
Abstract
Acute abdominal pain in the pediatric patient is a common clinical symptom often resulting in uncertainty and thus often subsequently leads to a sonographic examination of the abdomen. Sonography is often the modality of choice for pediatric abdominal imaging, and consequently, sonographers should have a fundamental appreciation for the causes of acute abdominal pain in the pediatric population. Intussusception, which is the telescoping of a proximal segment of bowel into a distal segment, is one potential cause of acute abdominal pain for these patients. This review clarifies the etiology and classification of intussusception and provides an overview of the clinical manifestations, sonographic identification, and treatment of this potentially severe disorder. Also, this review provides a novel imaging sign, called the “cinnamon bun” sign, that sonographers can employ while examining patients for possible intussusception. The cinnamon bun sign is a descriptive term that may be used to illustrate a transverse sonographic plane through an intussusception.
Sonography is often the modality of choice for pediatric abdominal imaging due to its ease of use, lack of ionizing radiation, and cost-effectiveness. Consequently, sonographers should have a fundamental appreciation for the causes of acute abdominal pain in the pediatric population. Intussusception, which is the telescoping of a proximal segment of bowel into a distal segment, is one potential cause of acute abdominal pain for these patients.
The term intussusception is a combination of the Latin word parts of intus, meaning “within,” and susception, meaning “an undertaking” or “to take up.” It was first described by Paul Barbette of Amsterdam in 1674 as “introsusception,” only to obtain its official moniker over a century later by John Hunter when he encountered three cases.1,2 The first successful operation on a child with intussusception was performed by Sir Jonathan Hutchinson in 1871. 2
Intussusception is described as a condition that results from the invagination (telescoping) of a proximal segment of the bowel into a distal segment (Figure 1).2,3 The proximal segment may be referred to as the intussusceptum, while the distal segment may be referred to as the intussuscipiens. 3 The initial telescoping of bowel prohibits normal intestinal function by effectively producing a bowel obstruction, only to be further propagated and possibly enhanced by normal peristalsis. Unfortunately, as the regular waves of peristalsis encounter the intussusception, there exists the potential for further invagination of the intussusceptum into the intussuscipiens. As this continued telescoping effect occurs, there is an increase in the length of the intussusception, with the eventual involvement of the mesentery and its blood vessels, thus heightening the prospect for potentially devastating consequences, including vascular compromise and bowel necrosis. 1
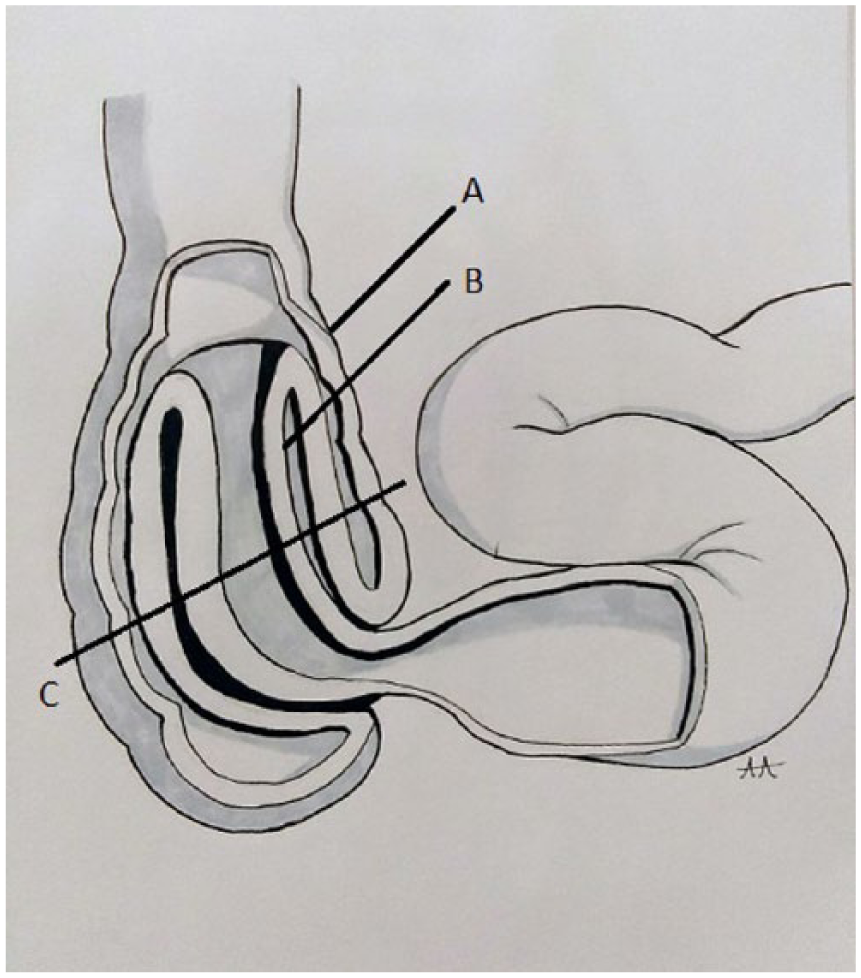
Diagram of intussusception. (A) The intussuscipiens is the distal segment of bowel. (B) The intussusceptum is the proximal segment of bowel into which the intussuscipiens invaginates. (C) Represents a transverse section of an intussuception, depicted by Figure 2. Drawing by Alicia Arellanes.
Etiology of Intussusception
Although intussusception can occur in adults, Yalamarthi and Smith 2 found that 95% of cases are discovered in the pediatric population. 2 Intussusception, which is more likely to be discovered in males, is the most common cause of intestinal obstruction in children, and it most often occurs in pediatric patients between the ages of 6 and 36 months of age, with a peak occurrence between 5 and 7 months.4,5 Kang and Peters 5 and Wang et al. 6 identified intussusception as the second most common cause of acute abdominal pain in children between the ages of 3 months and 6 years. Overall, Kaya et al. 7 found an estimated incidence of 0.1% to 0.4% for intussusception in live births. The overwhelming majority (90%) of childhood cases of intussusception are of unknown origin. 2
Idiopathic intussusception is not considered a genetic disease, although some familial distribution has been reported. 7 Kaya et al. 7 provided a case report of simultaneous intussusception found in 6-month-old identical twins. The twins presented within hours of each other with both clinical and imaging findings consistent with intussusception. 7 Other similar cases of simultaneous intussusception have been reported, including another set of identical twins and one set of 18-month-old fraternal twins. 7
Pendergast and Wilson 8 describe a strong association between intussusception and the idiopathic enlargement of Peyer’s patch, which is lymphoid tissue that is most often located along the surface of the distal ileum and jejunum. Although the enlargement of Peyer’s patch may be unknown in most cases, there has been a specific association established with the adenovirus infection. 5 The adenovirus is a common virus that is easily spread to others and can cause a wide range of illnesses, including the common cold, pneumonia, and gastroenteritis. 9 Individuals who are more prone to have adenovirus include infants and people with weakened immune systems. 9 Research conducted by Yalamarthi and Smith 2 found Peyer’s patch enlargement noted in nearly half of childhood cases of intussusception.
First described in 1911, Waugh syndrome provides an association between childhood intussusception and intestinal malrotation. 10 Intestinal malrotation in children is congenital and is described as the abnormal rotation and fixation of the bowel. 11 In those affected by Waugh syndrome, malrotation increases the susceptibility of intestinal prolapse, often of the ileocecal section of colon into the ascending colon. 10 It is suspected that Waugh syndrome is underreported and therefore may often be an underlying contributing factor in acute, as well as recurrent, intussusceptions.10,12
Peutz-Jeghers syndrome is a rare autosomal dominant disorder that is characterized by gastrointestinal polyps and mucocutaneous pigmentations. 5 Cagir and To 13 found that 50% of the patients with this syndrome will experience an intussusception during their lifetime. Many of the gastrointestinal lesions start developing early in life, coupled with an increase in risk for intussusception. 13
Rotavirus is a contagious virus, which often causes severe watery diarrhea, vomiting, fever, and abdominal pain due to gastroenteritis, the inflammation of the stomach and intestines. 11 The severe dehydration associated with rotavirus symptoms can lead to hospitalization and even death. 11 Rotavirus most commonly affects infants and younger children. While rotavirus (A) is the most common worldwide cause of acute gastroenteritis in young children, the advent of vaccines has drastically reduced the incidence of rotavirus-associated gastroenteritis, as well as the associated mortality.11,14 The use of the first rotavirus vaccine was suspended in 1999 due to an increased risk of intussusception in infants after dosage. 15 There are currently two Food and Drug Administration–approved second-generation versions of the rotavirus vaccine available and recommended by the Centers for Disease Control and Prevention (CDC), as well as the World Health Organization, as a part of a routine vaccination regimen for infants.11,14,15 These second-generation rotavirus vaccines still carry an increased risk for intussusception, primarily after the first dose, but it is a reduced risk in comparison to the first-generation vaccine. 15 According to the CDC, about 1 in 20,000 to 1 in 100,000 US infants who get rotavirus vaccine may develop intussusception within a week of getting the vaccine. 11 Consequently, 40 to 120 infants in the United States could develop intussusception as a result of rotavirus vaccination each year. 11
Classification of Intussusception
Intussusception is often classified according to the site of origin. Common locations include enteric, ileocolic, ileocecal, and colonic. 2 Enteric refers to intussusception confined to the small intestine, while colonic refers to intussusception within the colon. 2 The most common location of intussusception in children is within the right lower quadrant, in the area of the ileocecal valve.2,5,8 An intussusception located at the ileocecal valve is thus consequently referred to as an ileocecal intussusception. The ileocecal valve is often pinpointed as the lead point, or starting point, of the ileocecal intussusception. For reasons often not understood, the valve allows the ileum to invaginate into the cecum. 2 Ileocolic and ileocecal intussusceptions can be difficult to differentiate in clinical practice, although intralesional lymph nodes are commonly seen with ileocolic intussusception.2,16 Appendiceal intussusception is rare and usually a complication of appendicitis, but it can also occur in isolation or infrequently as an adjunct to ileocolic intussusception.3,16
Meckel’s diverticulum, located typically in the area of the distal ileum, is the most common congenital anomaly of the small intestines. 17 This outpouching can serve as a lead point, or beginning, of the intussusception. Other lead points include duplication cysts, appendicitis, inspissated meconium, tumor, or a polyp.16,18 Any intestinal abnormality that alters the normal peristaltic motion of the bowel increases the probability for intussusception. 8
Clinical and Sonographic Findings of Intussusception
Clinical findings of intussusception can vary, although the classic clinical triad, which includes vomiting, abdominal pain, and rectal bleeding, is often present. 8 The abdominal pain associated with intussusception tends to be intermittent, which is suggested to be the result of the interference of the normal peristaltic motion in the area of the invagination. 5 This pain may be referred to as paroxysmal, meaning a sudden recurrence. Also, the intussusception may be large enough to be palpable in some patients. 18 Pediatric intussusception is considered chronic when abdominal pain is intermittent and lasts more than 14 days, often without the presence of other clinical symptoms of intussusception. 12 Chronic intussusception is more common in older children and often associated with longstanding anorexia, vomiting, and significant weight loss. 12
In children, the presence of red currant jelly stool is a hallmark of intussusception. 18 Red currants are berries, similar to gooseberries, which are native to Europe but may be found in the United States. They are often used to create jellies and jams, and they may be included in some pastries and tarts. When squashed, the red currants create a substance that is similar in both consistency and color to that of the stool found in patients with intussusception. The presence of sloughed mucosa due to bowel compromise gives rise to this particular consistency. 19 Gross or occult blood with or without mucous may also be discovered in the stool of those afflicted with intussusception. 5
Sonography can play a vital role in the diagnosis of intussusception, especially for the pediatric patient. There is no patient preparation for a sonogram to investigate for possible intussusception, and although potential communication barriers may exist with pediatric patients, the sonographer could inquire about the area of pain in patients who can offer such useful clinical information. Having the patient identify the area of pain by pointing with a single finger can provide an explicit region of interest to be examined. For infants, a general inquiry to the caregiver of the patient should be made, especially questions concerning the patient’s eating habits, bowel movements, and the duration of abnormal clinical signs and symptoms.
In most situations, a linear 5.0- to 7.0-MHz transducer is adequate for a pediatric abdominal sonogram due to the small body habitus of pediatric patients, with a curvilinear transducer used as needed. 18 The sonographic technique used to investigate the patient with suspected intussusception includes the use of graded compression. Graded compression refers to the act of pressing on the patient’s abdomen gently with the ultrasound transducer to distort the anatomy being evaluated. In theory, normal bowel is compressible, while abnormal bowel will typically not yield to compression, thus maintaining its shape. 18 Using this technique, the sonographer should analyze the entire abdomen and pelvis in both sagittal and transverse scan planes, keeping in mind that the majority of pediatric intussusception will be discovered in the right lower quadrant in the area of the ileocecal valve. The sonographer should also note free fluid within the pelvis, as well as any trapped fluid within the area of intussuscepted bowel, as these findings suggest compromised bowel. 20 Any area of bowel wall thickening should be thoroughly investigated. A pathological lead point for the intussusception may be found sonographically up to 66% of the time. 20
Color Doppler settings should include low-velocity flow and a low filter. 21 Color gain should be adjusted dynamically throughout the examination to maximize the visualization of blood flow. 21 Care should be taken in interpretation of color flow images to avoid mistaking color noise, or motion artifact due to patient movement, as blood flow. 21 Hyperemia may indicate inflammation in the affected segment of bowel. 18 However, a study by Kong et al. 21 found that color Doppler is often not seen in cases of intussuscepted bowel of more than 48 hours’ duration, likely due to vessel compression from increased edema. Absence of blood flow is indicative of gangrenous change, although the presence of flow on color Doppler does not preclude the presence of gangrenous tissue. 21
The sonographic appearance of intussusception has been thoroughly documented and described. These descriptions of intussusception include “doughnut,” “target,” “bull’s eye,” “crescent in a doughnut,” “sausage-shaped,” “sandwich,” “pseudokidney,” “coiled spring,” and “sleeve-like shape.”3,5,6,16 While the “doughnut,” “target,” “bull’s eye,” and “crescent in a doughnut” signs have been used to describe the appearance of intussusception in the transverse scan plane, the others have been used to describe the appearance of intussusception in the longitudinal plane. However, when analyzed closely in the transverse plane, the concentric bands of mucosa, submucosa, and muscularis of the intussusception take on the appearance of a cinnamon bun. The “cinnamon bun” sign describes the alternating hypoechoic and hyperechoic bands of tissue that are produced by the intussusception (Figures 2 and 3). 18 With compression, the cinnamon bun–shaped mass should not distort, while normal bowel will be compressible. Color Doppler can be used to evaluate for areas of hyperemia, around and within the intussusception, which can indicate vascular compromise (Figure 4).
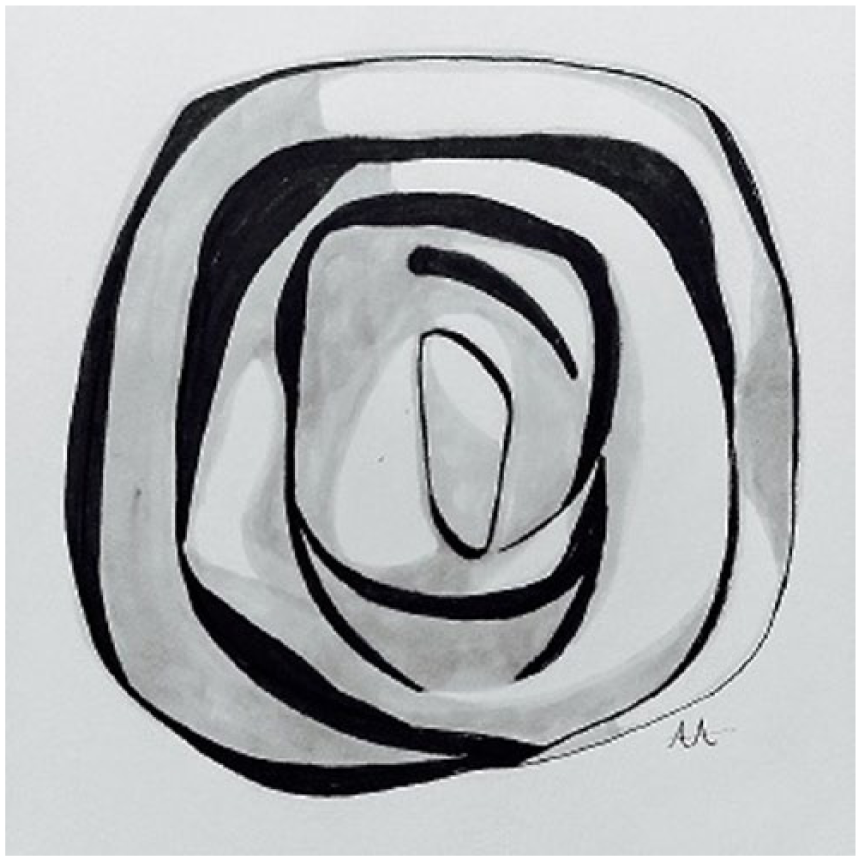
Drawing of the cinnamon bun sign. Here the illustration is depicting the transverse section of an intussusception, represented by “C” in Figure 1. Drawing by Alicia Arellanes.
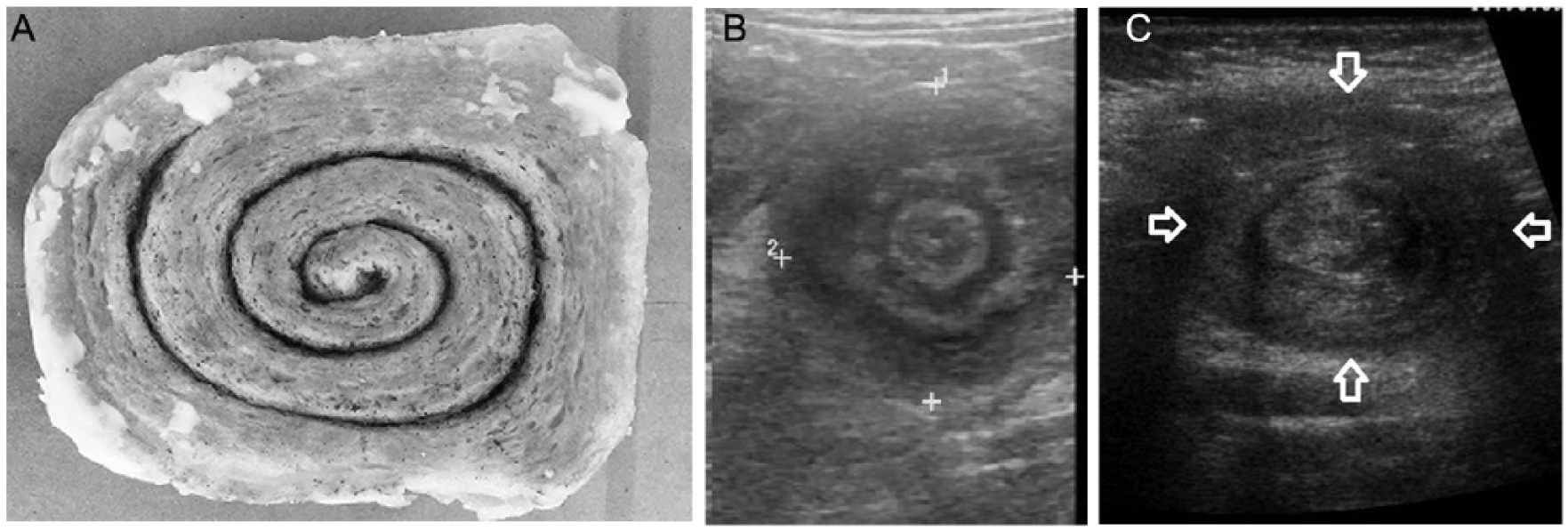
(A) Comparison image of a cinnamon bun. (B, C) Transverse sonographic images of an intussusception reveal the “cinnamon bun” sign (between calipers and arrows). Image B courtesy of Dr. Maulik S. Patel, Radiopaedia.org, rID: 9265. Image C courtesy of Dr. Jeremy Jones, Radiopaedia.org, rID: 8042.
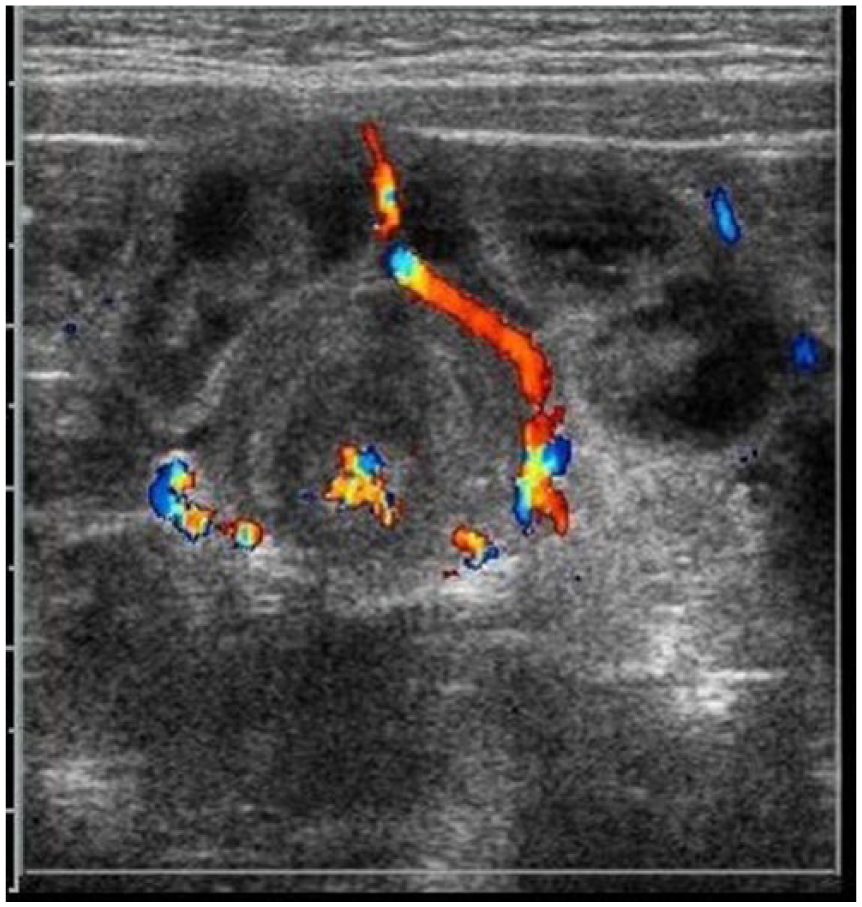
Intussusception with color Doppler, indicating hyperemic blood flow. Blood flow is noted around the intussusception and within the central portion of the abnormality.
Sonography is considered by some to be the present first-line modality used to evaluate pediatric patients for suspected intussusception, as it has been proven to be a safe and reliable technique, especially when the examination is performed by a competent professional.5,22 Kang and Peters, 5 Newman et al., 16 and Verma et al. 22 found sonography to have a high degree of accuracy, with a sensitivity between 97% and 100% and a specificity from 88% to more than 97%. A review by Manson 20 found sensitivities and specificities of “almost 100%.” It is often preferred over other modalities due to its low number of false-positive results, lack of ionizing radiation, and its ability to rule out other potential pathologies.5,22 Nonetheless, and potentially secondary to operator experience disparity, as well as a small sample size, a study conducted by Honjo et al. 1 found that the accuracy of sonography could be as low as 50%. 1 Computed tomography (CT) and colonoscopy can also be used for diagnosis, with data from Honjo et al. 1 and Kang and Peters 5 showing a higher rate of accuracy than sonography, at nearly100%. Contrast enemas were previously used as the diagnostic method for intussusception but currently are only used for therapeutic reduction. 22
Some pitfalls of sonography as a diagnostic modality include the broad range of clinical symptoms that can occur with intussusception, including cases of transient intussusception, which may resolve between imaging and surgery.8,22 In addition, a range of other conditions can mimic the appearance of intussusception, including a feces-filled colon, enterocolitis, volvulus, inflammatory bowel disease, psoas hematoma, and edematous, hemorrhagic, or otherwise thickened bowel.16,22
Complications and Treatment
Early diagnosis and treatment of intussusception is essential because of the risk of mesenteric imprisonment and vascular compromise. 23 As the pathophysical process of intussusception progresses, the affected bowel becomes partially or completely obstructed. 19 Mesenteric vessels ultimately become compressed between the affected bowel layers. 19 Untreated, vascular compromise progresses to bowel ischemia and necrosis. 19 The consequences of this disease process are severe and include bowel perforation and even death. 6
Although the consequences of untreated intussusception can lead to fatalities, Manning and Little 19 found that the mortality rate of intussusception in children in developed countries is less than 1%. The treatment depends on the presence of any underlying disease process or malignancy, as well any associated inflammation, edema, or ischemia, and the location and extent of the intussusception. 1 Due to the lower likelihood of malignancy, most childhood cases can be managed nonoperatively. 3 Treatment for intussusception in children is increasingly via barium hydrostatic reduction. 2 Enemas have been the preferred method for treatment in the United States since 1948, with a reported success rate between 60% and 90%. 19 While gravity-fed enemas were historically used, air reduction with the occasional addition of barium is the current method. 19 It now is hypothesized that the pressurized air more easily separates the bowel layers without added contrast. 19 Late symptoms seen in children with untreated intussusception include metabolic acidosis, hypotension, peritonitis, and an altered mental state. 19 Surgical treatment is more likely required when these symptoms are present. 19
Conclusion
Early diagnosis and treatment of intussusception are essential to not only subdue symptoms but also subvert potential devastating sequelae. Sonography can play a dynamic and decisive role in the identification of intussusception, especially for the pediatric patient. With this in mind, the sonographic investigator should be motivated to learn more about this disorder, and the use of a single, simple descriptive sign, such as the “cinnamon bun” sign, can aid in the diagnosis of this serious condition. Sonographers should take particular care in evaluating pediatric patients with abdominal pain, especially those under 36 months of age, for intussusception. Ultimately, sonographers should strive to have a systematic understanding of the presenting features and sonographic findings of intussusception to deliver unique, first-rate patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.