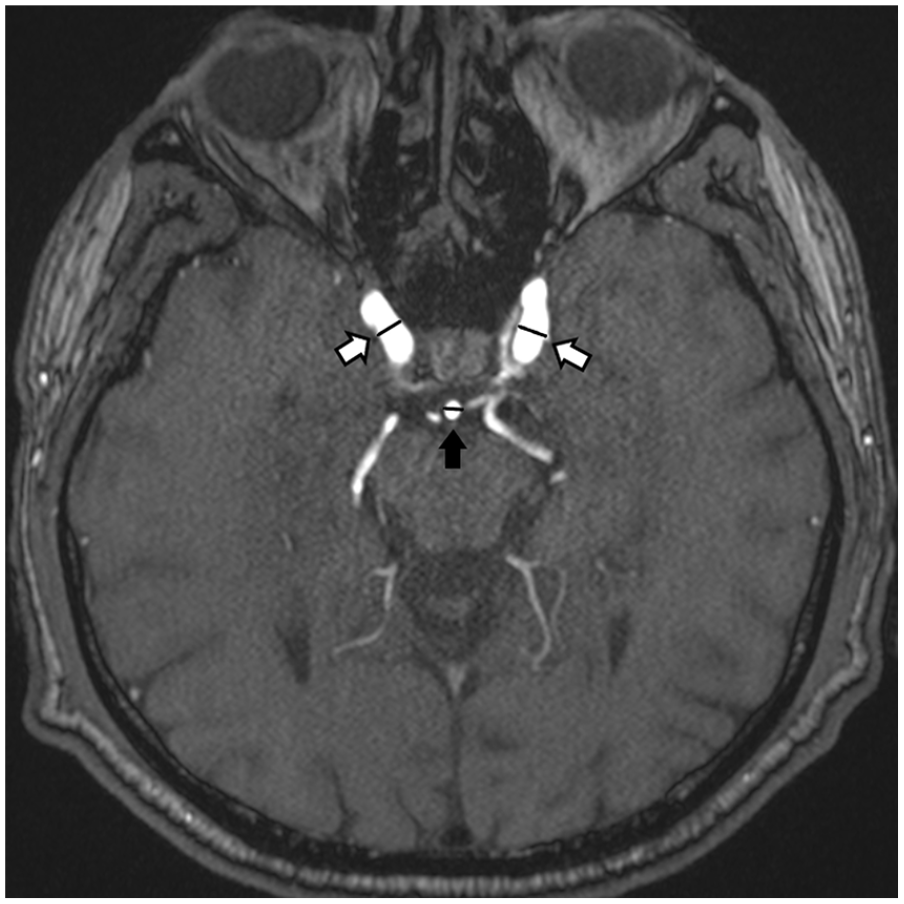
On the axial MRA image, both white solid arrows show the measured segments of ICA. The black solid arrow indicates the area where the basilar artery was measured. ICA, internal carotid artery; MRA, magnetic resonance angiography.
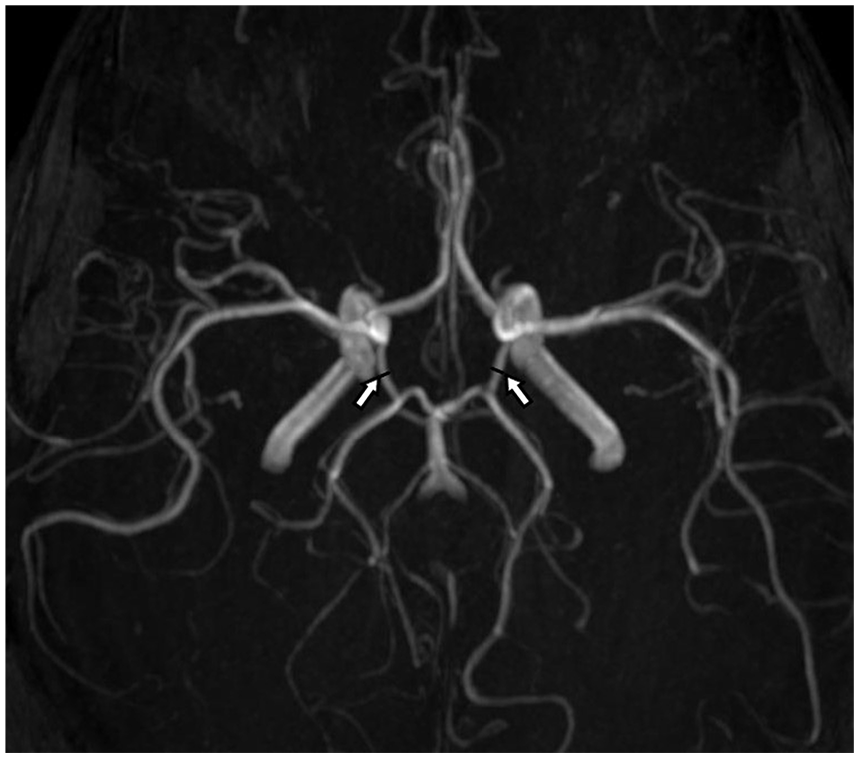
On the axial MIP image, both white solid arrows show the measured segments of PCoA. MIP, maximum intensity projection; PCoA, posterior communicating artery.
Duplex Examination and Measurements
The DS examinations were performed in a supine position after the patient rested for 15 minutes, in a quiet room. The DS examination was preformed with a Aplio 500 and a linear transducer 11L4 PLT-704SBT (Canon Medical Systems, Otawara, Japan). First, the visible segments of the ICA and VA were evaluated for significant stenosis or occlusion. The VA calibrations, FV, maximum velocity (Vmax), end-diastolic velocity (Ved), mean velocity (Vm) were measured and recorded. The Doppler angle was adjusted between 30° and 60° during the DS (Figure 3). The VA calibration was measured with color Doppler, during the systolic phase. The VA parameters were measured at the level of the transverse processes, at C4-5 level. Both the MRA and DS images were evaluated by a radiologist, with 20 years of experience.
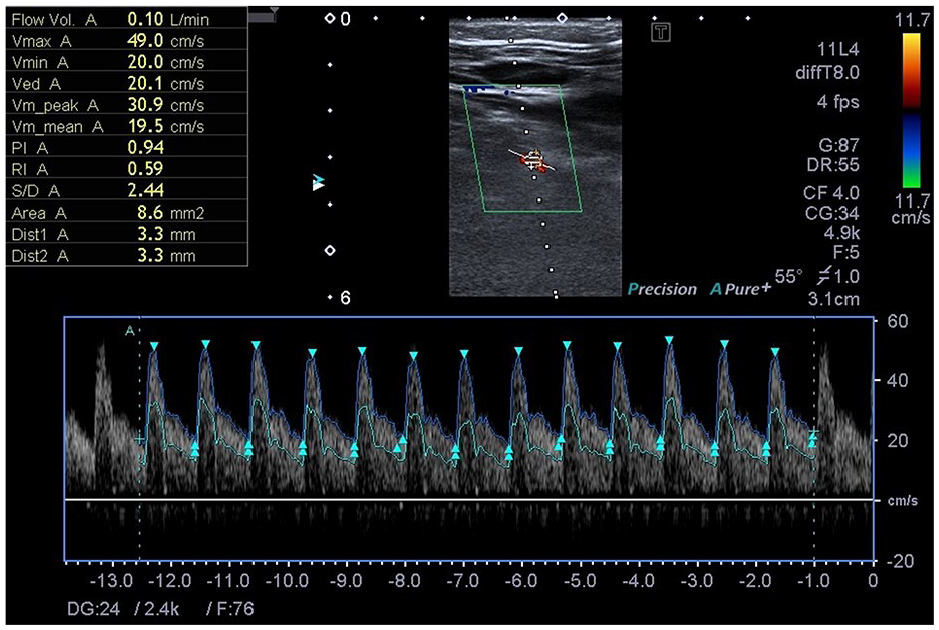
The duplex measurements, from the right vertebral artery, for a 39-year-old female are provided. In this case, the angle was set to 55° insonation. In the upper left corner of the image, Doppler parameters are provided for this patient.
Statistical Analysis
A descriptive analysis was performed to generate demographic data. The Student t test was used to compare the mean values of the groups. Statistical significance was determined as P < .05, a priori. A Pearson correlation analysis was performed to determine the strength of association between the mPCoAC, VA Vmax, VA calibration, and total VA volume values. SPSS was used for all statistical analyzes (IBM SPSS Statistics 20).
Results
The data were generated from 66 patients and 64.7% were female, while 35.3% were male. There was no significant difference between the mean age of females and males (P = .40).
Evaluating DS flow parameters, the right mean VA velocity was 25.45 cm/s for females and 23.33 cm/s for males and the difference was statistically significant (P = .01). There was no statistically significant difference in terms of bilateral Vmax, Ved, VA FV, and VA calibrations (see Table 1). Within the female group, the mean Vmax was 45.76 cm/s (range = 17.75–63.60 cm/s), total VA FV was 299.91 mL/min (range = 110–490 mL/min), the mean VA calibration was 3.45 mm (range = 2–4.2 mm) was measured. Within the male group, the average Vmax was 45.23 cm/s (range = 33.55–58.10 cm/s), the total VA FV was 311.17 mL/min (range = 210–450 mL/min), the average VA calibration was 3.65 mm (range = 3.25–4.25 mm) was measured.
The Study Cohort’s Doppler Measurements Taken in Both Vertebral Arteries.

Abbreviations: VA.Cal, vertebral artery calibration (mm); VA.Vol, vertebral artery flow volume (mL/min); Ved, end-diastolic velocity (cm/s); Vmax, maximum systolic velocity (cm/s); Vmean, mean velocity (cm/s).
The evaluation of the MRA images demonstrated that the right ICA (RICA) calibration was 4.77 among males and 4.46 mm among the females. The BA calibration was 3.25 mm in males and 3.08 mm in females. The gender flow value differences were statistically significant (P < .05). There was no statistically significant difference between left ICA (LICA) and bilateral PCoA calibrations (Table 2).
The Study Cohort’s Vessel Diameter Measurements, Taken With Magnetic Resonance Angiography.

Abbreviations: BA, basilar artery; LICA, left internal carotid artery; L.PCoA, left posterior communicating artery, RICA, right internal carotid artery; R.PCoA, right posterior communicating artery.
The vessel diameter measurements were recorded in millimeters.
The cut-off value, used to separate group 1 and group 2, was calculated as 0.95 mm. Group 1 (mean calibration is 0.53 ± 0.26 mm) below this cut-off was 45 persons and group 2 (mean calibration is 1.27 ± 0.16 mm) above it was 57 persons. There was no statistically significant difference between these two groups in terms of VA Vmax (P = .68), VA FVs (P = .35), VA calibrations (P = .09), and BA calibrations (P = .09). However, mean RICA and LICA calibrations were significantly higher in group 2 than group 1 (P < .01). These research findings are provided in Table 3.
The Cohort’s Comparison of Doppler and Magnetic Resonance Angiography Measurements for Groups 1 and 2.
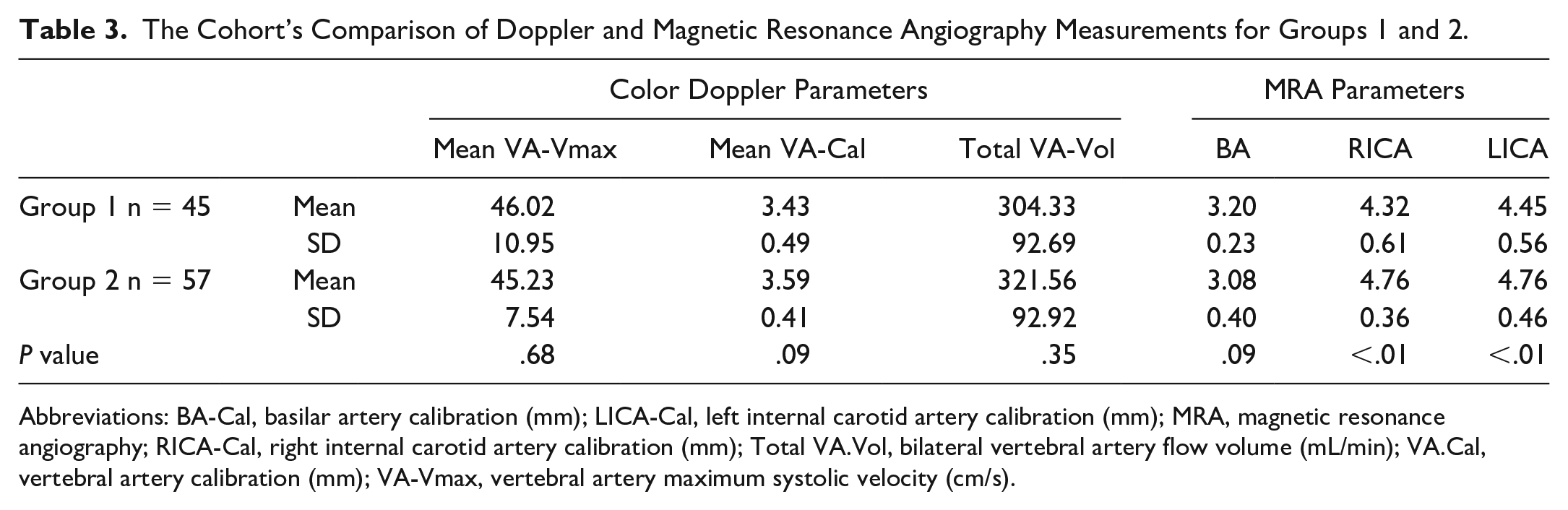
Abbreviations: BA-Cal, basilar artery calibration (mm); LICA-Cal, left internal carotid artery calibration (mm); MRA, magnetic resonance angiography; RICA-Cal, right internal carotid artery calibration (mm); Total VA.Vol, bilateral vertebral artery flow volume (mL/min); VA.Cal, vertebral artery calibration (mm); VA-Vmax, vertebral artery maximum systolic velocity (cm/s).
There was no significant correlation between the mean PCoA calibration and mean Vmax (r = −.11; P = .29), mean calibration (r = −.08; P = .44), and total FV (r = −.14; P = .17) of vertebral arteries.
Discussion
This study cohort demonstrated that there was no significant relationship between PCoA calibration and VA FV, mean VA calibration and Vmax. The BA calibration was significantly smaller within group 2 and RICA-LICA calibrations were significantly higher in group 2. This situation could indicate that the anterior circulation contributed to the PCA blood supply. Similarly, the posterior circulation, especially the PCAs, may have been supported from the anterior circulation in variations such as the persistent trigeminal artery. This has been reported in many cases with hypoplasia in the BA proximal segments. 11 Despite these calibration differences in the PCoA, no significant changes in VA calibration, VA FV, and velocities were observed, which may indicate that the blood in the posterior circulation was largely used in the blood supply of the posterior fossa. A decrease in the flow rate may explain vertebrobasilar ischemia and presyncope. Hong et al investigated the hemodynamic effect of fetal variant of COW and compared the control group with presyncope cases. 7 In that study, they found a decrease in FV in both VA and carotid arteries in the presyncope group. In the same study, they compared cases with typical type of COW and fetal-type COW. They reportedly found a significant decrease in VA volume, in cases with fetal type COW. However, only visual data were used in this study and PCoA calibration was not quantified. Moreover, a very small group (bilateral fetal-type Willis cases 3; unilateral fetal-type Willis cases 13) was used in the comparison. In the present study, there was no significant difference in VA flow parameters between groups divided according to PCoA calibration. Moreover, there was no significant correlation between PCoA mean calibration and VA Vmax, VA diameter, and total VA volume.
The VA FV is an important parameter to show perfusion in posterior circulation. 9 In a study by Kotil et al, they found 30 cases with right and left VA FVs at 105 and 117 mL/min, respectively. 12 In a study conducted with 844 cases, Vural et al measured the right and left VA calibrations as 3.14 ± 0.35 and 3.49 ± 0.54 mm, respectively. 13 In the same study, VA FV was measured as 119.21 and 151.45 mL/min on the right and left, respectively. Nemati et al found a mean VA FV of 119 mL/min and a peak systolic velocity of 39.92 cm/s in the group below 60 years of age. 14 Moreover, they did not find a difference between the two groups when comparing VA FV and Vmax below 60 years and older. Tarnoki et al evaluated 86 twin cases (out of total 172 cases) and studied the VA flow parameters. 15 In that study, the mean velocity of the VA was 44 ± 13.4 cm/s on the right and 40.9 ± 12.6 on the left. In the present study, VA calibrations were slightly higher than Vural’s measurements. The present study cohort’s VA volume measurements were higher than the Kotil measurements and slightly higher than the Vural measurements. When compared with the measurements of Tarnoki et al, the present cohort’s Vmax measurements were similar in the right VA and higher in the left.Compared with Nemati et al, the present cohort’s PSV measurements were higher.
The presence of intracranial collaterals, such as the COW, is a mechanism that protects the brain against infarcts. Kızılkılıç et al evaluated VA flow parameters in 120 patients with carotid stenosis. These cases were confirmed by carotid angiography. They found no difference in VA flow values between the group with carotid stenosis greater than 50% and the group with less than 50%. Moreover, 38 cases demonstrated clinical signs of VBI. They made statistical comparison between these cases and found no significant difference. As a result, their conclusion was that blood flow in the normal VAs was not affected even in the presence of ICA occlusion, in patients without collateral flow through the vertebrobasilar system, into the carotid. 16 Angiography is still the gold standard diagnostic method for demonstrating collaterals. 17 However, with new technological advances, computed tomography angiography, and MRA are now widely used for imaging the cranial vascular system. 18 Transcranial Doppler can also be used to evaluate the structure of the COW. 19
Due to the prospective and limited number of studies, VA changes in a fetal type COW or typical type of COW could not be evaluated in this study.
Conclusion
The blood supply to the brain is a very complex process. Flow reduction in any system can be compensated by other contributing vessels. The COW is an important mechanism that protects the brain against ischemia. The aim of this study was to investigate the relationship between PCoA calibration and VA flow parameters in patients below the age of 50 years, with no underlying cerebrovascular disease. However, in this cohort, no significant difference was found between VA flow parameters due to the developmental formation of PCoAs. There was no significant correlation between mean PCoA calibration and VA Vmax, VA diameter, and total VA FV. The findings, within this cohort, would suggest that the VA flow rate is relatively maintained, regardless of PCoA study measurements. Flow volume alone may not be sufficient for VA volume measurements with DS. Discovering the degree of PCoA development should be considered, in the assessment of FV.
Footnotes
Ethics Approval
This study was approved by the Institutional Review Board.
Informed Consent
Consent was obtained from all participants.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because only humans were evaluated in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Trial registration was not applied due to study type.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.