
Abstract
Although still rare, the incidence of cesarean scar ectopic pregnancies has increased in the past few years due to the number of cesarean section deliveries being performed. If left untreated, this can have devastating complications for patients, including hemorrhage, uterine rupture, and maternal death. Occurrence of cesarean scar ectopic is about 1 in 2000 pregnancies. Most of these pregnancies have a normal rising beta-human chorionic gonadotropin (beta-hCG), and patients may present asymptomatic, with light spotting during early first trimester and with or without cramping. Due to rarity, there is very minimal awareness among sonographers of the likelihood of cesarean scar ectopic, which can be misdiagnosed as cervical pregnancy or spontaneous abortion in progress. Ultrasound is the primary imaging modality and plays a very important role in recognizing and providing proper early diagnosis.
Introduction
Ectopic pregnancy is the implantation of a fertilized ovum outside the endometrial cavity, and these account for 1% to 2% of all pregnancies.1,2 Cesarean scar pregnancy is a rare form of ectopic pregnancy, and sonographers should be aware of this possibility.3–5 Detection of cesarean scar pregnancy can difficult, and a false-negative diagnosis can result in complications including hemorrhage, uterine rupture, and maternal death. Sonography, typically the primary imaging modality, plays a very important role in recognizing cesarean scar implantation. 6 An empty endometrial cavity, gestational sac, or hypoechoic mass at the site of the previous cesarean delivery and a very thin myometrium anterior to a gestational sac are all signs that should raise the sonographer’s suspicion for a cesarean scar ectopic pregnancy. Early diagnosis aids in early treatment, avoiding complications and preserving patient fertility.
Case Reports
Case No. 1
A 31-year-old woman, gravida 3, para 2, with a history of cesarean section and rising beta-human chorionic gonadotropin (beta-hCG) levels presented to the outpatient clinic for a viability sonogram secondary to light spotting in the first trimester. Transvaginal sonography was done using a Siemens S2000 ultrasound system (Siemens Healthcare, Malvern, PA) with a transvaginal EC9-4 probe. Sonographic findings included a viable fetus with a gestational age of 5 weeks and 6 days and a heart rate of 111 beats per minute (bpm) located within the cesarean scar from the prior delivery (Figures 1 and 2). Very little overlying myometrium was seen anterior to the gestational sac. The results were given immediately to the obstetric physician on call as soon as the examination was completed. The patient was counseled about the risk of the condition by the physician, and she was advised to proceed with hospitalization for treatment of the cesarean scar ectopic pregnancy. Prior to admission, the patient had another sonogram at a local hospital that confirmed implantation of the pregnancy in the scar. During hospitalization, the patient underwent systemic methotrexate treatment and was monitored for decrease of her beta-hCG levels. She was discharged from the hospital on day 9 with instructions to continue beta-hCG testing until complete resolution of the pregnancy. No further sonographic images regarding resolution of the ectopic pregnancy were available as she transferred her care to another medical facility.

Transvaginal gray scale sonogram showing a fetus within the cesarean section scar. Note the characteristically thinned myometrium just anterior to the gestational sac.
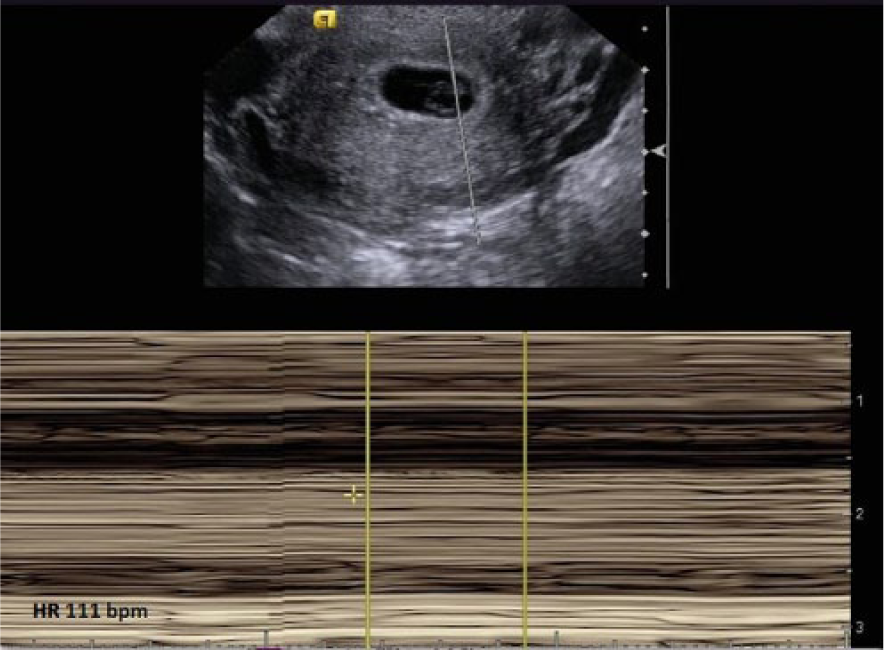
Transvaginal M-mode sonogram through the gestational sac seen in Figure 1 showing a heart rate of 111 beats per minute.
Case No. 2
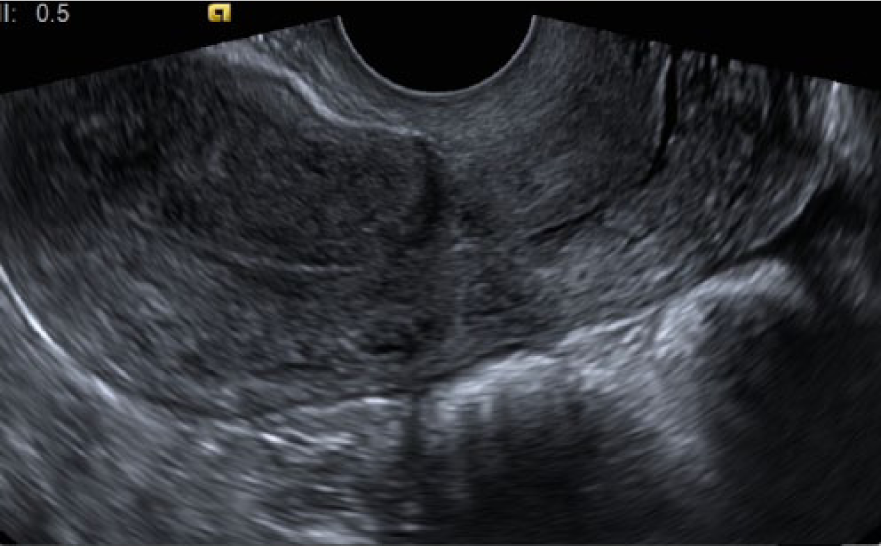
A 34-year-old woman, gravida 2, para 1, with a prior cesarean section delivery presented to the same clinic for a viability ultrasound secondary to light bleeding in the first trimester. Transvaginal sonography using a GE Logic E9 ultrasound system (GE Healthcare Ultrasound, Waukesha, WI) and a transvaginal RIC 5-9 probe showed a viable fetus with a gestational age of 6 weeks and 2 days and a heart rate of 97 bpm located in the lower uterine segment in the proximity of the prior cesarean section scar (Figures 3 and 4). There was a 3 mm space between the gestational sac and outer border of the myometrium. Sonographic findings were reported immediately to the obstetric physician on call. The patient was transferred to a local hospital where repeat transvaginal sonography confirmed the diagnosis of a cesarean scan ectopic pregnancy, and she was admitted for treatment. Based on the patient’s desire to preserve future fertility, the size of the gestational sac (less than 8 weeks), and the patient’s hemodynamic stability, the decision was made to proceed with systemic methotrexate treatment. During the length of treatment, beta-hCG was noted to be trending down appropriately. After a 9-day hospital stay, the patient was discharged home with a plan to undergo serial beta-hCG testing and follow-up sonography to monitor the resolution of the ectopic pregnancy. Two months after the initial diagnosis, repeat transvaginal sonography was done and showed no evidence of any remaining ectopic pregnancy (Figure 5).

Transvaginal gray scale sonogram showing a fetus in the proximity of the scar from a previous cesarean section. Again note the characteristically thinned myometrium just anterior to the gestational sac.
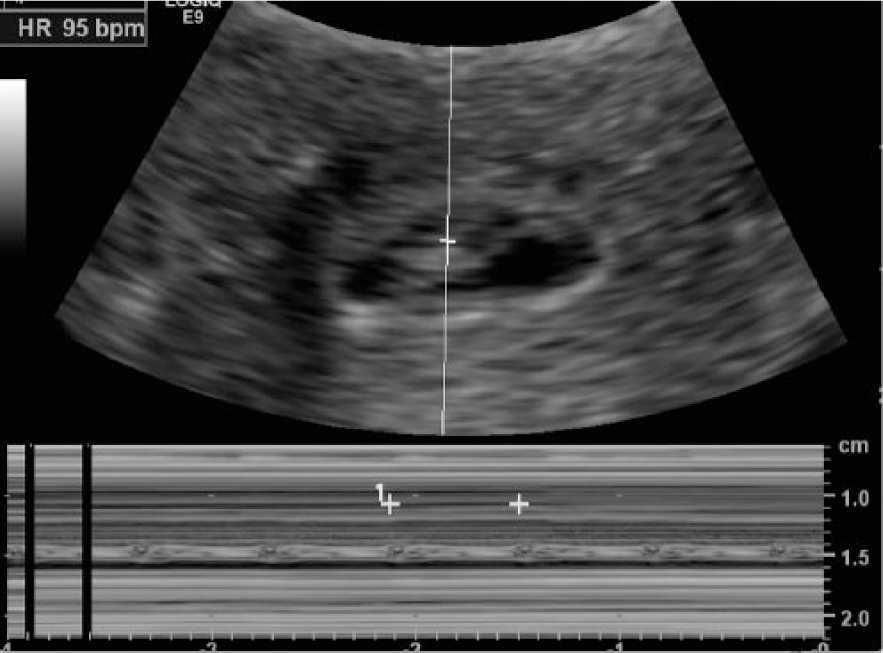
Transvaginal M-mode sonogram through the gestational sac seen in Figure 3 showing a heart rate of 95 beats per minute.
Discussion
Ectopic pregnancy is common and can be potentially life threatening. 1 A cesarean scar ectopic pregnancy is seen as a gestational sac embedded within the cesarean scar, surrounded by scar tissue, and separate from the endometrial cavity; this location is unusual and rare.2–5 A recent report by Natasha et al 2 estimates an incidence of ectopic pregnancy in a previous cesarean scar in about 1 in 2000 or 6% of ectopic pregnancies among women with prior cesarean delivery. Cesarean section scar pregnancies can happen spontaneously in addition to in vitro fertilization. 5 Early diagnosis can be vital for the patient since implantation with trophoblastic invasion into scar tissue without supportive myometrium can cause uterine rupture. 6
The exact cause of implantation within the scar is not well understood, though it may be related to incomplete or improper healing of the scar. 3 A possible mechanism for implantation in this location is a migration of the embryo through a microtubular tract/fistula between the cesarean scar and the endometrial canal or a wedge defect in the lower uterine segment.3,4 Uterine surgery (dilation and curettage, myomectomy, and hysteroscopy), in vitro fertilization, and manual removal of the placenta may be other factors that contribute to formation of the fistula between the scar and the endometrium.5,7
Most patients with a cesarean scar pregnancy in the early stages will have light to moderate bleeding, with or without cramping, or may be asymptomatic. The trend of beta-hCG levels rising can mimic a viable intrauterine pregnancy. As the pregnancy continues, the symptoms typically will progress to very heavy bleeding and severe pain. Acute onset of intense pain can be an indication of uterine rupture.3,4
Sonography is used as a primary diagnostic imaging modality in recognizing cesarean scar pregnancy between 5 to 10 weeks gestation, 6 although it is possible to make the diagnosis as late as 16 weeks gestation if uterine rupture has not occurred. Later in the first trimester, cesarean scar ectopic pregnancy can be difficult to distinguish from a cervical pregnancy, a low implanted pregnancy, or a pregnancy with a placenta accreta; it can also be misdiagnosed as a spontaneous abortion in progress. 2 Hysteroscopy may be helpful for these cases.4,8
Early diagnosis is critical in avoiding complications that can include hemorrhage, uterine rupture, need for emergency hysterectomy, and maternal death. 3 Endovaginal sonography plays a very important role in the proper early diagnosis of a cesarean scar ectopic pregnancy with an overall reported sensitivity of more than 90%.3,6 Sonographic findings in early cesarean scar pregnancy are:
an empty uterine cavity and an empty cervical canal with the gestational sac or hypoechoic mass located in the anterior wall of the uterus at the area of cesarean scar from the previous delivery;
visualization of a very thin (less than 5 mm) or nonexistent layer of overlying myometrium anterior to the gestational sac;
discontinuity of the anterior uterine wall in the sagittal plane with a bulging gestational sac;
color and/or spectral Doppler evidence of perfusion around the gestation sac/mass.
Magnetic resonance imaging (MRI) can be used to confirm the pregnancy location but is usually not necessary for making a diagnosis. 5
Optimal treatment for a cesarean scar ectopic pregnancy is not well established and depends on patient presentation, severity of symptoms, the hemodynamic status of the patient, and the gestational age of the pregnancy. 3 There are several treatment managements that have been used, including systemic (intramuscular injections) or local (intragestational sac injection) administration of methotrexate, selective uterine artery embolization, hysteroscopy, laparotomy, and in some cases, hysterectomy.3,4,9–11 The most commonly reported treatment option for early diagnosed cesarean scar ectopic pregnancy (gestational age less than 8 weeks) is methotrexate administration.9,10 Generally, systemic (intramuscular) methotrexate treatment for a patient who is pain free and hemodynamically stable, with gestational age less than 8 weeks, has been shown to be successful. Prior to the systemic treatment, the patient needs to have baseline full blood count and liver and renal function tests done. Since the systemic approach calls for repeated doses, some physicians prefer local/direct injection of methotrexate into the gestational sac under direct sonographic guidance, which results in interruption of the pregnancy more rapidly.4,9 Published series show that medical treatment with methotrexate is successful in approximately 70% to 80% of cases. 4 Both of the patients presented had systemic administration of methotrexate without complications.
The primary advantage of medical management is the avoidance of surgery, which can be associated with complications, and the preservation of future fertility. The disadvantage is the slow resolution of the pregnancy, with the risk of rupture and the possibility of a necessary hysterectomy if treatment fails. Because of these factors, patients usually are hospitalized for the length of the medical management to monitor for bleeding and decline of beta-hCG levels. If medication therapy is unsuccessful, surgical intervention may be necessary.8,10
Conclusion
A cesarean scar ectopic pregnancy may lead to severe complications and maternal death secondary to hemorrhage if not detected early. Although this type of ectopic pregnancy is still a rare occurrence, sonographers should be aware of the possibility of a cesarean scar pregnancy. Transvaginal sonography plays an important role in providing the proper diagnosis. No pregnancy in the uterine cavity, a thin or absent myometrium between the gestational sac and bladder, and interruption of the anterior lower uterine segment wall in the sagittal plane are all strong indicators of a cesarean scar ectopic pregnancy. Methotrexate treatment is usually successful with early diagnosed cesarean scar ectopic pregnancies. Early detection and management play an important role in providing the proper treatment, avoiding complications, and preserving patient fertility.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.