
Abstract
The objective of this study was to investigate the concordance of measurements for early postpartum endometrial thickness between magnetic resonance imaging (MRI) and transcutaneous diagnostic medical sonography (DMS) as well as its implications. The measurements of early postpartum endometrial thickness were reviewed across 51 postpartum women who underwent MRI and transcutaneous DMS. Additionally, 30 women with a normal menstrual cycle formed a control group, and their data were compared. The results indicated that the endometrial thickness at early postpartum was 4.63 ± 0.62 mm on MRI and 8.18 ± 4.70 mm on DMS, with a comparative significant difference (P < .001). The endometrial thickness of the control group was 10.02 ± 1.71 mm on MRI and 10.17 ± 1.81 mm on DMS with no comparative significant difference (P = .124). This cohort study questions whether the hyperechoic zone in the early postpartum uterine cavity represents the actual endometrial thickness. Care should be taken by sonographers in labeling the hyperechoic zone in the early postpartum stage as endometrium.
An endometrial thickness measurement is an important parameter for a female endocrine evaluation in clinical practice. Diagnostic medical sonography (DMS) has been used widely for obtaining an endometrial thickness measurement and has been proved to be accurate and reproducible compared with magnetic resonance imaging (MRI), computed tomography (CT), and histological studies.1–8 However, marked discordance between MRI and DMS measurements of postpartum endometrial thickness occurs frequently in clinical practice, and the published sonographic measurements for postpartum endometrial thickness in the literature is rather inconsistent.9–18 It is hypothesized that the measurements of postpartum endometrial thickness utilizing DMS may have not been properly assessed. There doesn’t appear to have been a study conducted on measurement accuracy of early postpartum endometrial thickness. The purpose of this study was to investigate the concordance of measurements of early postpartum endometrial thickness between MRI and transcutaneous DMS as well as its implications.
Patients and Methods
Study Population
A retrospective study on concordance of measurements of early postpartum endometrial thickness between MRI and transcutaneous DMS was conducted following Institutional Review Board approval. Archived medical records of 7148 puerperal women in a tertiary hospital were reviewed between May 2007 and September 2017. To obtain an adequate qualified sample, the following inclusion criteria were adopted: puerperal women who underwent both a DMS examination and a MRI study of the pelvis within 72 hours of delivery. The exclusion criteria used for the study were: puerperal women who underwent both a DMS and a MRI study more than 72 hours after delivery, or a DMS and a MRI study that exceeded an eight-hour interval (given that the uterine cavity might have undergone change), or the endometrium or presumptive endometrium was difficult to identify on DMS and/or MRI, or the presence/suspicion of retained products of conception, or the presence of anechoic or hypoechoic materials in the measuring uterine cavity (except cervical canal), or the presence of gas within the endometrial cavity that would produce sonographic foci shadowing, or lack of a MRI examination, or congenital uterus deformity, or multiple pregnancy, and postpartum endometritis. As a result, 51 postpartum women’s records were included in the study with 7097 postpartum woman records excluded.
To compare the difference and agreement of DMS and MRI in the evaluation of uterine endometrium among these women and their postpartum endometrial hyperechoic zone, a study was executed. To strengthen the study, a control group of normal female records was selected. The control group was comprised of 30 female volunteers with normal menstruation and no abnormal finding in uterus and adnexa. This sample was selected from 300 volunteers who underwent DMS and MRI for pelvic or abdominal evaluation.
DMS Examination
The sonographic examination was performed by 5 radiologists who had 4 to 20 years of experience conducting obstetrics and gynecology sonography. The equipment types used to gather uterine measurements were: Voluson expert 730 (GE Healthcare, Piscataway, NJ, USA), Logiq 9 (GE Healthcare, Waukesha, WI, USA), ProSound α 10 (Hitachi Aloka Medical Ltd, Tokyo, Japan), Acuson S2000 (Siemens Medical Solutions USA, Inc, Malvern, PA, USA), Voluson E8 (GE Healthcare, Zipf, Austria). All DMS examinations were completed with a curvilinear transducer with a frequency of 2 to 6 MHz. All the equipment used was adjusted to the gynecology preset, which adjusted the gain of the gray-scale, the time-gain compensation, and the focal zones accordingly so that the region of interest was displayed clearly.
Measurements of the uterus were taken with transcutaneous 2D DMS, in the midsagittal and axial planes, with the urinary bladder being slightly or moderately distended. Measurements of the endometrial thickness were taken with 2D DMS in the midsagittal plane at the largest width of the endometrium, in accordance with the cited literature.1,7,10,11,15 Doppler imaging was used to evaluate blood vessels in the uterine cavity in all women. All representative images obtained by DMS and Doppler imaging were saved in the Picture Archiving and Communication Systems (PACS) for retrospective review.
MRI Examination
After the DMS evaluation, undetermined cases as well as diagnostically complex cases (suspected placenta increta, placenta accreta, ovarian torsion, and other conditions) were evaluated by using MRI (Signa Excite Xl Twin Speed 1.5T system, GE Healthcare, Milwaukee, WI, USA). Gadodiamide, a MRI contrast agent, was injected for enhanced imaging. Measurements of the endometrial thickness were taken in the midsagittal plane at the largest width of the endometrium on T2-weighted MRI images, based on the published reference criteria.1,2 For those women with a distended cavity, the width of the endometrium was assessed based on two layers of endometrium. The MRI images of the women’s uterus were also saved to the hospital PACS for retrospective review.
Image Interpretation
The DMS and MRI images were retrieved and sorted from the PACS and saved into separate folders by three junior radiologists, who were not responsible for interpreting the cases. The DMS and MRI images were evaluated and interpreted by two senior radiologists in the sonography clinical area and one radiologist in MRI. Thickness of the endometrium on the MRI images was measured at the time of the research study; however, the thickness of the endometrium on DMS was retrospectively acquired from previous study.
Statistical Analysis
Because the DMS and MRI images were evaluated and interpreted in agreement by two senior radiologists in sonography and one radiologist in MR imaging, an interobserver agreement was not completed. Statistical analyses of the measurements of endometrial thickness between DMS and MRI in the postpartum and control group were performed with paired-samples t test using SPSS 20 (SPSS, IBM, Armonk, NY, USA), and a P < .05 was set a priori.
Results
The study puerperal women ranged in age from 22 to 38 years, with a mean age of 33.3 years. The control group of women ranged in age from 19 to 42 years (mean = 33.3 years). The data collected on the puerperal women included gravidity, parity, unique patient history, gestational age at delivery, mode of delivery, performance of manual exploration of the uterine cavity, birth weight, and neonatal condition. Thirty-six of the puerperal women were primiparas, 12 delivered their second child, and 3 had parity of three or more. Gestational ages at delivery ranged between 35 and 41 weeks (mean = 38.2 weeks). Fifteen women had undergone normal vaginal deliveries, 16 had assisted vaginal deliveries (12 had vacuum extraction, and 4 underwent forceps deliveries), and 20 had cesarean deliveries. There were 3 women who delivered vaginally and had exploration of their uterine cavity. The infant birth weights ranged between 1876 and 4312 g (mean = 3342 g). The 51 women that were included in the study were followed clinically for 5 days to observe their postpartum uterine discharge. Upon review of the puerperal women imaging cases, none were found to have retained products of conception on image of MRI, which was consistent with the DMS findings. There was no discharge of retained products of conception, as part of the documented follow-up. Endometrial thickness of the postpartum participants was 4.63 ± 0.62 mm on MR image (range, 3.7–6.0) and 8.18 ± 4.70 mm with DMS (range, 1.60–18.00), with a significant difference between them (P < .001). Endometrial thickness of control group was 10.02 ± 1.71 mm with MRI (range, 3.7–6.0) and 10.17 ± 1.81 mm with DMS (range, 1.60–18.00), with no significant difference between them (P = .124). Comparison of the measurements of endometrial thickness between postpartum participants and the control group of women based on DMS and MRI is listed in Table 1. Figures 1 through 3 demonstrate the measurements of endometrial thickness varied across conditions based on DMS and MRI images. Figures 4 and 5 show the scatter plot characteristics based on the measurements of normal endometrial thickness and postpartum endometrial thickness, utilizing DMS and MRI images.
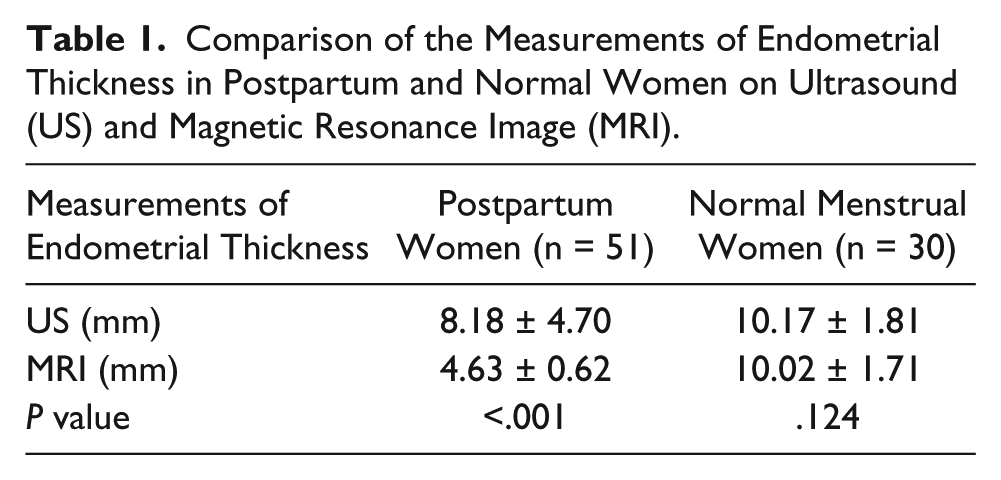
Comparison of the Measurements of Endometrial Thickness in Postpartum and Normal Women on Ultrasound (US) and Magnetic Resonance Image (MRI).
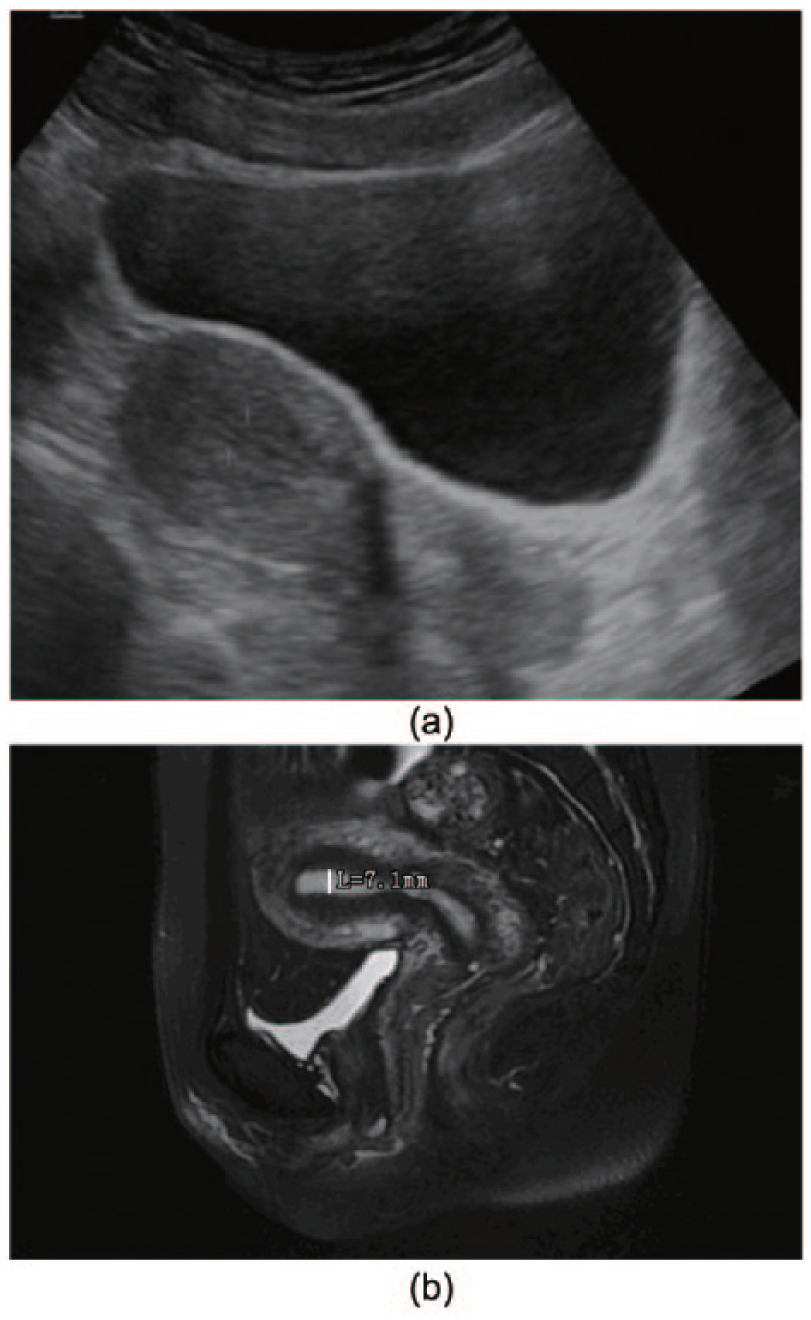
(A) Thirty-six-year-old woman with normal uterus and menstruation. Sagittal diagnostic medical sonography image of the uterus obtained during the proliferative phase, the endometrium presents trilaminar appearance, and thickness is 7.6 mm (between cursors). (B) Sagittal T2 magnetic resonace image of the normal uterus. The endometrium provides a high signal, thickness is 7.1 mm, the low signal layer immediately outside is the junctional zone, and the myometrium has an intermediate signal.
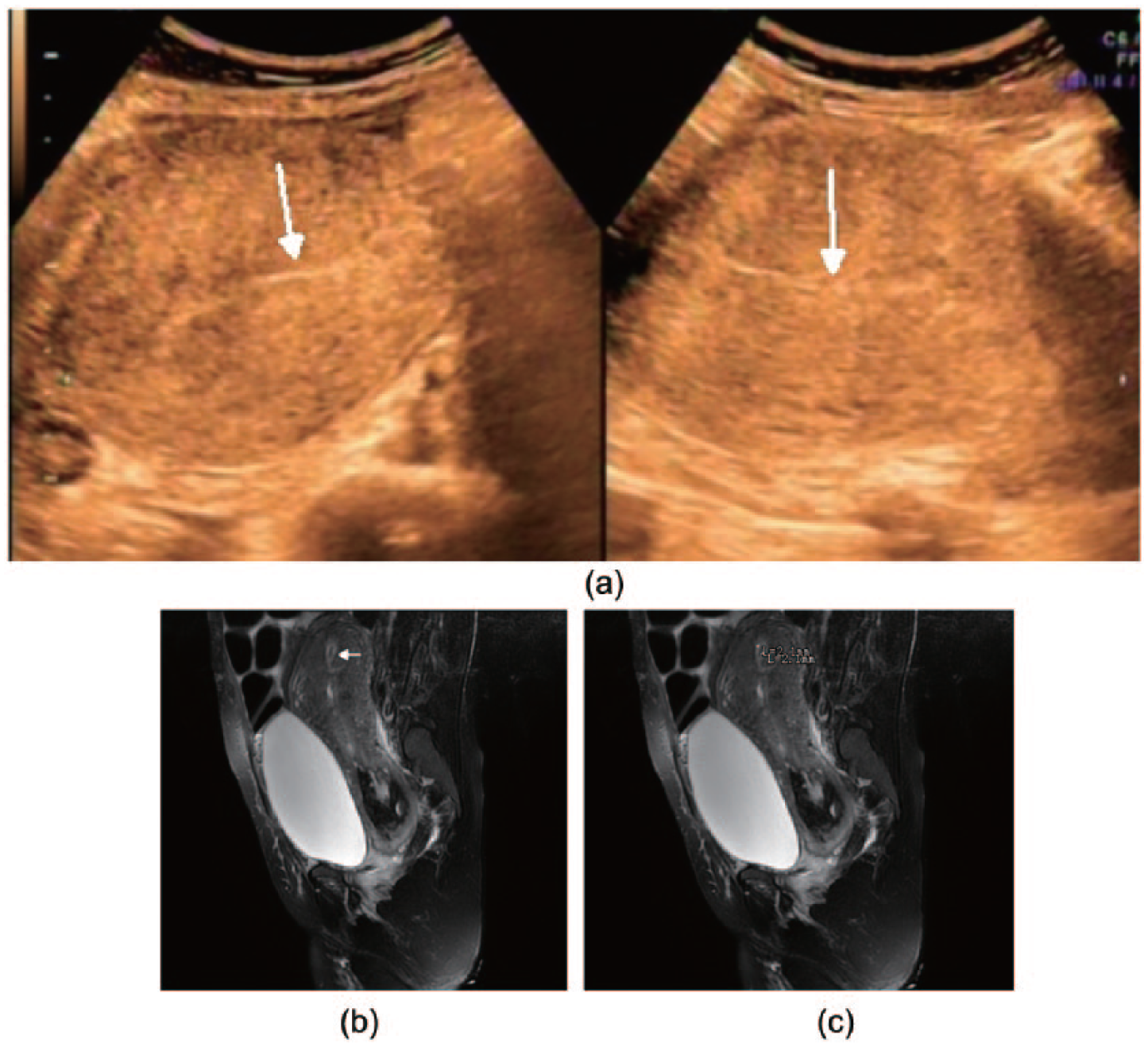
(A) Twenty-seven-year-old woman after cesarean delivery in 23 hours with postpartum uterus. Sagittal transcutaneous sonogram shows echoic endometrial cavity assumed as endometrium (arrow). (B) Sagittal T2 weighted magnetic resonance image shows the uterus cavity distended with low signal fluid and debris (arrows). The endometrium is thin (between 1.7 and 2.2 mm), appearing high signal outside the low signal. (C) Contrast-enhanced Sagittal T1-weighted magnetic resonance image shows the uterus wall has been enhanced, appearing intermediate high signal, and the endometrial cavity presents well-defined homogenous markedly low signal indicating there is fluid and debris in cavity between endometrial layers (arrows).
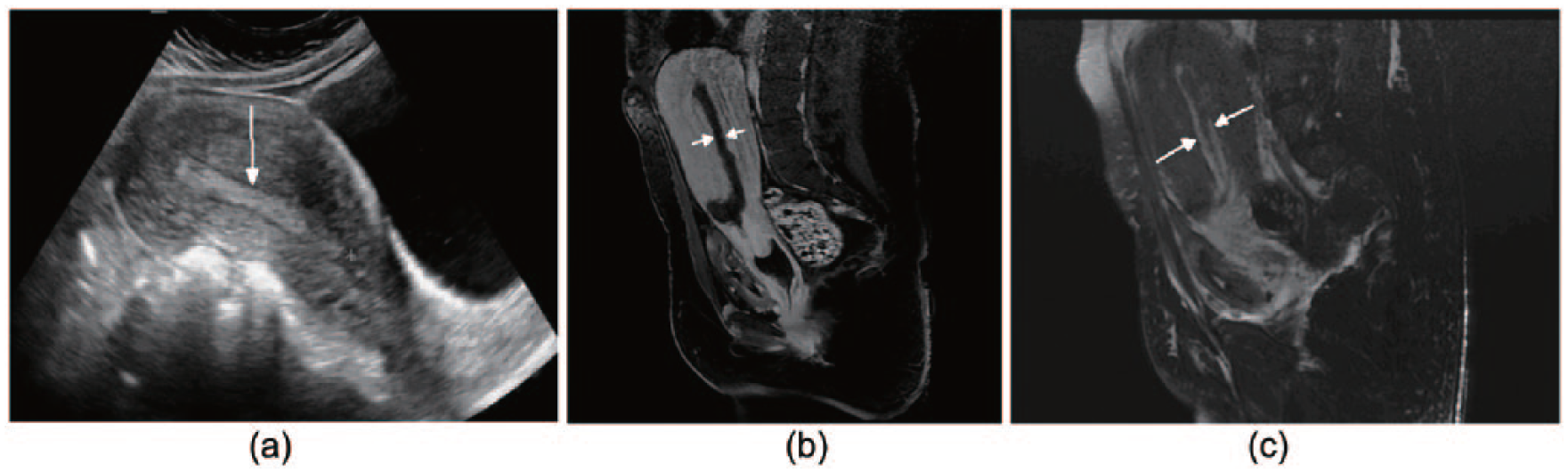
(A) Thirty-one-year-old woman with placenta increta after vaginal delivery in 70 hours. Sagittal and axial transcutaneous sonogram shows slight hyperechoic thin stripe (arrows) in endometrial cavity assumed as endometrium, and thickness is 1.6 mm. (B) Sagittal T2 weighted magnetic resonance image shows the uterus cavity is slight distended with low signal materials (arrow). The endometrium is thin, appearing high signal outside the low signal. (C) Sagittal T2 weighted magnetic resonance image shows the uterus cavity is slight distended with low signal materials. The endometrium is thin, appearing high signal outside the low signal, and thickness is 4.2 mm.
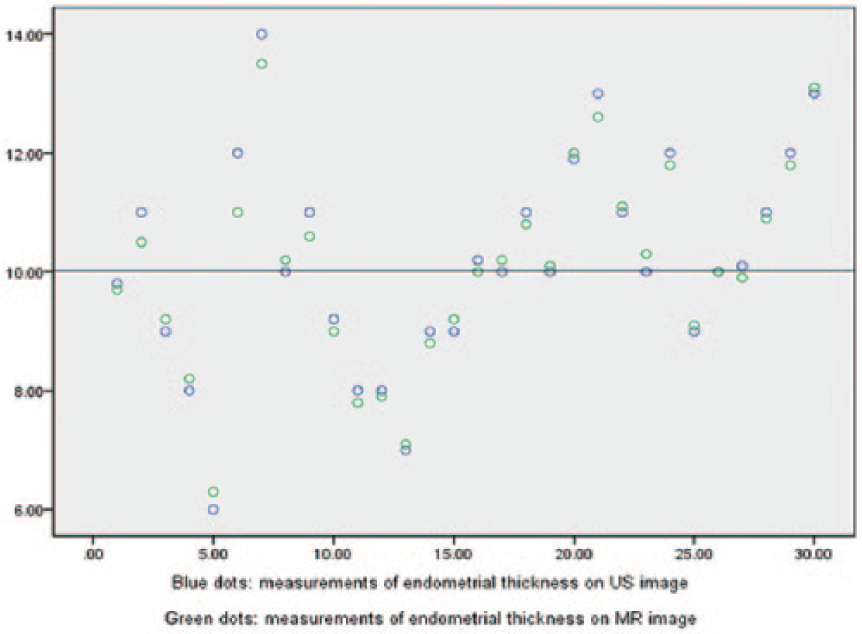
Scatter plot shows the measurements of normal endometrial thickness on diagnostic medical sonography image and mangetic resonace image. The measurements on mangetic resonace image and on ultrasound are discrete, and they are closely paired and concordant except in five cases.
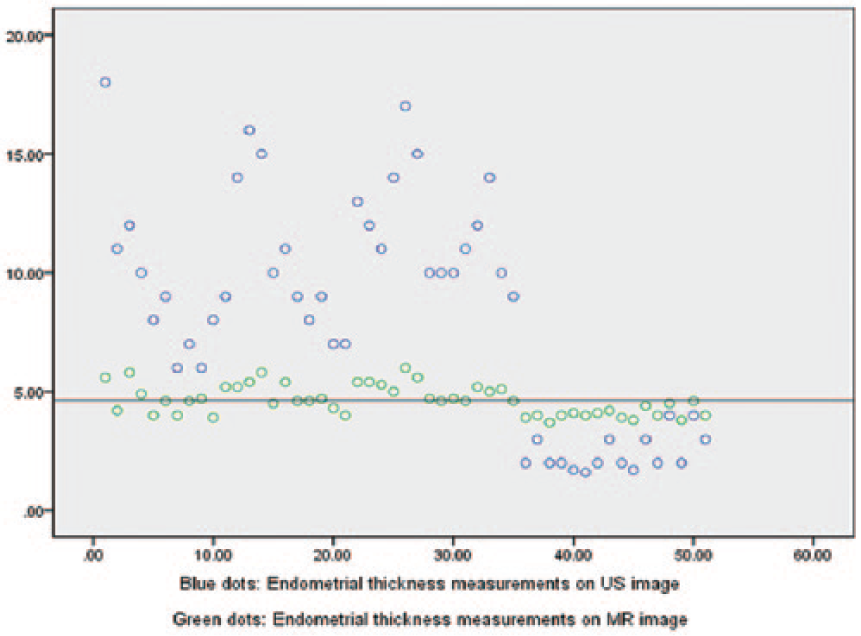
Scatter plot shows the measurements of postpartum endometrial thickness on diagnostic medical sonography image and mangetic resonace image. The measurements on the mangetic resonace images are converging, on diagnostic medical sonography are discrete, and they are almost not paired.
Discussion
Accurate measurement of endometrial thickness plays an important role in the clinical practice of gynecology, obstetrics, and internal medicine. This measurement also provides indispensable information for the purpose of evidence-based diagnosis and further management.4–18 Previous studies on the evaluation of the postpartum uterine cavity have focused mainly on the retained products of conception (RPOC) instead of the dimensions of the actual endometrium.9–17 Weissmann-Brenner et al. 9 reported that mean endometrial thickness is 8.1 mm (range, 2.8–28 mm) within 48 hours of delivery; in contrast, Koskas et al 10 reported that endometrial thickness had a mean endometrial thickness of 13 ± 2 mm at one to three hours after delivery. This is in comparison to a study conducted by Sokol et al., 13 which reported that the endometrial stripe thickness of postpartum patients was 11 ± 6 mm within 48 hours of delivery; a study conducted by Fuller and Feldman 11 described that in their patient cohort, the mean endometrial cavity measurement was 11.5 ± 3 mm; however, their values were inconsistent and believed to be due to the presence of echogenic material in the endometrial cavity. Unfortunately, clinicians remain unsure as to what the proper parameters should be for these postpartum women. Other studies of patients with RPOC were evaluated to attempt to clarify how to measure the endometrium with and without this condition. Ustunyurt et al 12 reported that when an endometrial thickness of 13 mm was chosen as the diagnostic cutoff level for RPOC, it had the best diagnostic clinical performance. However, Abbasi et al. 17 conducted a similar study but concluded that endometrial thickness more than 8 mm (utilizing DMS) could not be used to differentiate RPOC from deciduas and suggested that an endometrial thickness of greater than 8 mm in postpartum women is often a concomitant of actual endometrium and endometrial deciduas. In the present study, early postpartum endometrial thickness measured through transcutaneous DMS was either significantly higher or much lower than those measured on MRI images (4.63 ± 0.62 mm). It is important to note that in the present study, there was no RPOC noted on the images or in clinical follow-up, which differs from the aforementioned studies.9–17 Meanwhile, the measurements of endometrial thickness for the present control group compared between DMS and MRI imaging had good concordance and were consistent with the delineation by Nalaboff et al. 1 This would seem to indicate that measuring early postpartum endometrial thickness through transcutaneous DMS in a similar manner as measuring the endometrium of control group could lead to great clinical discordance. In this study, findings from the corresponding T2-weighted MRI images showed that there were women with early postpartum endometrial thickness on DMS that had actually included echogenic materials in the distending cavity apart from the actual endometrium, as illustrated in Figures 2A and 2B. This had not been identified on DMS as it wasn’t noted by the radiologist interpreting these studies. It would seem that the possible causes for discordance in measurements of early postpartum endometrial thickness with DMS could be attributed to the radiologists assuming that the echogenic zone in the center of the uterus was the endometrium.
Postpartum endometrium and other materials (deciduas, blood necrotic vessel ends, blood, etc.) in the uterine cavity can be diagnostically identified on MRI; however, it is believed to be more difficult with DMS.9–18 During sonographic examination, slight transducer compression of the examinee’s abdomen may reduce the space within the uterine cavity, therefore causing the echogenic materials condensed, mimicking the normal endometrium. The environment of the early postpartum uterine cavity is different from other physiological or pathological situations, which may bring varied echogenic patterns with DMS. The early postpartum uterus is much larger than the normal uterus, so the thicker uterine wall may compromise sonographic resolution and negatively affect the uterus and endometrial echogenicity. The early postpartum endometrium isn’t specifically classified to a particular phase of normal menstrual cycle. In early postpartum, just after labor, estrogen and other hormones produce modulation and fluctuation, which do not favor endometrial proliferation and secretion. Given this physiology, the thickness of the endometrium should not be thicker than that in proliferative and secretory phase of the menstrual cycle. The thickness of the endometrium in proliferative and secretory phase of the normal menstrual cycle is 5 to 7 mm and 7 to 16 mm, respectively.1–3 In this study, the mean thickness of early postpartum endometrium on MR image is 4.63 mm, which approaches the proliferative phase of control group and is in concordance with the aforementioned analyses. Accurate diagnosis requires that these factors be taken into account in addition to the clinical history and physical examination findings. There were 16 cases that the measurements of early postpartum endometrial thickness on DMS were lower than those on MRI imaging. One reason may be that the actual endometrium in early puerperal women is ambiguous and the echogenicity is not well defined; therefore, only those parts located near the interface can be identified with confidence on DMS. The concern is that these sonographic images and resulting measurements may not accurately represent the actual endometrium.
Although this study is retrospective, the clinical practice of evaluating the uterus and postpartum endometrium using DMS and MRI is a standard clinical protocol, and the measurements are assumed to be reliable. Transvaginal sonography is considered to provide much better resolution, but the uterus of early puerperal women is large and often cannot be visualized completely in this way. In addition, there may be some inconvenience to the vaginal approach for obtaining imaging, so abdominal DMS was routinely performed in these clinical sites.
Limitations
The limitations of this research were as follows: (1) The research design of this study is pre-experimental; therefore, it has threats to internal and external validity; (2) the retrospective design and the sonographic measurements were not a mean of several measurement attempts, which may hav the potential of harming measurement accuracy; (3) absent evaluation of interobserver agreement of the sonographers, but according to Kang et al., 3 the agreement among sonographers is high and usually doesn’t cause marked influence; and (4) absence of histopathological analysis.
The MR T2-weighted images delineate the uterine zonal anatomy, which has higher qualification to identify the uterine endometrium; therefore, measurements of it could begin to build a reference criterion. 2
Considering the limitations mentioned previously, the authors would suggest that a higher level study be conducted based on a prospective design, with multiple clinical centers, and based on a larger scale of postpartum women and patients.
In this particular study, the measurements of early postpartum endometrial thickness between transcutaneous DMS and MRI are substantially different. Taking the measurements on MRI images as reference resulted in the measurements based on transcutaneous DMS to be increased, while in some other cases, the measurements were decreased. The results of this study provide low-level evidence that the hyperechoic zone presumptive endometrium in early postpartum uterine cavity may not be the actual endometrium.
Conclusion
Caution should be exercised when evaluating the hyperechoic zone in the early postpartum uterine cavity. It is a concern that the DMS measurements may not represent the actual endometrial thickness. Sonographers as well as sonologists should be careful in labeling the hyperechoic zone (except in cases of retained products of conception) in the early postpartum uterine cavity as endometrium, and it is different from the DMS assessment for nonpuerperal uterus.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.