
Abstract
Objective:
The aim was to evaluate the long-term changes in systolic and diastolic functions with tissue Doppler imaging in children with sickle cell anemia.
Materials and Methods:
In this study, myocardial performance index of ventricles and mitral and tricuspid valve E/A ratios were calculated. Wall motion velocities of the interventricular septum, right and left ventricles, and mitral and tricuspid annulus were assessed during the systole (Sm), the early diastole (Em), and the late diastole (Am) with pulsed Doppler echocardiography.
Results:
These diagnostic parameters were obtained from 38 patients (mean 12.5 ± 3.2 years old) who were reached after a mean 6.7 years in long-term follow-up. Left ventricular and septal end-systolic and end-diastolic diameters, and right and left ventricular myocardial performance index were higher in patients (P < .05 and P = .001, respectively). The Em, Am, and Sm velocities of the right ventricle and septum were significantly lower in the patients at the baseline measures (P < .05) and all these velocities decreased significantly in patients over time compared with their baseline values (P < .05). In addition, it was observed that myocardial performance index values of the right and left ventricles increased significantly over time (P < .05).
Conclusion:
This is the first study reflecting the age-related changes in global systolic and diastolic functions in sickle cell anemia by serial imaging.
Sickle-cell anemia is a common inherited hemoglobinopathy caused by the substitution of adenine-to-thymine in the sixth codon of the beta globin gene, resulting in glutamic acid being replaced by valine. The abnormal hemoglobin, hemoglobin S, leads to sickling of the erythrocytes. The sickling leads to obstruction in microcirculation, tissue ischemia, chronic hemolysis, and organ dysfunction, especially in conditions such as hypoxia and infection. Cardiac involvement is a major cause of mortality and morbidity of the disease that is often assessed by conventional 2D and M-mode echocardiography. However, these imaging techniques are inadequate to demonstrate subclinical influences as well as being dependent on the patient’s preload status. Tissue Doppler imaging not only allows the evaluation of all wall movements of the ventricular myocardium throughout the heart cycle but also provides additional information about both systolic and diastolic function of the heart. 1 The myocardial performance index or the Tei-index estimated by tissue Doppler imaging is an imaging index and can be used to measure both the global systolic and diastolic functions combined. 2
Tissue Doppler imaging studies in children with sickle-cell anemia are available in the literature. However, age-related changes in cardiac systolic and diastolic function have not yet been demonstrated. The main objective of the study was to evaluate left and right ventricular function with the tissue Doppler imaging and assess the subclinical early affection of myocardium in pediatric patients with sickle-cell anemia, using the Tei index and to compare them with the healthy control group. The secondary objective was to evaluate the change in these functions with long-term echocardiography follow-up over time.
Materials and Methods
In this prospectively designed study, 56 patients (36 boys, 20 girls) with the diagnosis of sickle-cell anemia and age and sex-matched 40 healthy children (26 boys, 14 girls) were included. The control group consisted of patients who had a normal echocardiographic evaluation. The first echocardiographic evaluations of the patients were performed between February 2007 and November 2009. After 4 to 8 years (mean 6.7 years), 38 patients (22 boys, 16 girls) who were reached were evaluated with echocardiography again.
The exclusion criteria were sickle-cell crisis within the past 3 months, hemoglobin SC, and hemoglobin S-thalassemia or presence of other cardiac problems or chronic disease.
Local Ethics Committee approval was obtained for the study protocol (2.11.2016/345) and informed consent for all participations was obtained. Our study was conducted in accordance with the Declaration of Helsinki.
Echocardiography
Both the patient and control groups were evaluated by transthoracic echocardiography (Vivid S5 Pro Ultrasound System [GE Medical Systems, Horten, Norway]) by using 6 MHz transducers. All subjects underwent a complete 2D spectral Doppler and color flow Doppler examinations. Echocardiographic examinations were performed by the same experienced echocardiographer. Measures were recorded during 3 cardiac cycles and averaged to reduce the influence of respiration on myocardial velocities. The left ventricle ejection fraction was calculated by using Simpson’s biplane method. Right ventricle morphology was defined by using right ventricular end-diastolic diameter with M-mode imaging (see Figure 1A). The left atrial volume was calculated at the apical 2-chamber view (see Figure 1B). Tricuspid regurgitation jet and ventricular septal flattening were used to assess pulmonary hypertension in conventional echocardiography. Tissue Doppler velocities were obtained at the apical 4-chamber view. Sample volume was placed at the septal and lateral ages of the annulus of mitral and tricuspid valves, and medium and apical areas of the left ventricle, interventricular septum, and right ventricle. The Doppler signal quality was enhanced by lowering the Nyquist limit to 10 to 30 cm/s, using the lowest wall filter settings with minimal optimal gain, decreasing the Doppler sample volume size to 5 mm, and optimizing the sweep speed at least to 100 mm/s. Peak early diastolic (Em), peak atrial systolic (Am), and peak systolic (Sm) myocardial velocities were recorded (see Figure 2). The mitral and tricuspid inflow velocities were recorded from the apical 4-chamber view, with the pulse wave Doppler sample volume placed at the tip of its leaflets during diastole. The peak velocity during early diastole (E), peak velocity during late diastole (A), and E/A ratios were calculated for mitral and tricuspid valves (see Figure 1C and 1D).
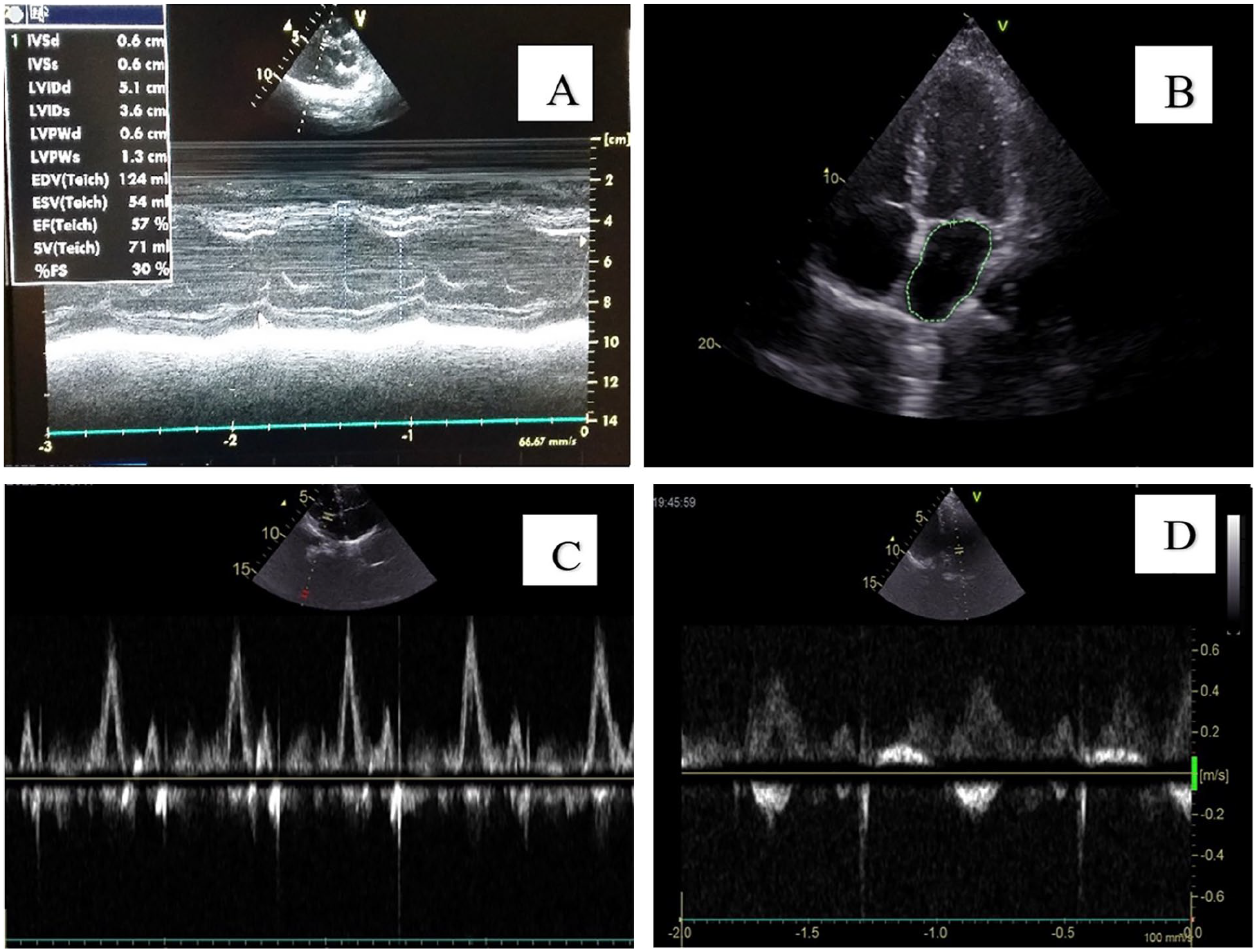
(A) M-mode echocardiographic measures of left ventricular function. (B) Left atrial volume measure. (C) Mitral inflow E and A waves. (D) Tricuspid inflow E and A waves.
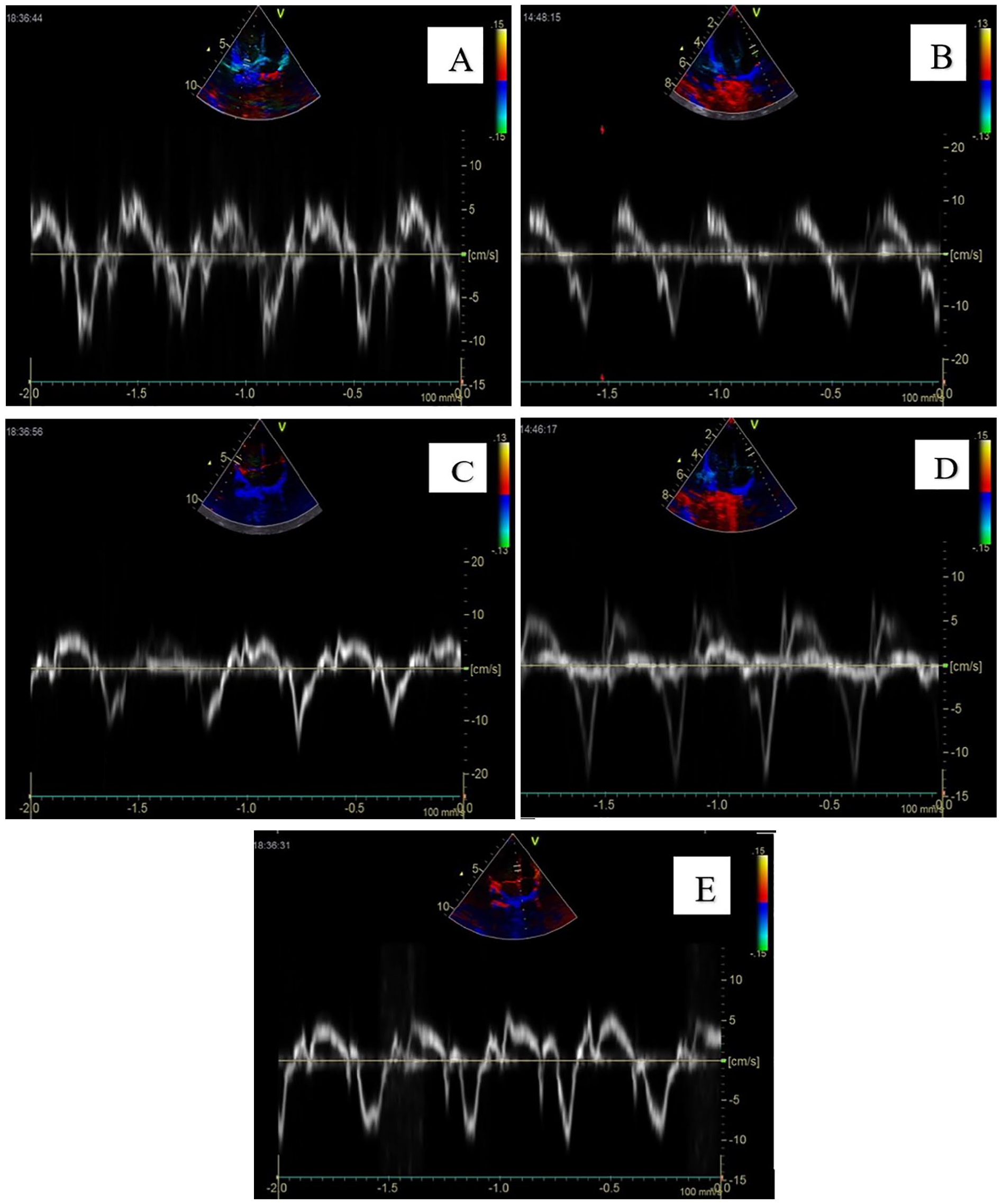
(A) The Sm, Em, and Am velocities of mitral valve annulus. (B) The Sm, Em, and Am velocities of tricuspid valve annulus. (C) The Sm, Em, and Am velocities of left ventricle. (D) The Sm, Em, and Am velocities of right ventricle. (E) The Sm, Em, and Am velocities of interventricular septum. Am, late myocardial diastolic velocity; Em, early myocardial diastolic velocity; Sm, peak systolic myocardial velocity.
The Doppler time intervals were measured from atrioventricular inflow and ventricular outflow Doppler tracings, as described by Tei. 3 The interval “a” from cessation to onset of atrioventricular inflow is equal to the sum of isovolumic contraction time, ejection time, and isovolumic relaxation time. The ejection time “b” is derived from the duration of the ventricular outflow Doppler velocity profile. The sum of isovolumic contraction time and isovolumic relaxation time was obtained by subtracting “b” from “a.” The myocardial performance index was calculated as (a – b) / b (see Figure 3).3,4 The z scores were calculated for appropriate M-mode and Doppler echocardiography parameters to standardize for age and/or body surface area.5,6
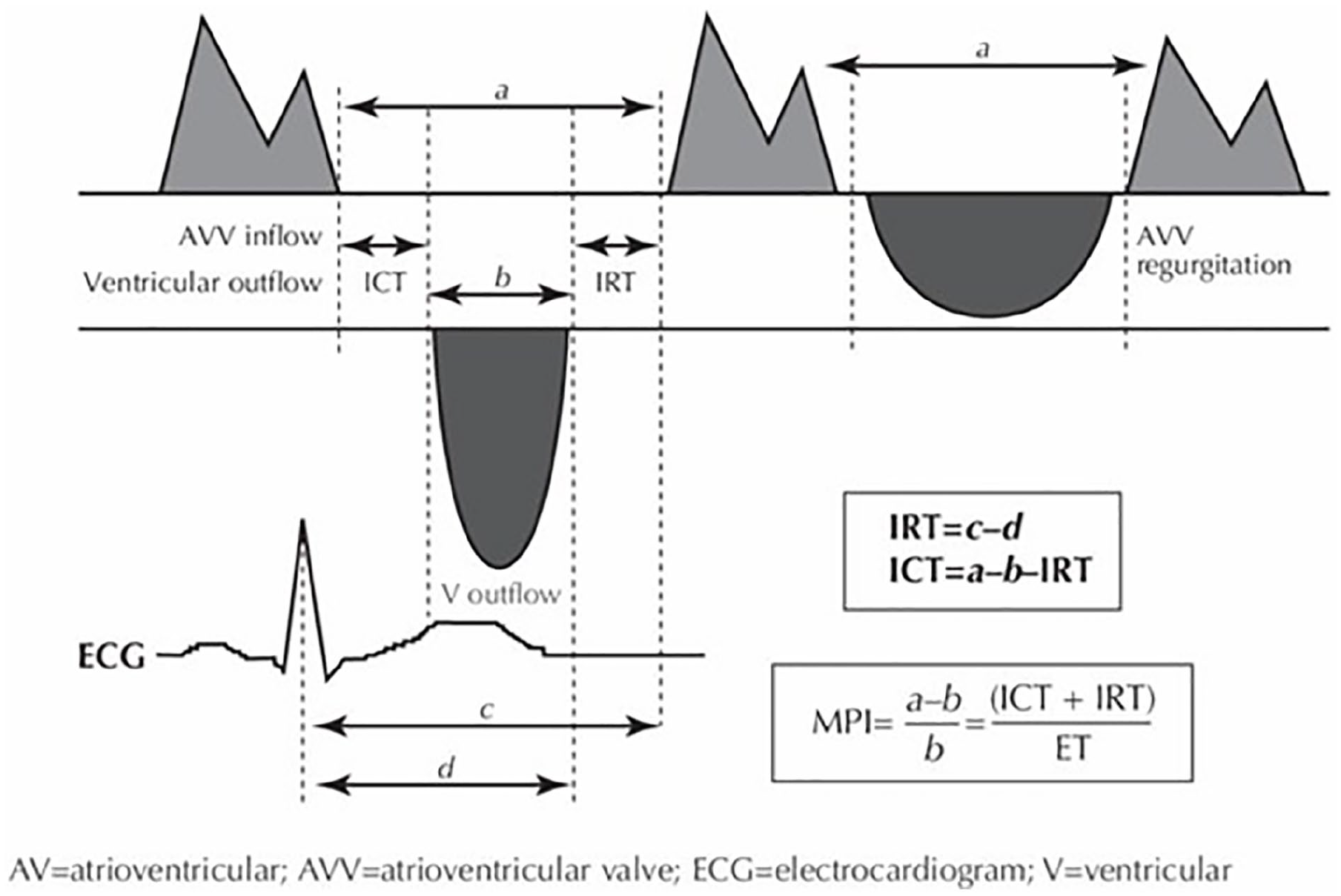
Measurement of myocardial performance index. ICT, isovolumic contraction time; IRT, isovolumic relaxation time.
Statistical Analysis
The STATA MP/11 statistical package was used for the data processing. Normality assumption for continuous echocardiographic parameters and lead values was checked by the Shapiro–Wilk test. These variables were summarized as mean ± standard deviations, and the comparisons between patient and healthy control groups were performed using an independent t test or Mann–Whitney U test. The change in velocities between the first and last examinations was analyzed using paired t test. The comparisons for categorical variables were done using the χ2 test or Fisher exact test. The statistical significance level was assessed as P < .05.
Results
The study included 56 patients with a mean age of 9.6 ± 2.4 years and 40 age and sex-matched healthy controls. The demographic data of the patient and control groups are shown in Table 1. The mean time interval between the first and last echocardiographic evaluations of the patients was 6.7 years (4–8 years), and the study was completed with 38 patients with a mean age of 12.5 ± 3.2 years.
Characteristics of Groups.
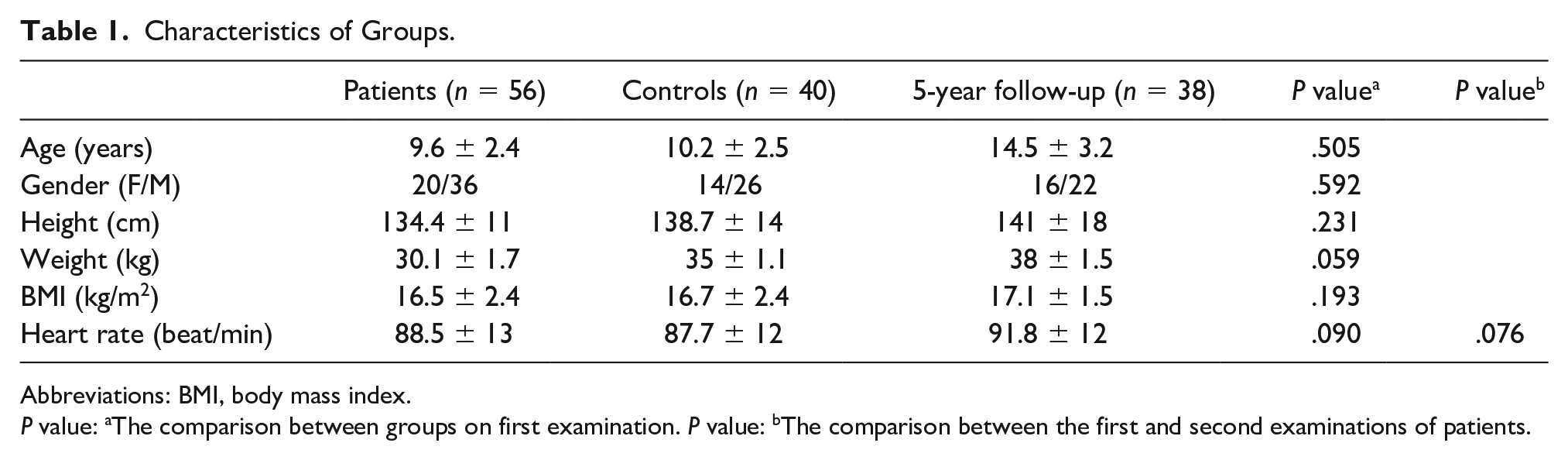
Abbreviations: BMI, body mass index.
P value: aThe comparison between groups on first examination. P value: bThe comparison between the first and second examinations of patients.
The left ventricle internal dimensions in systole and diastole (LVIDs, LVIDd), the thickness of left ventricle posterior wall in systole and diastole (LVPWs, LVPWd), the thickness of interventricular septum in systole and diastole (IVSs, IVSd), and tricuspid regurgitation jet velocities of the patient group at the first examination were significantly higher than the controls (P < .05). The LVIDd, LVPWs, LVPWd, and IVSd values in the second examination were significantly higher than those at baseline of the patients, whereas all these values were normal in range when z scores were calculated. In addition, the E velocities of mitral and tricuspid valves were significantly higher in patients (P = .002 and P = .012, respectively). However, there was not any significant change in mitral and tricuspid inflow velocity patterns of the patients in years (P > .05; Table 2).
Conventional Echocardiographic Measures of the Groups.
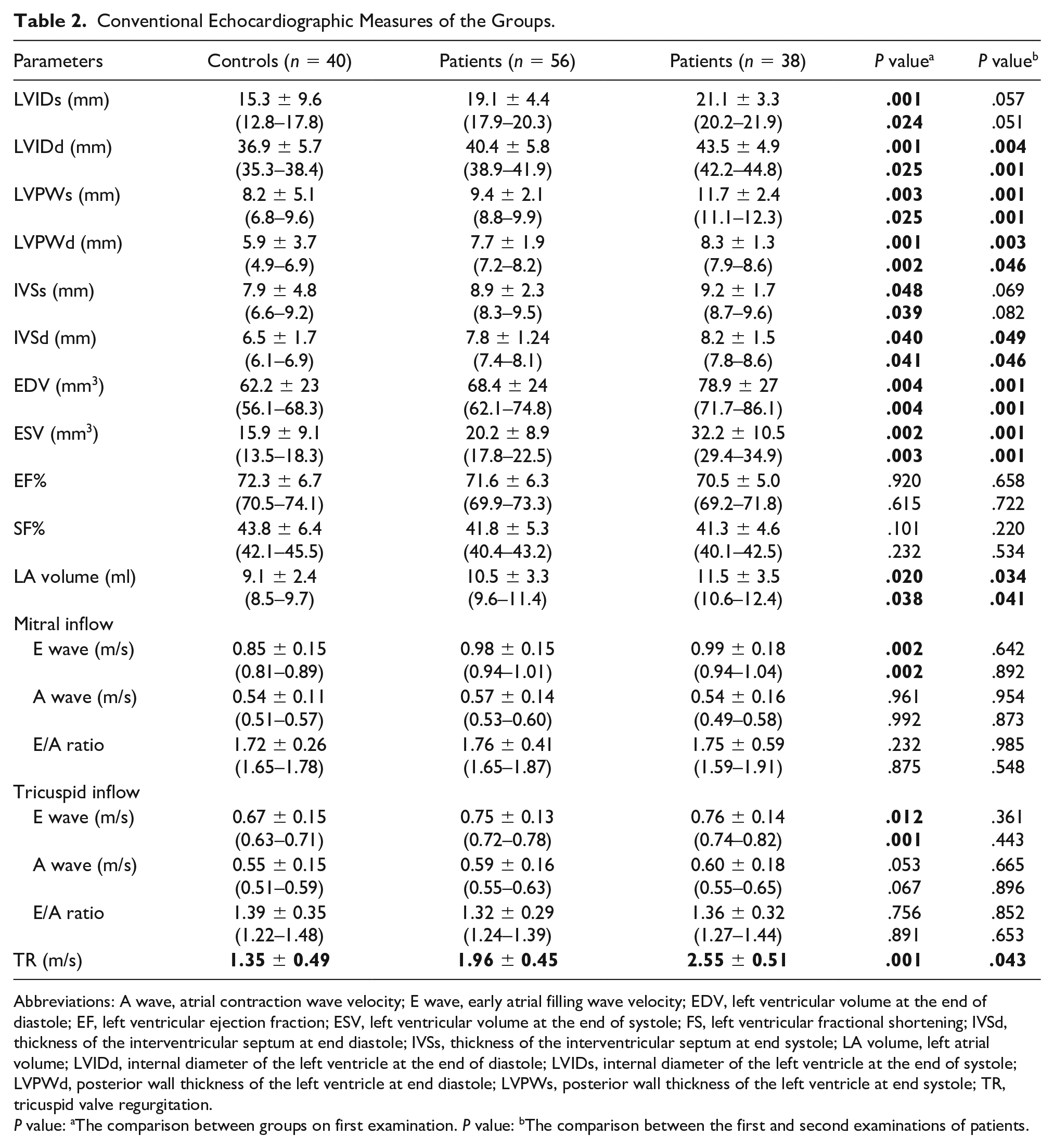
Abbreviations: A wave, atrial contraction wave velocity; E wave, early atrial filling wave velocity; EDV, left ventricular volume at the end of diastole; EF, left ventricular ejection fraction; ESV, left ventricular volume at the end of systole; FS, left ventricular fractional shortening; IVSd, thickness of the interventricular septum at end diastole; IVSs, thickness of the interventricular septum at end systole; LA volume, left atrial volume; LVIDd, internal diameter of the left ventricle at the end of diastole; LVIDs, internal diameter of the left ventricle at the end of systole; LVPWd, posterior wall thickness of the left ventricle at end diastole; LVPWs, posterior wall thickness of the left ventricle at end systole; TR, tricuspid valve regurgitation.
P value: aThe comparison between groups on first examination. P value: bThe comparison between the first and second examinations of patients.
The myocardial performance indexes of both left and right ventricles, and calculated z scores, were significantly higher in patients in the first examination and significantly increased over the years between the first and second examinations (P < .05).
The Sm and Em values of the mitral and tricuspid valves were significantly lower in the patients than in controls at baseline (P < .05). In addition, the Em velocity of the left ventricle and Sm, Em, and Am velocities of the interventricular septum and right ventricle were significantly lower in patients than in controls (P < .05).
The Sm and Em velocities of the mitral and tricuspid valves continued to decrease significantly over the years in patients (P < .05). In the comparison of patients’ changes over the years, it was observed that the Sm, Em, and Am velocities of the right ventricle and interventricular septum decreased significantly (P < .05), but a similar change was not observed in left ventricular parameters. The tissue Doppler imaging velocities are shown in Table 3.
Tissue Doppler Imaging Measures of the Groups.
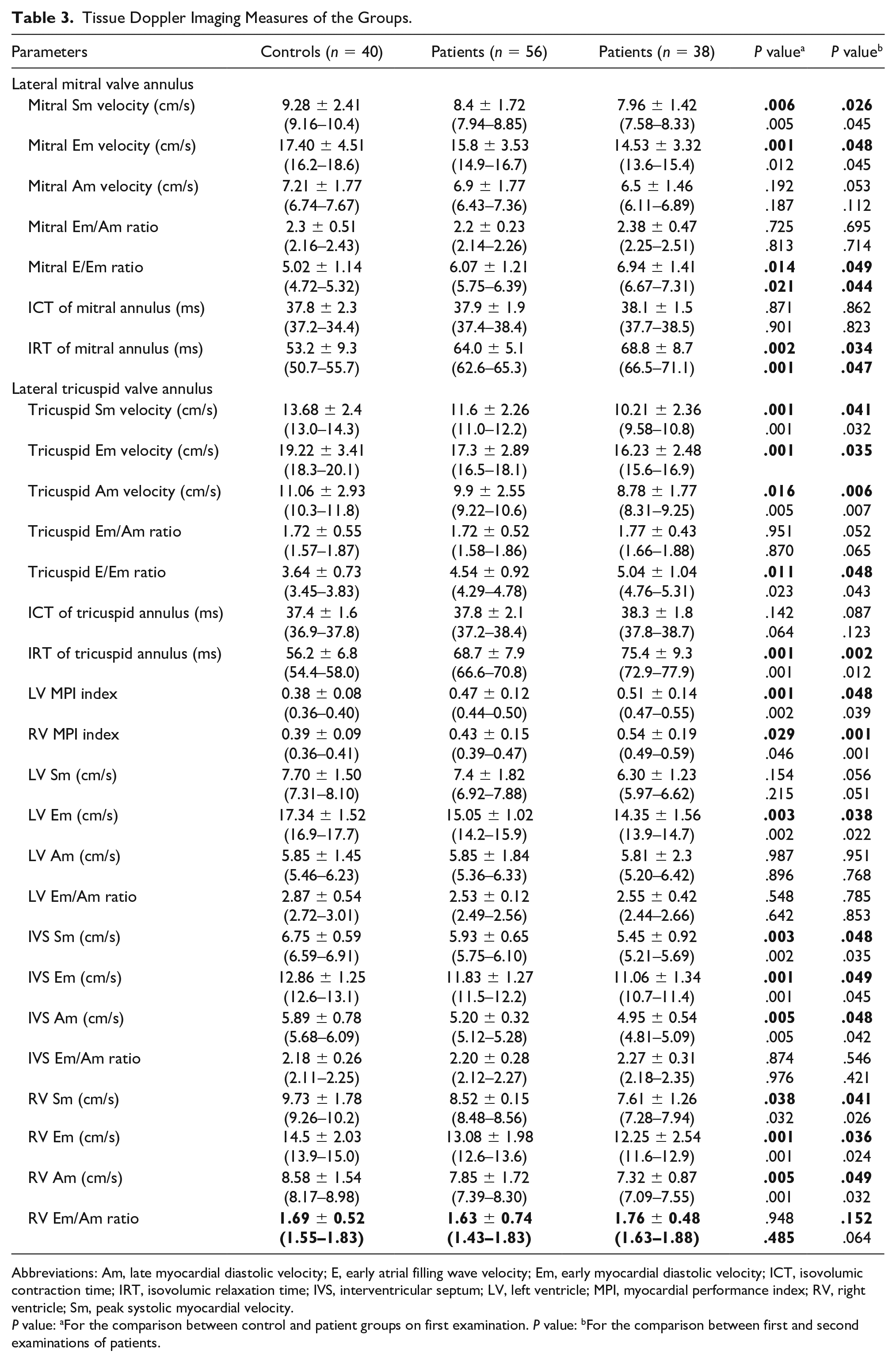
Abbreviations: Am, late myocardial diastolic velocity; E, early atrial filling wave velocity; Em, early myocardial diastolic velocity; ICT, isovolumic contraction time; IRT, isovolumic relaxation time; IVS, interventricular septum; LV, left ventricle; MPI, myocardial performance index; RV, right ventricle; Sm, peak systolic myocardial velocity.
P value: aFor the comparison between control and patient groups on first examination. P value: bFor the comparison between first and second examinations of patients.
Discussion
This is the first study in the literature evaluating the changes in cardiac functions in patients with sickle cell anemia by using serial load-independent echocardiography parameters over the years. In this study, it was observed that systolic and diastolic thickness of left ventricle and interventricular septum and myocardial performance indexes of both ventricles increased over time, while the Sm, Em, and Am velocities of the right ventricle and interventricular septum decreased.
Chronic hemolysis and associated endothelial dysfunction are the mainstays of clinical presentation of sickle cell anemia. In addition, chronic anemia is responsible for the early cardiac effects of the disease. An increase in resting heart rate and stroke volume is necessary to tolerate chronic anemia and to provide tissue oxygenation and cardiac output. This developing compensatory mechanism also causes dilatation of the heart and left ventricular hypertrophy. It is thought that diastolic dysfunction and pulmonary hypertension may develop in early childhood, while systolic dysfunction may develop in the late period of the disease.7–9 In addition, iron deposition hurts cardiac contractility as repeated transfusions are needed. All these cardiac effects are more evident in adulthood, but it may not be easy to recognize heart failure in the pediatric population, especially in patients with low transfusion needs and mild anemia. Therefore, recording changes in serial echocardiographic follow-up allows early detection of cardiac dysfunction. Conventional echocardiographic parameters of healthy controls and patients with sickle cell anemia have been compared several times. AboHadeed et al. studied left and right ventricular systolic and diastolic functions and did not show a difference in systolic and diastolic diameters of the ventricles, fractional shortening, and corrected ejection time between patients and controls. 10 Conversely, Eddine et al. revealed that left ventricular dimension and mass increased in patients with sickle-cell anemia, but ejection fraction and fractional shortening of the left ventricle were normal. In addition, they added that progressive left ventricular dilation and hypertrophy were associated with worsening anemia. 11 Caldas et al. evaluated 107 children with sickle cell disease by comparing them with 70 healthy children and reported that all M-mode measurements of the patients, including systolic and diastolic dimensions, ejection fraction, and fractional shortening of the left ventricle, were statistically higher than those of the controls. 12 In some studies, the left ventricular diastolic diameter was evaluated as a predictor of increased mortality in adults with sickle cell disease, independent of advanced age, the severity of anemia, high body mass index, and high blood pressure.8,13 In our study, while ejection fraction and fractional shortening of the left ventricle were similar in patients and controls, left ventricular systolic and diastolic diameters were significantly increased in patients. In the initial evaluation, it was known that the annual need for transfusion and the frequency of painful crises were less than 5 per year in most patients, and none of the patients had severe anemia with hemoglobin levels <7 g/dL. It was thought that the similarity of ejection fraction and fractional shortening with the control group, despite the increase in systolic and diastolic parameters of the patients, might be due to the absence of severe clinical disease in our study group.
Similarly, in this study, the second echocardiographic evaluation, within a mean of 6.7 years, showed that there was a significant increase in diastolic diameters of the left ventricle and interventricular septum, while the increase in systolic diameters was not significant. This result suggests that subclinical influences primarily affect diastolic functions due to chronic volume overload, but that systolic dysfunction may become more evident over time. In addition, the abnormal measurements of diastolic function obtained in this study and its continued deterioration over time in patients with sickle cell anemia, even if their clinical disease is mild, is an important contribution to the literature.
The left atrial volume, which is one of the important findings of left ventricular diastolic dysfunction, was significantly increased in the patient group in accordance with the literature. 10 The mean heart rate of the patients was not different from the control group, and there was no significant increase in the follow-up examinations. This result was thought to be due to the absence of patients with severe anemia in the study.
The tricuspid valve regurgitation jet of the patient group was also evaluated and, although no significant insufficiency was detected above 1.96 ± 0.45 m/s, it was statistically higher when compared with the control group and was observed to increase significantly in patients over time. Gladwin et al. suggested that the noninvasive measurement of tricuspid regurgitation jet velocity by echocardiography could be used to identify patients at high risk for death. 14 The results obtained in this study may indicate that the changes in the pulmonary vascular bed, which lead to the development of pulmonary hypertension, begin even in the early period of the disease. It can also be considered because of the presence of right ventricular dysfunction, which develops over time as the natural course of the disease. The fact that tricuspid insufficiency was found to be slightly increased in the patient group in our study supports the conclusion that the risk of death in patients with sickle-cell anemia may be higher than in the normal population. In addition, the increasing gradient of tricuspid valve regurgitation in patients over time indicates that many patients have a suspicion of pulmonary hypertension. This result, which shows that the duration of exposure to sickle cell disease with age leads to progressive cardiac dysfunction and also leads to pulmonary hypertension is consistent with the literature.15,16
The myocardial performance index is a combined measure of systolic and diastolic function, and the higher myocardial performance index values represent the reduced biventricular myocardial function. The myocardial performance index is minimally affected by heart rate, preload, and afterload. Chronic volume overload, iron deposition, and endothelial dysfunction lead to decreased myocardial contractility and increased stiffness of the myocardium. As a result of ventricular dysfunction, isovolumic contraction time and isovolumic relaxation time are prolonged, and ejection time is shortened and myocardial performance index value increases. In previous studies, both the right and left ventricular myocardial performance indexes were found significantly higher in pediatric patients with sickle-cell anemia when compared with controls.10,12,17–19 Similarly, in this study, both the left ventricle and right ventricle tissue Doppler imaging-derived myocardial performance index were found significantly higher in children with sickle-cell anemia than in controls. Moreover, it was shown, for the first time, that the increase continued over time when compared with the baseline values of the patients. In this study, the mean isovolumic relaxation time was found significantly higher than in controls, which causes an increase in myocardial performance indices of the right and left ventricles in patients with sickle-cell anemia and both continued to increase in follow-up in patients. The results of this study supported that the onset of ventricular dysfunction in patients with sickle-cell anemia starts early in childhood and continues with age, which might be a significant determinant of the clinical outcome in these patients.
AboHadeed et al. demonstrated a significant decrease in Sm velocities of mitral and tricuspid valves, showing systolic dysfunction in the left and right ventricles. In addition, they reported that the Em and Am velocities of mitral and tricuspid valves, indicating diastolic dysfunction of left and right ventricles, decreased. Furthermore, they showed a significantly reduced Em/Am ratio and a higher left ventricle E/Em ratio in patients with sickle-cell anemia. 10 In this study, the Sm and Em velocities of the lateral mitral valve annulus and Sm, Em, and Am velocities of lateral tricuspid valve annulus were significantly lower in patients and continued to decrease over time. This decrease can be interpreted as both ventricles showing systolic and diastolic dysfunction in the patients with sickle-cell anemia. Moreover, all the Sm, Em, and Am velocities of the lateral wall of the right ventricle significantly decreased in patients and continued to decrease over time, while only the Em velocity of the lateral wall of the left ventricle decreased. This result not only demonstrated diastolic impairment starting earlier than systolic dysfunction but also right ventricular dysfunction starting earlier than left ventricular dysfunction. The results of these patients did not demonstrate any difference in Em/Am ratios of the ventricles and lateral mitral and tricuspid annulus between the first and second examinations of the patients. Early atrial filling wave velocities of mitral and tricuspid valves were higher in patients. However, the difference in E/A ratios for both the mitral and tricuspid valves was not significant between patients and controls, as well as between the first and second examinations of the patients. Bahl et al. explained these results that chronic severe anemia leads to a hyperdynamic state with improved left ventricle function and decreased peripheral resistance. They added that chronic severe anemia alone did not lead to ventricular dysfunction in patients without other underlying cardiac or systemic diseases. 20
The E/Em ratio is an index for evaluating diastolic functions of the ventricles. Sachdev et al showed that an increase in the left ventricular lateral E/Em ratio was associated with functional impairment, as assessed by the 6-minute walk test. 13 An average ratio ≤8 identifies patients with normal ventricular filling pressures, whereas a ratio ≥13 indicates an increase in filling pressures. 21 In this study, both mitral and tricuspid E/Em ratios were found to be <8, indicating the normal biventricular filling pressures. However, the ratios were significantly higher in the patients’ group and continued to increase over time, thought to be a consequence of subclinical diastolic dysfunction of both ventricles.
Limitations
The main limitation of the study was that the patients were not grouped according to their hemoglobin levels. Cardiac effects of iron overload could not be evaluated clearly due to the lack of patients with severe anemia and with the frequent need for transfusions. The other important limitation was that the patients had mild pulmonary hypertension, and the results may be inapplicable to patients with severe pulmonary hypertension. In addition, evaluating the changes in cardiac functions of the same patient group over the years with cardiac magnetic resonance imaging and comparing them with tissue Doppler echocardiography results could increase the reliability of the study. Another limitation of this study was that it was a longitudinal study with a pediatric population, where dimensions should normally increase with age.
Conclusion
Myocardial performance index and tissue Doppler techniques are effective and noninvasive methods to evaluate early hemodynamic impairment and global systolic and diastolic functions in patients with sickle-cell anemia. The most important point worth mentioning in this study was that the changes in longitudinal follow-up, not cross-sectional, were revealed in patients with sickle cell disease in the pediatric age group. We demonstrated that tissue Doppler imaging measures have prognostic value in detecting early cardiac dysfunction in long-term follow-up of children with sickle-cell anemia. Finally, we would like to mention that adding the longitudinal strain of the myocardial function in sickle cell patients compared with controls may be a potential valuable next step for further evaluation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from Mersin Üniversitesi Institutional Ethics Committee; 2016/257.
Informed Consent
Informed consent was not sought for this study because all case data were de-identified and/or aggregated and followed ethics committee or institutional review board (IRB) guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used to conduct this study.
Trial Registration
Not applicable.