
Abstract
The proportion of sonographers who scan in pain is increasing, in spite of recommendations and guidelines for proper body mechanics and for the use of ergonomic equipment in the workplace. No study has examined in detail the type of equipment that is available to sonographers in the workplace and whether sonographers who have access to ergonomic equipment are scanning in pain. This study evaluated the proportions of sonographers who had access to various types of ergonomic equipment and compared the results with the prevalence of scanning-related pain. Most sonographers had access to ergonomic features manufactured into ultrasound machines but had less access to equipment provided by employers, such as scanning chairs and cable braces. Sonographers who had access to machines that had swiveling keyboards reported less pain and injury than those who did not.
Current research on ultrasound ergonomics shows that work-related musculoskeletal disorders (WRMSDs) are a prevalent hazard among sonographers.1–9 In particular, the neck, shoulder, and wrist appear to be injured most frequently.1–9 Studies have associated equipment design (including console design and transducer design), duration of work, awkward body postures, and workplace culture as having the potential to increase the risk of WRMSDs.2–4,6–9 Awareness of the issue began in the late 1990s, and much of the evidence-based research has been replicated.
In 1997, Pike et al. published sentinel research revealing that >80% of sonographers scan in pain that is directly attributed to workplace tasks. 1 Since then, multiple studies have shown sonographers scanning in pain 75% to 90% of the time.2–6
Sonographers primarily report WRMSDs as pain in the shoulder and neck.1–6 Back pain is also frequently reported, followed by hand and wrist pain.1,3,4,7 Other WRMSD-related symptoms include tingling or numbness of the extremities, weakness in one or both extremities, motion restriction, numbness in hands upon awakening, and clumsy fingers.3,5
To minimize pain, a machine console height that allows for 90° elbow bend and an elbow support sling are effective tools to reduce muscle activity in the neck and trunk. 8 Muscle activity in the upper trapezius and rotator cuff muscles decreases when the need to reach for the ultrasound console is eliminated. 9 Muscle activity also decreases when arm abduction is reduced from 75° to 30° and more so when support cushions are used to support the scanning arm. 9
Studies report that approximately 80% of sonographers have access to adjustable scanning tables and height-adjustable chairs but that the tables may not have electronic controls and that the chairs may not be adequate for proper scanning postures.4,6 Studies that report the use of a cable brace while scanning are minimal, and the overall relationship between the use of a cable brace and scanning in pain has not been evaluated. 4 Workplace culture appears to prevent sonographers from reporting their injuries to management, citing lack of formal mechanisms to do so, fear of retaliation or job loss, and feelings of hopelessness that the problem would be addressed.1,4,6,7,10
Effectiveness of ergonomic education has been sparsely researched. 6 Most sonographers report no formal training in ergonomics and no support from upper management for an injury prevention program.6,7 In 2015, Hancock presented an intervention to encourage student sonographers to adopt proper ergonomic behaviors in the workplace. 11 Her technique integrated a unique blend of instructor and peer feedback during the student experience, which created sustained ergonomic behaviors postgraduation. 11 Students who received feedback reduced their negative ergonomic behaviors as compared with groups that received no peer feedback or participated in self-instructional activities. 11 As part of a longitudinal follow-up study, she noted a possible lack of access to ergonomic equipment in the sonography workplace once employed. 11
Previous studies evaluated the area of pain, the prevalence of pain among sonographers, and the possible causes of WRMSD symptoms. In spite of increased awareness, the prevalence of sonographers with WRMSD symptoms does not appear to change.1–9 The studies indicate that WRMSD symptoms are associated with longer work days, more years in the profession, and awkward body movements and postures.1–9 The proportions of sonographers scanning in pain, the areas of pain, the tasks that cause pain, the equipment limitations, and the workplace culture are similar across all the reviewed studies.1–7 Some problems with the studies include small sample sizes,2–5 no statistical analysis reported,5,8 and no report of individual correlation between measurements. 9 Three of the cross-sectional studies do have large sample sizes and thus are more generalizable to all sonographers.1,6,7
Industry guidelines have been established for equipment manufacturers, employers, and sonographers. 12 It is unclear why sonographers continue to report a high prevalence of WRMSD symptoms. In a comparison of Pike et al. with Evans et al., the age of the workforce increased by 10 years between the studies, which coincidentally corresponds to the time span between the research of the two cohorts.1,6 Therefore, age could contribute to the increase in the prevalence of WRMSDs in that interval. 6 There was an increase in the awareness of ergonomic issues and more education available. 6 Furthermore, many ergonomic features were introduced into the ultrasound machine design, but the prevalence of sonographers scanning in pain increased.1,6 Applying transducer pressure, sustained shoulder abduction, and twisting motions remain constant as the main sources of pain.1–6
Of surveys that asked about ergonomic education, none of the respondents cited an education or training program as a source of information. 6 This phenomenon is surprising when considering that the education standards of the Joint Review Committee on Education in Diagnostic Medical Sonography require ergonomic education in educational programs. 13 It is unclear if there is an intervention that would alter sonographer behaviors and whether behaviors could be sustained in the absence of ergonomic equipment or workplace policies that support proper ergonomics. The least reported area is the availability of ergonomic equipment in the workplace, especially the ancillary equipment described as industry standards, with only two studies reporting access in any detail.4,6 Finally, ergonomic interventions have not been thoroughly explored through randomized controlled trials.
The purpose of this research was to determine the amount of access to ergonomic equipment in the workplace, including all the equipment recommended in the consensus statement, and to establish a potential relationship between the availability of that equipment and whether sonographers who have access to it are scanning in pain. A second purpose included contributing to the current knowledge about whether specific pain is related to specialty areas and to determine how many sonographers report their WRMSD symptoms to administrators.
Methods
The research project was reviewed by an institutional review board, which granted it exempt status. An 18-question survey consisting of questions regarding sonography ergonomics and access to ergonomic equipment was created with Qualtrics online survey software. The survey was distributed to 230 diagnostic medical sonographers who were practicing in various specialty areas and registered in a clinic instructor database for a diagnostic medical sonography program accredited by the Commission on Accreditation of Allied Health Education Programs. The sonographers had varied levels of student contact on a weekly basis, and patient care was their primary job task. Only sonographers who had valid email addresses and were in a registered database were surveyed—for two reasons: (1) to calculate an accurate rate of return and (2) to ensure a necessary sample size for study power. For the complete survey, see the appendix.
Questions 1–4 asked for demographic information, including age, sex, and years of scanning. Questions 5a–5e asked sonographers to identify any scanning-related pain, including the area of pain, the frequency of that pain, and whether they reported pain to a supervisor. If respondents indicated that they reported their pain to a supervisor, they were asked to describe the supervisor’s response. Sonographers who did not report pain were given an open-ended question to describe why not.
Questions 6–18b were related to sonographers’ access to adjustable ultrasound machines, examination tables, and chairs and various types of adaptive equipment. If they reported having access to equipment, sonographers were asked to indicate if they used it. If sonographers did not use the equipment available to them, they were given the opportunity to describe why they chose not to use it.
The survey link, which was sent via email, was available during January 2016 and remained open to participants for 2 weeks. A reminder email was sent to all participants 1 week after the first email. Responses were analyzed with SAS 9.4 (SAS Institute, Cary, North Carolina). Incomplete surveys were not included for analysis. Frequency data describe the demographic information and access to ergonomic equipment. Dependent on expected cell counts, a series of chi-square or Fisher’s exact tests were used to compare whether sonographer self-reported pain was associated to access to certain types of ergonomic equipment. A logistic regression model was used to calculate odds ratios of prevalent work-related pain or injury. All statistical testing was completed with an alpha set at 0.05. It was hypothesized that sonographers’ scanning-related pain is correlated to specialty area and the availability of ergonomic equipment. It was believed that ≥80% of the respondents would answer yes to 5a and 5b, <50% would say yes to 5d, and <50% would say yes to questions 6–18. A sample size of 28 was required for a two-sided 95% confidence interval with a 15% margin of error.
Results
A total of 102 responses were collected out of 230 survey recipients, for a rate of 44.3%. After incomplete responses were dropped, 98 responses were available for analysis. To have sufficient responses in each cell for the chi-square or Fisher’s analysis, the specialty categories were combined as follows: both general categories were collapsed together, as were the cardiac categories. The “other” responses were evaluated and determined to best fit with the general category. Within the remaining categories, 44.9% of respondents (n = 44) were general sonographers; 36.7% (n = 36), cardiac; 12.2% (n = 12), obstetrics/gynecology, and 6.1% (n = 6), vascular. The average time scanning for all specialties was 11.3 years, and the mean age of the respondents was 37 years. Among survey respondents, 86.3% (n = 85) were women, and 13.3% (n = 13) were men.
Fifty-three percent (n = 53) experienced pain as a result of scanning. The most common areas of this pain, ranked highest to lowest, were shoulder (56.6%, n = 30), neck (24.5%, n = 13), wrist (11.3%, n = 6), and back (7.6%, n = 4). When pain was compared with the specialty area, no significant associations were found (P = .69). Results are presented in Table 1. There is no evidence of an association between sonographer age and report of scanning pain or injury (P = .64). Only 20.8% (n = 11) of the respondents with pain reported it to administrators, leaving 79.3% (n = 42) of sonographers with unreported pain. Open-ended responses on why they did not report it include responses such as “Nothing would be done if I did,” “It’s not severe enough yet,” or “It is probably my own fault.”
Comparing Sonographer-Reported Pain by Specialty Area. a
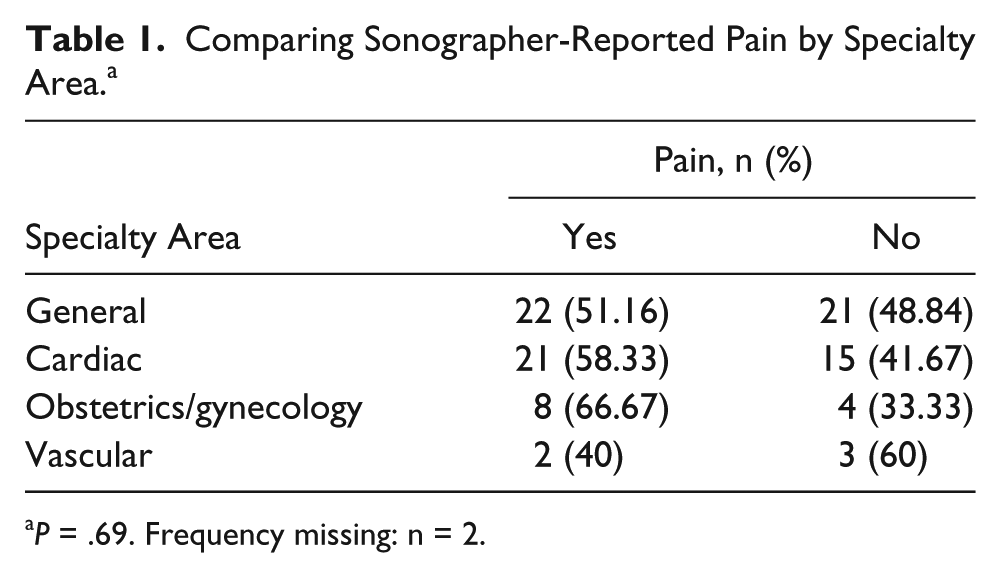
P = .69. Frequency missing: n = 2.
Access to ergonomic equipment results are detailed in Table 2. Notable is that 92.9% of sonographers (n = 91) have access to machines that have adjustable height; 92.8% (n = 90) have access to machines with a monitor that moves separately; and 94.6% (n = 94) have access to height-adjustable scanning tables. The swivel keyboard had a reported access of 72.5% (n = 71). Ergonomic chairs were available to 37.8% (n = 37), and only 2% (n = 2) reported access to a cable brace that supports the weight of the transducer cord.
Access to Ergonomic Equipment.
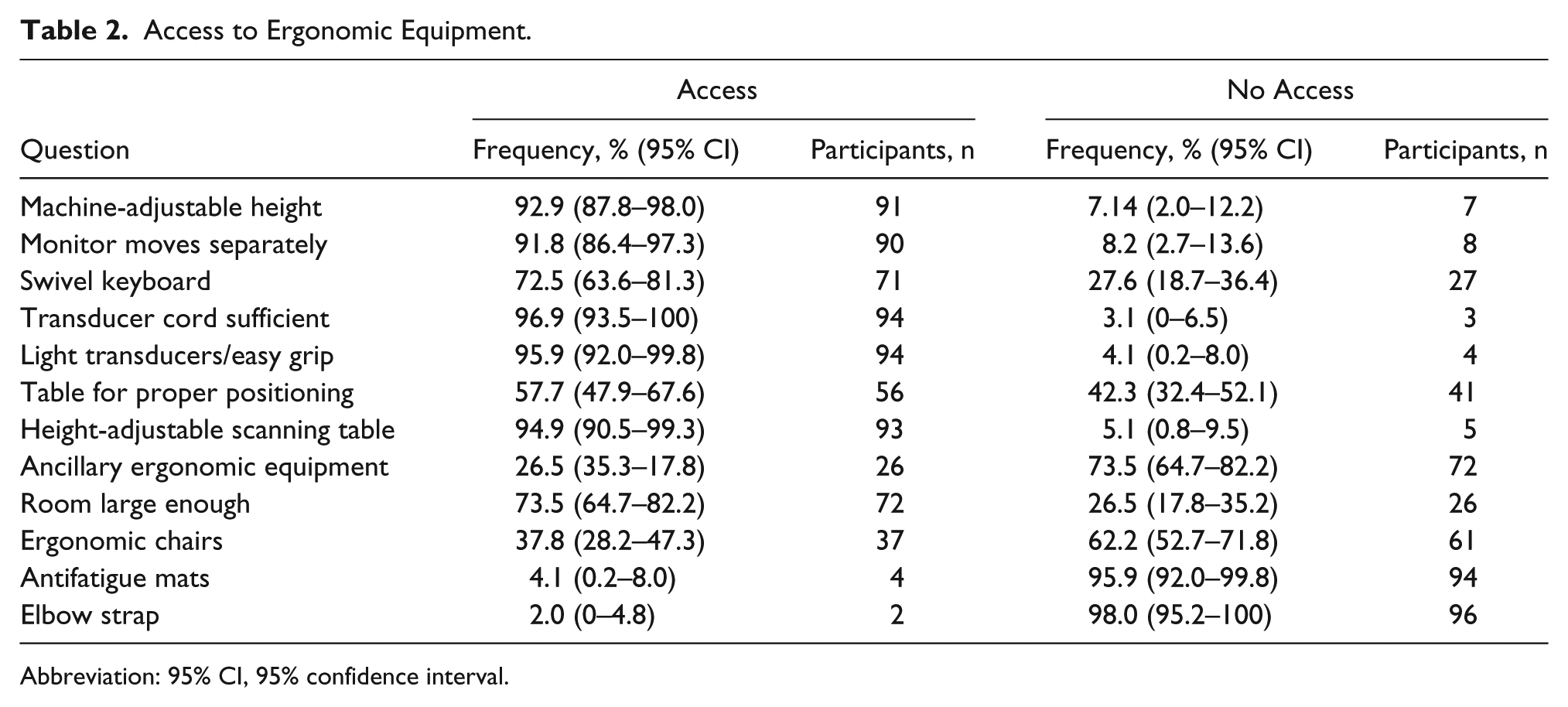
Abbreviation: 95% CI, 95% confidence interval.
When access to ergonomic equipment was compared with pain, the only significant finding was related to the swivel keyboard. Respondents who use a swivel keyboard reported less pain or injuries than those without a swivel keyboard (P = .02). No other associations between reported pain and the availability of equipment were significant. Detailed results are reported in Table 3. While no other results were significant, increasing the tolerance for alpha errors from 0.05 to 0.10 showed three more variables that correlated to scanning pain and injury. Access to a separate moving monitor (P = .07), large-enough rooms to accommodate scanning needs (P = .07), and an ergonomic chair (P = .06) showed lower associated pain or injury proportions.
Comparison of Access to Equipment and Proportions of Sonographers Reporting Pain or Injury.
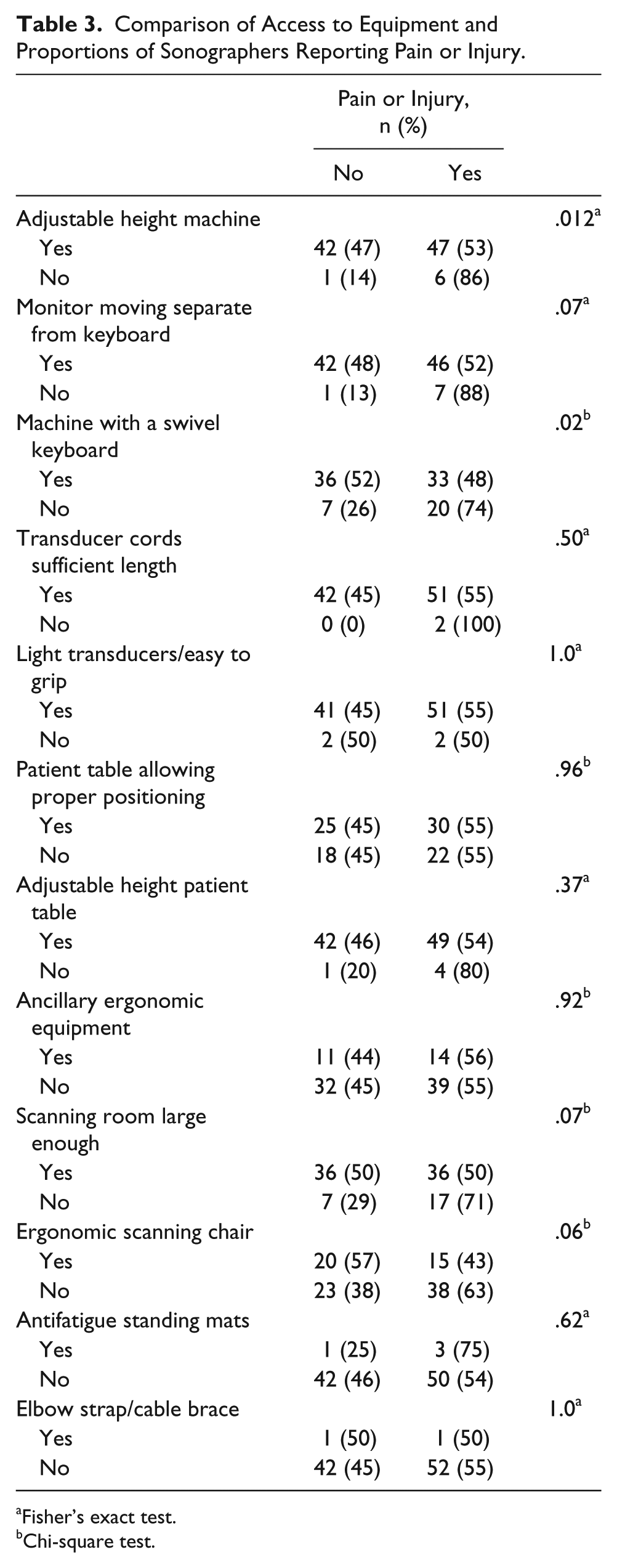
Fisher’s exact test.
Chi-square test.
A logistic regression model was used to determine adjusted odds of prevalent work-related injury or pain. Tests for interaction and confounding adjustments for age, sex, years scanning in specialty area, and total years scanning were included in the model. The three variables that had previously demonstrated weak association after alteration of the alpha (separate moving monitor, room large enough to accommodate scanning needs, and ergonomic chair) showed no associations, were not confounding variables, and thus were eliminated from the model. There was no evidence of any interaction among the covariates in the model (P > .05 for all interaction tests). After adjusting for age, sex, years scanning in specialty area, and total years scanning, having a swivel keyboard was associated with less work-related injury or pain (P = .008). The adjusted odds of having prevalent work-related injury or pain was 4.0 (95% confidence interval, 1.4-11.2) times higher among sonographers who do not use machines with swivel keyboards as compared with those who do.
Discussion
Ergonomics is the study of a person’s efficiency in the workplace, and it includes the concept that the physical work environment should adjust to fit the employee. For sonography specifically, it is the sonographer’s ability to adjust the physical environment so that he or she can scan comfortably and deliver diagnostic examinations and high-quality patient care. The concept of an ergonomic workplace has been a challenge for sonographers and continues to be an obstacle in spite of increased awareness of the problem.1–4
Sonographers can generate up to $1.1 million of billable revenue per year, and when a sonographer is injured and cannot work, there is a loss of approximately 60% of that revenue. 14 Additionally, workers’ compensation can cost a department $32 000 per year per person, which does not include the additional $130 000 to $160 000 for replacement staff. 14 The monetary loss is also accompanied by indirect costs, such as a loss of revenue from a down ultrasound room, a loss of experience and knowledge that is not easily replaced, and a cost of hiring either temporary workers or permanent replacements. 14 Overall patient care and the diagnostic quality of sonograms suffer with this loss of work experience.
Ergonomic awareness and education are growing trends. A keyword search for “ergonomics” in the Journal of Diagnostic Medical Sonography returns >25 relevant articles. It is possible that a more comprehensive search would show even more awareness of the problem. Factors contributing to endemic sonographer WRMSDs include behavior that sonographers can and must correct. Additionally, the availability of ergonomic equipment in the workplace that will allow the sonographers to make these required behavior changes is necessary. Administration is responsible for ensuring that ergonomic equipment is available, adopting policies favoring proper body mechanics, and encouraging or requiring the use of ergonomic equipment. In addition, administration is responsible for the development of formal mechanisms to report WRMSDs without fear of repercussion and for the establishment of protocols to ensure that these mechanisms are followed. Therefore, sonographers and administrators are both responsible for proper ergonomics in the workplace.
This study shows that there is wide access to ergonomic ultrasound equipment in the workplace, such as height-adjustable machines, monitors that move separately from the console, adequate-length transducer cords, light transducers with good hand grips, and height-adjustable scanning tables. Equipment manufacturers may be responsible for the majority of this access, as over the past 10 to 15 years there have been radical changes in equipment design to include most of these features. It is unclear if administrators or even sonographers made a conscious effort to ensure or request that the properly designed equipment is available or if it is a by-product of replacing older equipment, as most manufacturers currently include all the recommended ergonomic features as standard equipment design.
In this study, access to an ergonomic chair is lacking, with only 37.8% having one, which is lower than the percentage of respondents in Evans et al, who reported that 86% had one. 6 This difference may be explained by the smaller sample size in this study, but the magnitude of this difference is not associated with the sample size; rather, it is more likely that sonographers in this region have lower access to ergonomic chairs. The access to adaptable equipment, such as antifatigue standing mats and arm support cushions, is currently poor, and the worst access is to the least expensive ergonomic equipment: the cable brace, which retails for <$20. Although this study did not report associations between pain and access to these two pieces of equipment, the low numbers of sonographers reporting accessibility may have impeded the ability to detect a difference. However, use of cable braces or elbow straps to offset the weight of the transducer cord are recommended, 12 and given the low cost, it is a piece of equipment that a sonographer could provide personally. Given the small proportion of cable brace users, sonographers are either unaware of the availability of this piece of equipment or choose not to use it. Overall, employers need to improve employees’ access to adaptable ergonomic equipment, as costs of this equipment are relatively low when compared with the cost of ultrasound machines or treatment of WRMSDs.12,14
This study remains consistent with other studies regarding reasons why few sonographers report their pain to appropriate administrators. Comments including self-blame show an unwillingness to change the problem; the individual knew that she or he had the power to improve the symptoms but chose not to. Some sonographers stated that they did not believe that administration would respond in a helpful way and, therefore, reporting was not worth the time. These comments allude to the idea that the sonographer feels powerless to change the problem. Perhaps the most alarming comment came from a sonographer who reported a fear of job loss and was scared to be seen as a liability to the employer. This response indicates that administrator attitudes can influence the reporting of pain.
A limitation to the study is the lower sample size as compared with the studies by Pike and Evans,1,6,7 but it is greater than that of many studies.2–5,8–10 A larger sample size may have been achieved with snowball sampling, but the rate of return would be unknown. This research included a response rate >40%, which is considered strong when compared with past studies that had closer to a 30% response rate,1,6,7 and it had the statistical power to detect differences.
The respondents in this survey self-selected to answer, which could have led to the likelihood of injured sonographers being more motivated to respond. While the average years in the profession was similar to that of previous studies, the respondents’ average age was younger.1,6 The younger age could have contributed to a lowered rate of sonographers reporting scanning-related pain: 53% in this study versus 80% reported in most studies.1,6 The replies were limited to a particular geographic area and therefore may not be representative of sonographers across the United States. The survey did not describe in detail what adaptable equipment is, and for this reason, some respondents could have misinterpreted the question. Specific dimensions of the scanning room were not described, so the respondents may have answered subjectively to that question. For these reasons, this study should be repeated to reach a larger population in more diverse geographic areas. Finally, this study was not a randomized controlled trial, so it does not prove whether access to ergonomic equipment causes the reduction in the risk of WRMSDs.
This study shows that the availability of a keyboard that swivels separate from the console is associated with less work-related pain. The open feedback obtained in regard to administrator response provided information on pain reporting that was not previously known. This study shows that access to ergonomic equipment provided by the employer is low—including height-adjustable tables and chairs, support cushions, and cable braces—in spite of the knowledge that the use of such equipment can decrease workplace injury. Additionally, better mechanisms to report workplace injury are needed.
Although administrators play an important role in providing access to ergonomic equipment, sonographers must adopt the mind-set that proper ergonomic behaviors are not an option but a requirement. To change behaviors, sonographers first must believe that they are at risk for pain or injury. 11 Hancock noted that the most common method to deliver ergonomic education is passive, via lectures and articles, which may not foster true behavior modification. 11 Future research should be aimed at developing an active education model that inspires sonographers to change their behavior.
A scanning-related WRMSD should not be a forgone conclusion. To provide quality patient care, sonographers and administrators need to work together to prevent injuries. Randomized controlled trials may be needed to determine what interventions are the best at preventing scanning-related pain. Further studies that examine specific behaviors and access to ergonomic equipment are also needed to improve understanding of this complex issue.
Footnotes
Appendix: Email Survey
You have been asked to participate in a research project sponsored by a student in the Sonography program at the University of Oklahoma Health Sciences Center. Participation is completely voluntary, and there is no benefit or risk to you for participating. You will be completely anonymous and will not be identified in any way. By entering the survey you are agreeing to participate in research. During the survey, you may answer as many or as few questions as you wish. You may also leave the survey at any time. If you do not wish to participate in this research, you should not click on the link that leads to this survey.
Screening: I am at least 18 years old or older. Yes/No
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.