
Abstract
The aim was to collect cases of cesarean scar pregnancy (CSP) and describe the evolution of diagnosis, treatment modalities, and outcome. A retrospective cohort study was conducted of patients who had been diagnosed with CSP. Treatment decision was made according to the type of CSP, levels of beta human chorionic gonadotropin (hCG), and estimated vascularity. Forty cases with CSP were recorded. Overall success of the primary treatment was recorded among 30 of 40 cases (75%) and significantly correlated with degree of vascularity, type of CSP, and beta hCG levels. The treatment methods included serial methotrexate in 20 cases; 15 of them (75%) were successful. In this specific group, we found type 2 scar and high vascularity to be significantly associated with treatment failure. In conclusion, cases with type 2 CSP, high vascularity, and high beta hCG levels should be considered high risk, and extra caution should be taken in choosing treatment modality and follow-up.
A cesarean scar pregnancy (CSP) is a relatively rare form of ectopic pregnancy that may lead to life-threatening complications if diagnosis and treatment are delayed.1,2 The first case was described in 1978 by Larsen and Solomon. 3 In recent years, there has been an increase in CSP incidence due to the increase in the number of cesarean section deliveries and improved diagnosis with sonography. The estimated incidence ranges from 1 in 1800 to 1 in 2216 pregnancies, with a rate of 6.1% of all ectopic pregnancies in women with a history of cesarean section. 4 Two types of CSP have been defined using sonography: type I (endogenic type) progression of CSP toward the uterine cavity and type II (exogenic type) deep invasion in the scar defect and progression toward the bladder with possible protrusion into the abdominal cavity. 4
CSP can cause catastrophic complications such as uterine rupture with severe life-threatening bleeding, which may lead to hysterectomy. 5 Early diagnosis is essential for the success of conservative treatment, prevention of complications, and the preservation of fertility. The diagnosis is usually made by transvaginal sonography, showing the presence of a gestational sac at the site of the previous cesarean scar and an empty uterine cavity. Other possible sonographic findings include presence of trophoblast between the bladder and the anterior uterine wall, bulging of the sac beyond the anterior uterine wall,6–8 absence of myometrium between the gestational sac, and the bladder with discontinuity of the anterior uterine wall in the sagittal plane.9,10 Doppler abnormalities are also possible, including evidence of perfusion of the peritrophoblastic vasculature. 9
The optimal treatment for a CSP is unclear, and therapy should be tailored according to the patients’ clinical and sonographic presentation, beta human chorionic gonadotropin (hCG) levels, and the surgeon’s experience. Traditionally, treatment of a stable patient included dilatation and curettage 11 or methotrexate (MTX) given by direct sac injection12,13 or systemically. 14 More recent treatment options include Foley catheter insertion into the uterine cavity to create a pressure effect, 15 uterine artery embolization by angiography, 12 hysteroscopy to remove remaining pregnancy and stop bleeding, 16 laparoscopy to inject locally 100 mg etoposide under transvaginal ultrasound assistance,17,18 or combined methods. 19
In the case of uterine rupture or major bleeding, surgery is unavoidable and may include hysterectomy. In subsequent pregnancies, recurrent scar implantation may occur. 20 There are reports of successful term pregnancy after a cesarean scar pregnancy 20 ; however, uterine rupture (resulting in maternal or fetal death) and placenta accreta have also been reported. 21
The objective of this study was to describe the evolution of diagnosis, treatment modalities, and outcome (including subsequent pregnancies) over 10 years of practice experience.
Materials and Methods
A retrospective cohort study of patients was conducted to isolate patients who had been diagnosed with CSP during 2006 to 2016. In addition, these patients were treated and followed at the gynecologic department with sonography. After receiving approval of the Ethical Review Committee, patient data were collected from the hospital’s medical records and the electronic charting system.
Analysis consisted of the following clinical and demographic data, including age at diagnosis, number of previous pregnancies and previous caesarean deliveries, gestational age at diagnosis, treatment modality, treatment results, complications (heavy bleeding, pain, need for blood transfusion, and need for hysterectomy), second-line treatment if needed, beta hCG level at diagnosis and time until resolution, and subsequent pregnancy occurrence. Sonographic data included largest diameter of gestational sac, presence of heartbeat, type of CSP (type I or type II), vascularity, and thickness of myometrium between pregnancy and serosa.
Criteria for the diagnosis of CSP included the following4,11,22,23: (1) an empty uterine cavity; (2) a closed and empty cervical canal; (3) a gestational sac showing the “double decidual sign” with or without cardiac activity located anteriorly at the level of the internal os; (4) a mixed mass or a clear gestational sac embedded at the lower uterine segment, within the myometrium and the fibrous tissue of the previous cesarean section scar, and separated from the endometrial cavity or fallopian tube; (5) a thin or absent myometrial layer between the gestational sac and the bladder; (6) the presence of increased peritrophoblastic or periplacental vascularity around the location of previous cesarean section scar on color Doppler examination; and (7) negative “sliding sac sign,” which refers to the gestational sac’s position not being changed by gentle pressure applied by the transvaginal probe. CSP was formally diagnosed on an individual case basis when sonographic images contained one or more of the abovementioned criteria. All sonographic examinations were completed by the same two physicians with a subspecialty in advanced gynecologic sonography.
Vascularity of the CSP was determined according to the criteria previously published by the International Ovarian Tumor Analysis (IOTA) in which a score of 1 is given when no blood flow is found in a lesion, a score of 2 when only minimal blood flow can be detected (Figure 1), and a score of 3 when moderate to increased blood flow is present (Figure 2). 24 Treatment decision was according to the type of CSP, the levels of beta hCG, and the estimated vascularity of the CSP: in type I CSP with beta hCG levels below 10,000 and low to medium vascularity, dilatation and evacuation (D&E) or single MTX intramuscular injection was preferred. In type II CSP with medium to high vascularity and beta hCG levels above 10,000, serial intramuscular MTX injection (with alternate folinic acid) or MTX injection into the gestational sac was preferred as first-line treatment. A Foley catheter was used in cases of type II CSP with medium to high vascularity and elevated beta hCG. In mild cases in which treatment was either single MTX or D&E, patients were discharged home the following day and followed weekly thereafter using sonography and beta hCG until resolution. In medium- to high-vascularity cases (in which serial MTX was given or injected into the sac), patients were admitted to the gynecologic ward and daily beta hCG and sonography was performed. A successful treatment was defined as resolution of the pregnancy sonographically and also chemically. In cases of failure of the primary first-line treatment according to sonographic parameters or beta hCG levels, a similar treatment modality was repeated or a new one was initiated.
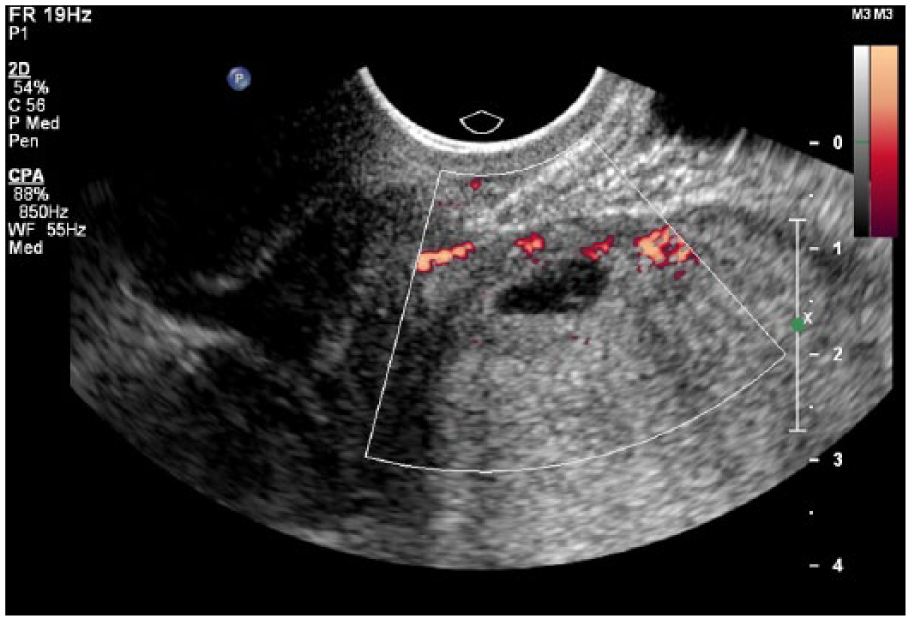
Moderate vascularity showing minimal blood flow gestational sac.
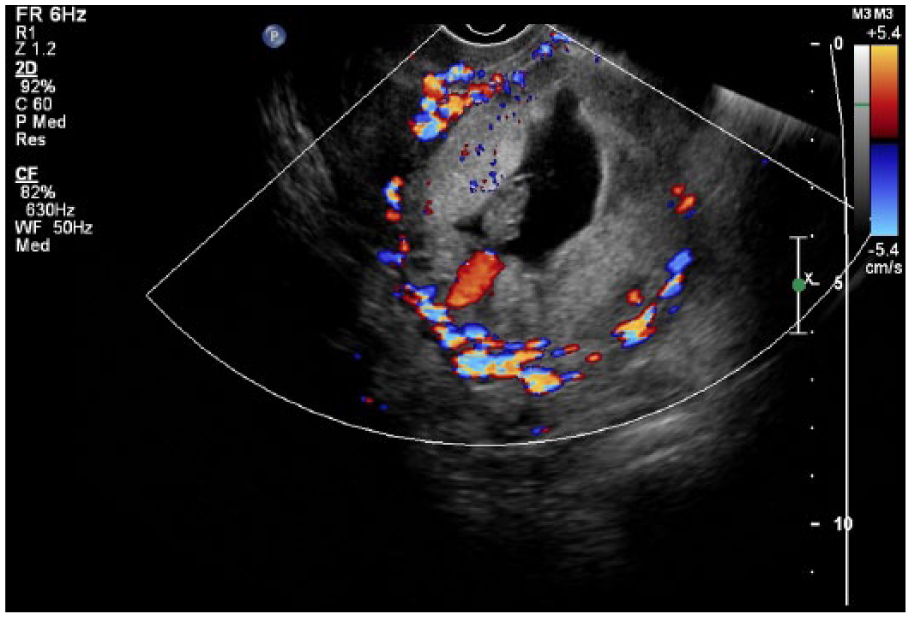
High vascularity when moderate to increased blood flow is present.
Statistics
Data analysis was performed using the SPSS statistical package version 18 (SPSS, Inc., an IBM Company, Chicago, IL). All statistical tests were two-sided, and a P value of <.05 was considered significant. Data for categorical variables are presented by the number of patients identified and by percent. For continuous variables, mean ± standard deviation (SD) are presented. To assess the association between categorical variables and outcome of treatment, chi-square test was used, and for continuous variables, the Mann-Whitney test was used. Multivariate analysis was used to assess the statistical significance of all covariates that were significantly associated with the success of primary treatment (including heartbeat, vascularity, type of scar pregnancy, and beta hCG levels).
Results
During the period, 40 cases of CSP were identified, 3 of which were recurrences. Mean age at diagnosis was 34.3 (range, 24–40) years, 26 (65%) had one previous scar, 13 patients (32.5%) had two previous scars, and 1 (2.5%) had three previous scars. Mean gestational age at diagnosis was 6 weeks 3 days. Mean gestational sac diameter on the longest diameter was 25 mm (range, 7–60 mm). Available and measurable crown rump length (CRL) was in 20 cases, and mean CRL was 8.8 mm (range, 3–18 mm). Fetal heartbeat was seen in 10 cases. Thirty cases (75%) were type I CSP (Figure 3) and 10 cases (25%) were type II (Figure 4). Vascularity was defined high in 10 cases (25%), medium in 10 cases (25%), and low in 20 cases (50%). Mean (SD) beta hCG levels at presentation were 21,970.3 (27,841.7) mg/dL (range, 230–118,000 mg/dL), and median levels were 9300 mg/dL (Table 1). Mean (SD) beta hCG levels at presentation among cases with positive heartbeat were 47,450.3 (23,786.3) mg/dL (range, 230–118,000 mg/dL) and 12,160.3 (6738.3) mg/dL (range, 1130–30,513 mg/dL) among cases with no heartbeat (P < .0001). Mean (SD) beta hCG levels among cases with high vascularity were 56,214.7 (32,456.5) mg/dL (range, 5200–118,000 mg/dL) compared to 13,890.6 (9541.7) mg/dL (range, 530–30,513 mg/dL) among cases with medium vascularity and 8593.7 (5629.6) mg/dL (range, 230–27,000 mg/dL) among cases with low vascularity (P < .005).
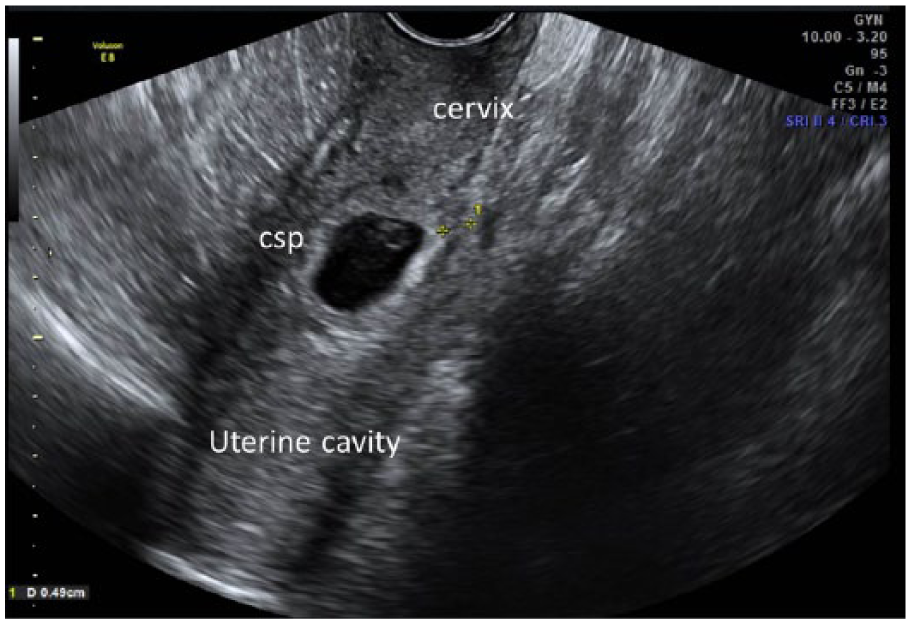
Type I cesarean scar pregnancy (csp) with progression of pregnancy sac toward the uterine cavity.
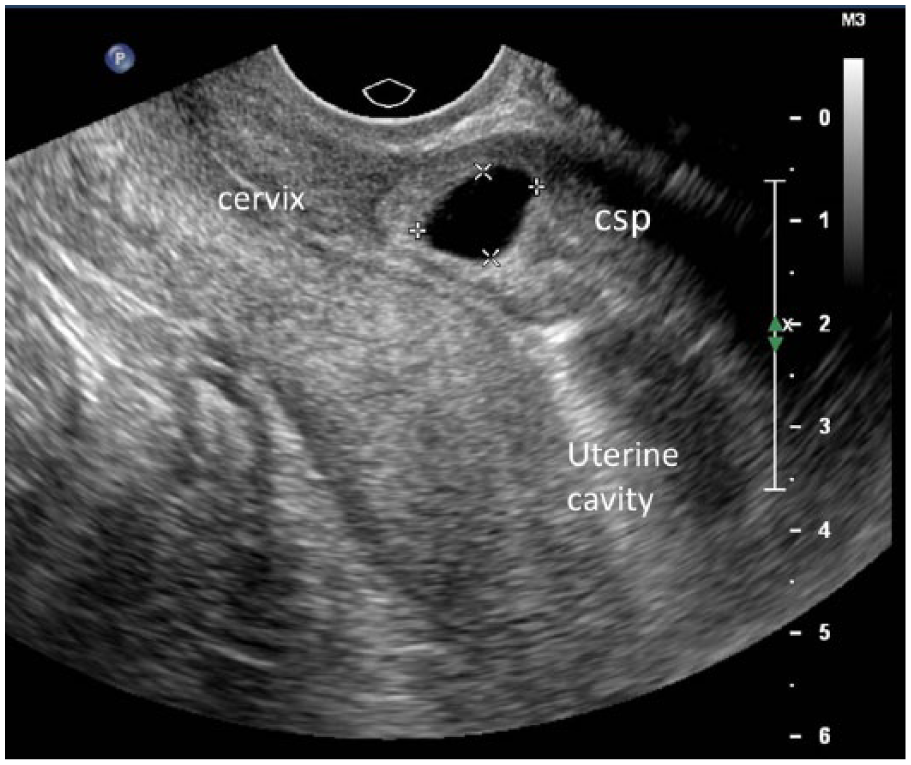
Type II cesarean scar pregnancy (csp) (exogenic type) with deep invasion in the scar defect and progression toward the uterine serosa.
Clinical Data on Cases.
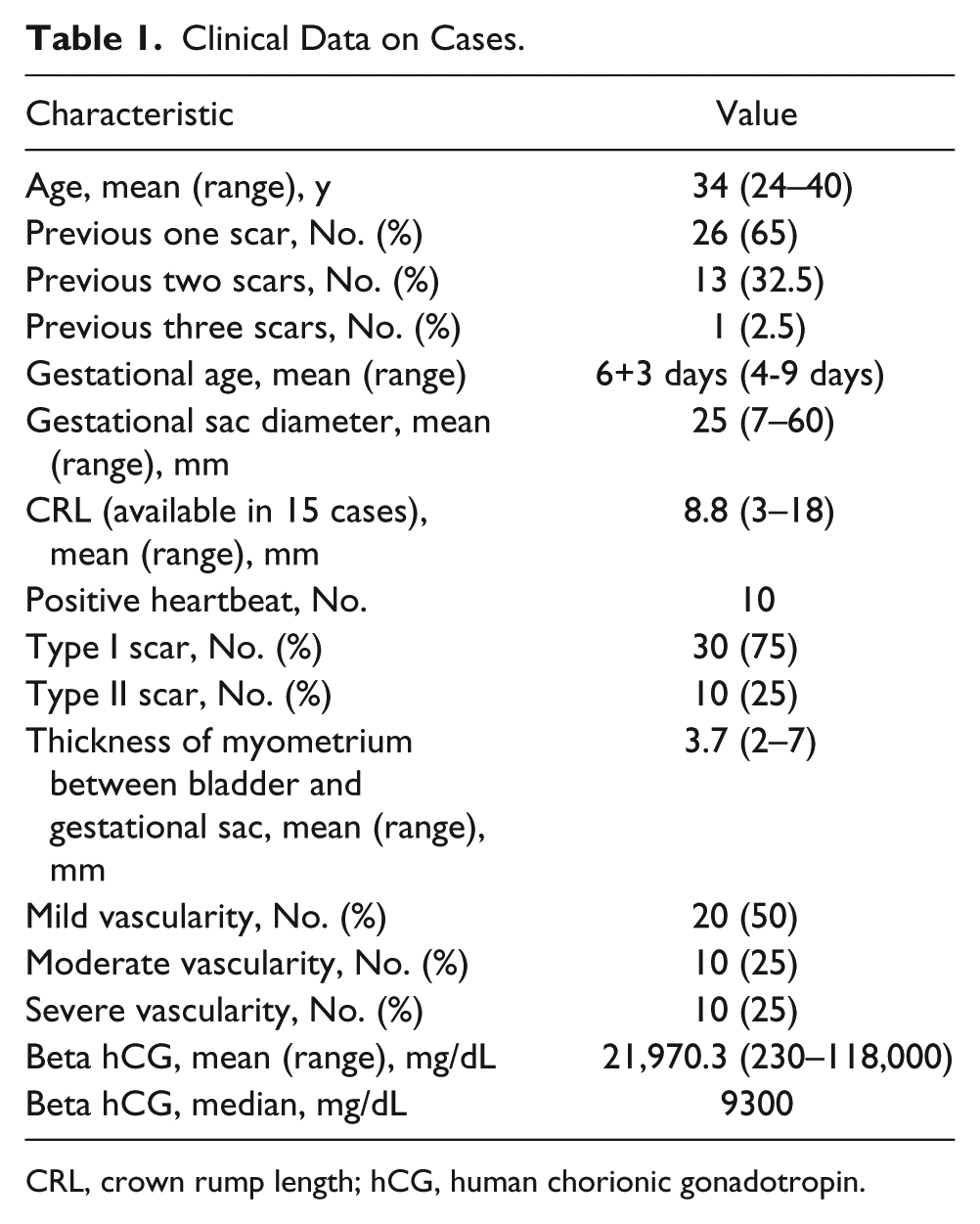
CRL, crown rump length; hCG, human chorionic gonadotropin.
Overall primary treatment success was recorded among 30 of 40 cases (75%). It significantly correlated with the degree of vascularity. Among 10 cases with high vascularity, treatment was successful in 5 (50%). The rate of successful treatment among medium vascularity was 60% and 90% among low-vascularity cases (P < .015) (Figure 5). Odds ratio (OR) for failure of primary treatment was 20 in high vascularity compared to low vascularity (OR = 20; 95% confidence interval [CI], 1.8–222.7; P < .015). Type of CSP was also significantly associated with successful primary treatment: type II had 60% failure rates compared to 20% among type I cesarean scar (OR = 7.3; 95% CI, 1.3–41.3; P < .024). Mean (SD) time to beta hCG resolution after primary treatment was 56 (33.6) days (range, 5–120 days). Levels of beta hCG were negatively associated with successful primary treatment. We found the cutoff of 9300 mg/dL to be most predictive of failure of primary treatment with an OR of 7.5 (95% CI, 1.3–43.3; P < .023). The levels of beta hCG, rate of failed treatment, and rate of complications were all significantly higher among cases with high vascularity.
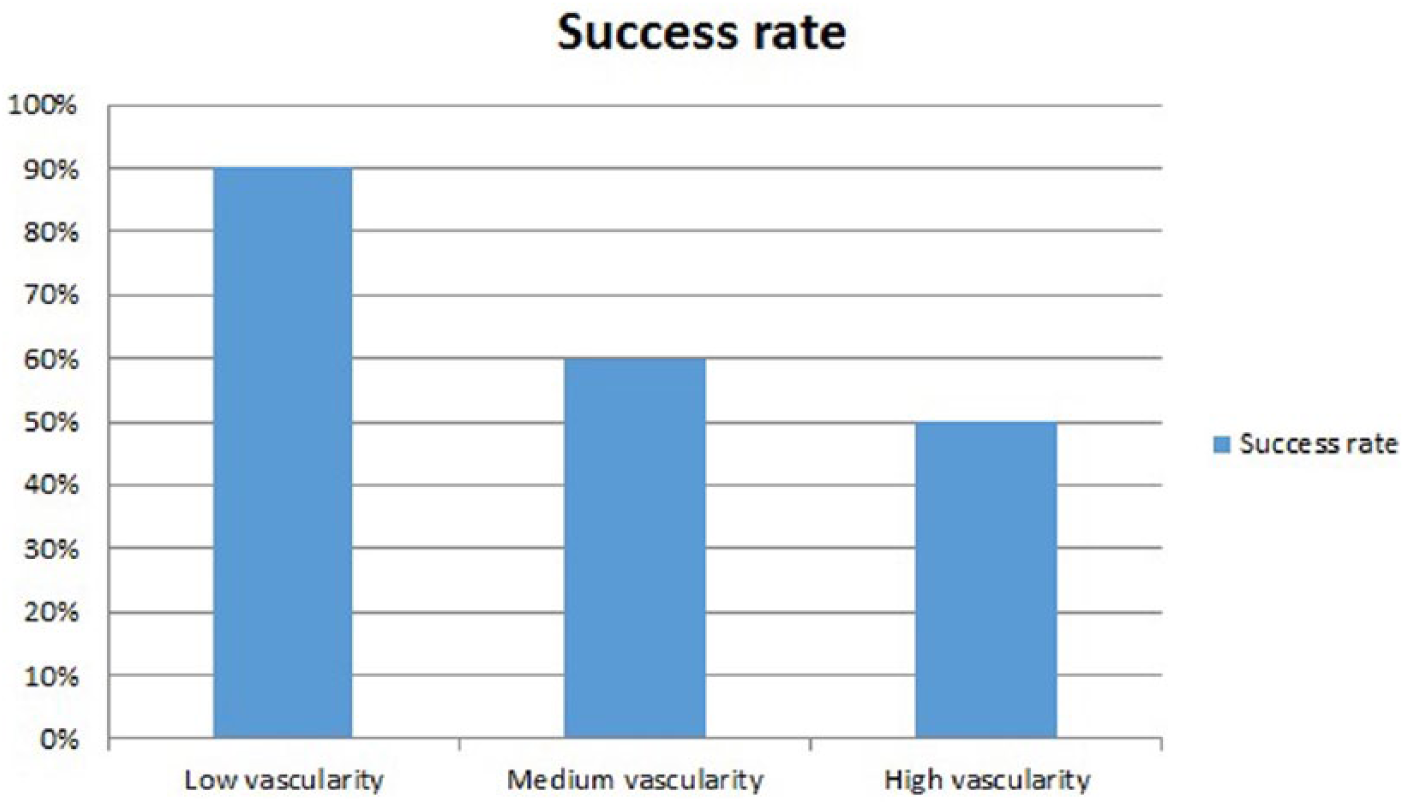
Rates of treatment success according to level of vascularity.
Multivariate analysis using presence of heartbeat, vascularity, type of scar pregnancy, and beta hCG levels, with relations to primary treatment success, found type of CSP and levels of beta hCG above 9300 mg/dL as significant and independent factors associated with failure of primary treatment.
The treatment’s methods and results of the aforementioned cases included serial MTX in 20 cases, with 15 of them (75%) successful. Median beta hCG level among those cases was 12,450 mg/dL (range, 2500–118,000 mg/dL), heartbeat was positive among 4 (20%) cases, and vascularity was low in 10 cases (50%), moderate in 4 (20%), and high in 6 (30%). Five cases were defined as type II scar and 15 as type I. A correlation was calculated between successful primary treatment in this group and presence of heartbeat, type of scar, type of vascularity, and levels of beta hCG and found type II scar (60% failure rate compared to 13% failure rate among type I [P < .05]) and high vascularity (33% failure rate compared to no failure among low vascularity [P < .0032]) to be significantly associated with failure of primary treatment. Single MTX was used in four cases, and all were successful. MTX injection into the gestational sac was performed in six cases, two of which had fetal heartbeat, and was successful in four of them (66%)) one failure with positive heartbeat). Dilatation and evacuation was used in seven cases (71% success rate) and Foley catheter in three cases (success in two cases). Median levels of beta hCG, type of vascularity, type of CSP, and presence of heartbeat in each treatment group are presented in Table 2.
Data According to Treatment Modality. a
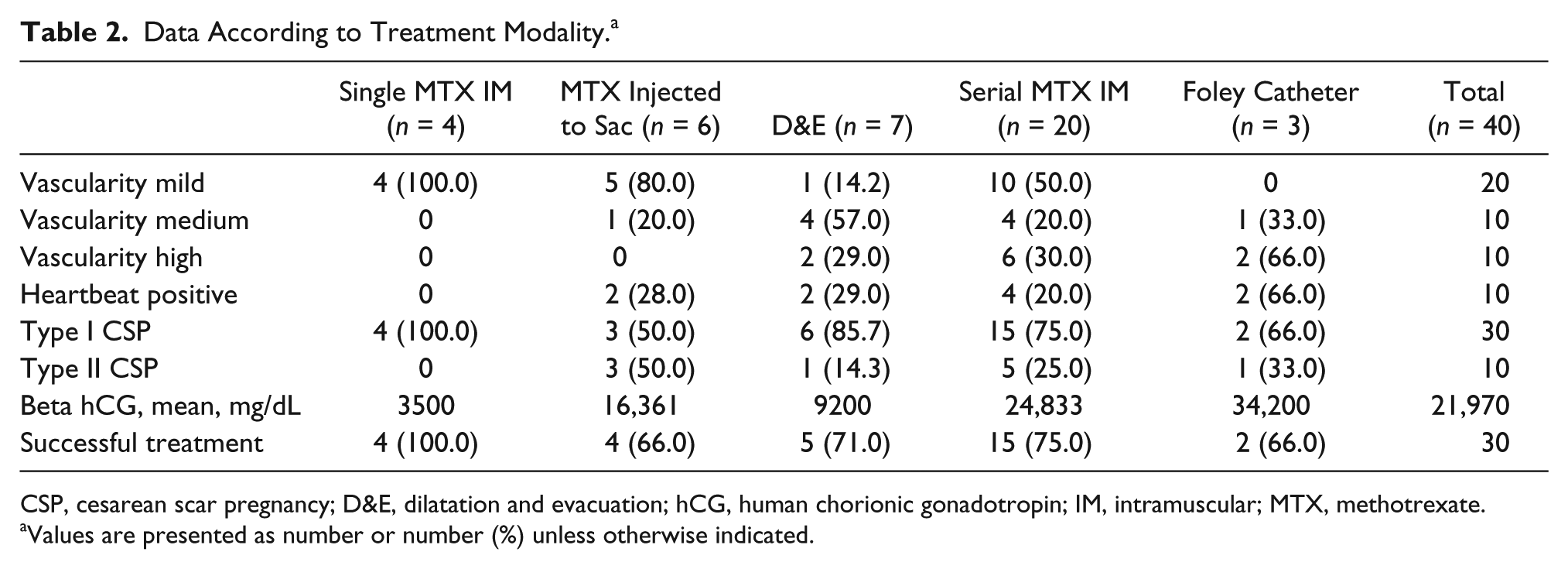
CSP, cesarean scar pregnancy; D&E, dilatation and evacuation; hCG, human chorionic gonadotropin; IM, intramuscular; MTX, methotrexate.
Values are presented as number or number (%) unless otherwise indicated.
Complications were recorded in three cases (7.5%) and included heavy bleeding with need for blood transfusion in two cases. These cases are described in Table 3.
Cases With Complications.
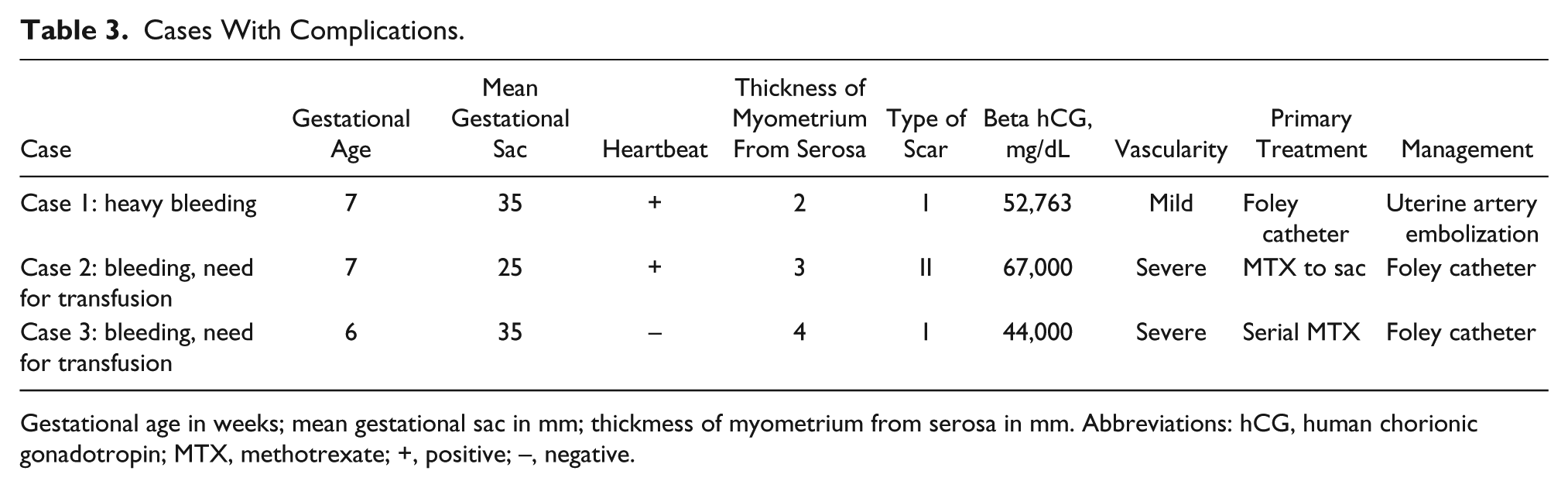
Gestational age in weeks; mean gestational sac in mm; thickmess of myometrium from serosa in mm. Abbreviations: hCG, human chorionic gonadotropin; MTX, methotrexate; +, positive; –, negative.
Fourteen patients achieved subsequent pregnancy; in three of them, CSP recurred. Eleven patients had an uneventful pregnancy, which was not complicated by morbidly adhesive placenta. Three recurrent CSPs were successfully treated as reported earlier.
Discussion
In this retrospective cohort study, 40 cases of CSP were evaluated. Cesarean scar pregnancy was found to have a successful treatment rate of 60% to 75%, with primary treatment being successful in 75% of the cases. Several factors seem to affect the success and the complications rates: beta hCG level, type of CSP, and the vascularity of the pregnancy assessed with Doppler waveforms. A worse prognosis was related to higher beta hCG levels, type II CSP, and severe vascularity.
Results of the study may suggest that the timing of the diagnosis is important for a better prognosis. The most prevalent symptom in CSP is vaginal bleeding, but most patients are asymptomatic; therefore, a routine early first-trimester sonogram in patients with previous cesarean section may be prudent for an early diagnosis. The cases of CSP in the present study were diagnosed at a mean gestational age of 6 weeks, resulting in only 5% major complications of bleeding requiring blood transfusion. A systemic review of CSP cases by Gonzalez and Tulandi 25 reported gestational age at the time of diagnosis ranging widely between 5 and 16 weeks, with a mean (SD) of 7 (2.5) weeks, with a higher complication rate in later diagnosis since it is likely to be related to higher beta hCG levels, severe vascularity, and therefore increased risk for bleeding.
To date, the optimal treatment modality of CSP is inconclusive due to limited reports with large numbers and the paucity of well-designed randomized controlled trials. Several treatment modalities are available, including expectant management, systemic MTX, local MTX, D&E, uterine artery embolization, hysteroscopy, and laparoscopy. Expectant management is usually not recommended due to the serious complications and consequences that might occur (i.e., massive hemorrhage, placenta accreta, uterine rupture).14,26,27 MTX is the most widely used treatment modality. Timor-Tritsch et al. 4 reported 19 patients between 6 and 14 weeks of pregnancy treated with a combined intramuscular and intragestational MTX injection. No complications were observed and beta hCG decreased, as expected. In the present study, 17 cases were treated with multidose systemic MTX; 70% were successful, and 6 cases were treated successfully with local MTX. Bodur et al. 28 concluded in a review that systemic MTX treatment for CSP is effective during the following conditions: beta hCG levels <12,000 mg/dL, negative embryonic cardiac activity, and <8 weeks of gestational age. In the present study, a cutoff of 9300 mg/dL of beta hCG for a successful primary treatment was noted.
A randomized controlled trial comparing systemic single-dose MTX to local MTX found both treatments to be equally successful (67.3% vs. 69.2%, respectively). However, the resolution of the pregnancy was faster in the systemic group. 29 Single-balloon catheter after local injection of methotrexate and double-balloon catheter were also reported as possible treatments of CSP. 15 Timor-Tritsch et al. 15 reported that the double-lumen catheter should be placed for a median of 3 days. In their study of seven CSPs and three cervical pregnancies, the median time from treatment to the total drop of human chorionic gonadotropin was 49 days, with no major complications observed. In the present study, a double-lumen catheter was used in three cases of CSP, with mean beta hCG levels of 34,200 mg/dL and a mean time to resolution of beta hCG levels of 34 days. The success rate was 66%, with one case needing uterine artery embolization due to bleeding.
Limitations of the current study were the small sample size, retrospective design, and a comparison of different types of CSP, which have different risks for complications. Strengths of the study were the comprehensive clinical information available in the patients’ medical records and data on different treatment modalities. Because multiple treatments were successfully implemented, results of this retrospective case series may suggest that treatment should be tailored individually for each patient, with availability of several second-line modalities, as well. Low-risk patients, especially those with type I CSP (in contrast to high-risk patients with positive heartbeat, high vascularity, and type II scar), may benefit from early evacuation of the sac. Failure to evacuate the sac early might later have complications, such as high-level vascularization, bleeding, and prolongation of time to resolution. Patients should therefore be aware of the prolonged course of time to complete resolution and be prepared for the possibility of needing second-line treatment. In addition, no cases were complicated by hysterectomy, which was undesired due to prospective wishes of fertility.
Results of this retrospective case series demonstrate the importance of identifying patients at risk of CSP. It is crucial that sonographers performing initial sonograms for confirmation of pregnancy in these patients are aware of these risks and their associated sonographic appearances for proper diagnosis. In addition, extra caution in the treatment plan should be taken in cases of CSP that have a high likelihood of complications, such as type II scar, severe vascularity, the presence of a heartbeat, and high levels of beta hCG. Treatment should be individualized, considering the imaging results, clinical symptoms, hCG level, the treatment modality available at each center, and the surgeon’s skills. Further, larger scale studies are needed to determine the best treatment or suggest more options to specific clinical cases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.