
Abstract
The prenatal diagnosis of congenital dacryocystocele has been reported using 2D sonographic imaging, but there are very few reports of the use of 3D sonography for this diagnosis. Two cases are presented in which 3D and Doppler sonography was helpful in determining the prenatal diagnosis. The embryologic basis of this obstruction of the nasolacrimal duct is discussed along with techniques for the prenatal diagnosis, including the potential value of 3D sonography in limiting the necessity of other prenatal testing. The importance of establishing the differential diagnosis is also discussed, as there is the possibility of the dacryocystocele being secondary to a sinonasal tumor.
Keywords
Congenital dacryocystocele or mucocele is a cystic obstruction of the nasolacrimal duct. It is considered a rare, benign finding that can be diagnosed prenatally only during the third trimester of pregnancy1,2 because of its embryologic basis.3–5 The development of the lacrimal drainage system begins around the sixth week of gestation. Canalization of the nasolacrimal pathway begins at about 12 weeks of gestation and is usually completed as early as 24 weeks. 6 Usually, the nasolacrimal duct becomes patent during the eighth intrauterine month of gestation, and if this does not occur, dacryocystocele might result. 7 The main cause of congenital dacryocystocele is atresia of the Hasner valve at the distal end of the nasolacrimal duct. 5
The lesion can be unilateral or bilateral and may resolve spontaneously antenatally 8 or in the postnatal period. Dacryocystocele is usually a benign lesion, but it may be also a marker of syndromes 5 or secondary to sinonasal cancer. 9 Differential diagnoses are of critical importance and include anterior encephalocele, nasal glioma, facial teratoma, dermoid cyst, hemangioma, rhabdomyosarcoma, and retinoblastoma. 5 The correct prenatal diagnosis of dacryocystocele plays a critical role with regard to alternative diagnoses that may influence prenatal management and prognosis. Many cases of dacryocystocele have been diagnosed prenatally with the aid of 2D sonography. Although 3D sonography might potentially reduce the need for complementary diagnostic tools in the postnatal period, very few articles have reported the use of both 3D and Doppler sonography in the diagnostic setting.
Case Series
Case 1
A primigravida woman in her late 30s with no history of consanguinity had a third-trimester scan at 32 weeks’ gestation. The patient had undergone genetic amniocentesis at 16 weeks with a normal karyotype. The second-trimester scan, performed at 20 weeks’ gestation, was normal. The third-trimester scan was carried out with a Voluson E8 (GE Medical System, Milwaukee, Wisconsin) using a transabdominal RAB 4- to 8-MHz probe. The following 2D sonography settings were used: harmonics, on high level; cross beam, 1; speckle reduction, 2; and dynamic contrast, 7. A mixture of gradient light 70/30 was used. Volume contrast imaging (VCI) was activated with a slice thickness of 2 mm to improve contrast resolution. A unilateral, isolated hypoechogenic mass measuring 15 × 13 mm, located in the medial portion of the canthus, was seen (Figure 1). Doppler examination was applied and revealed absent blood flow within the mass (Figure 2). Three-dimensional sonography with multiplanar volume rendering in the surface minimum mode confirmed the 2D sonographic diagnosis, and acquisition of fetal profile volume data sets was achieved during maternal apnea and fetal rest. Online and offline volume data set analysis resulted in a normal fetal profile. The neonate was delivered vaginally at term. Gestational weight was 3250 g with Apgar scores of 8 and 9 at one and five minutes, respectively. The diagnosis of congenital dacryocystocele was confirmed, and the lesion resolved spontaneously on postnatal day 14.
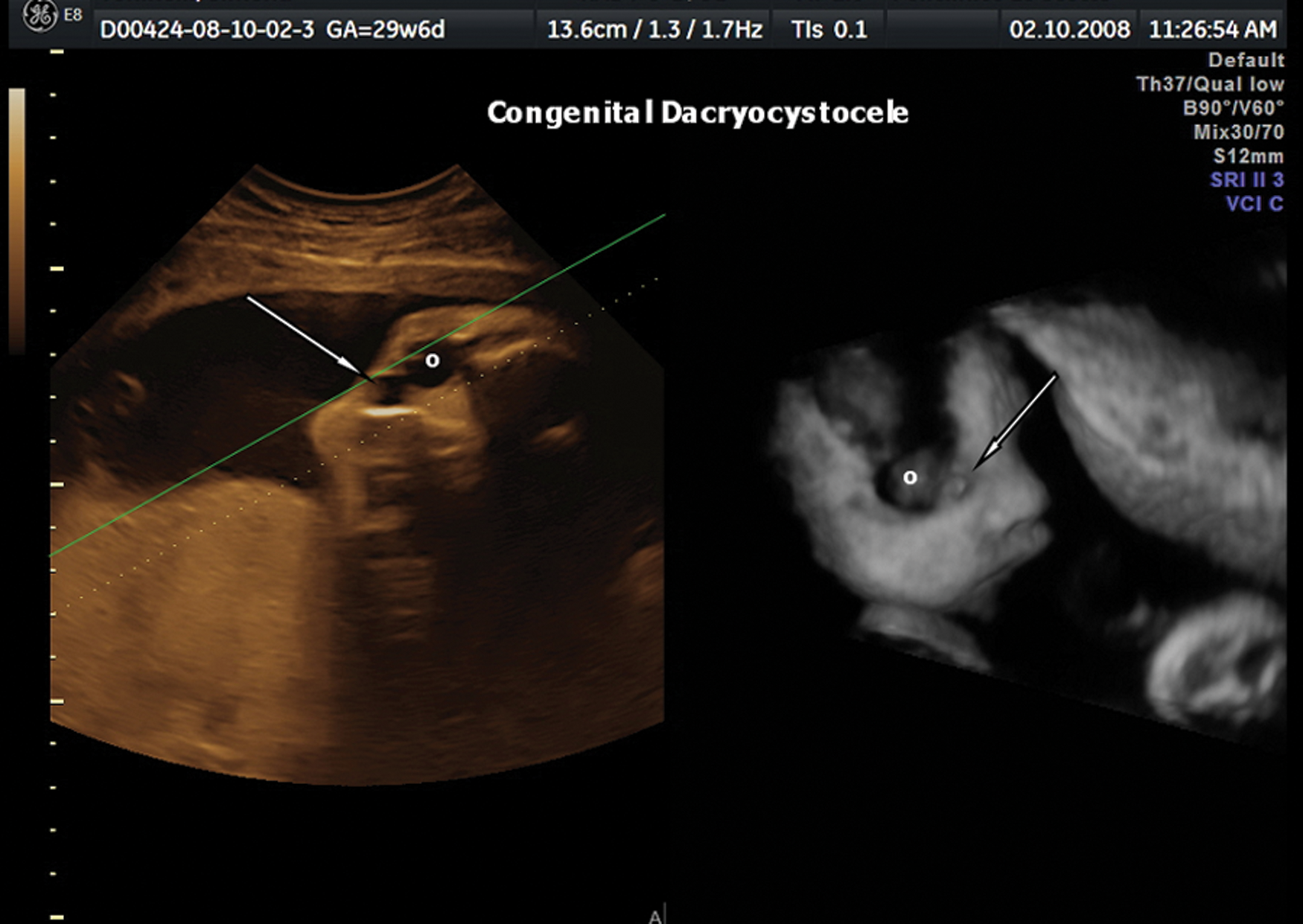
Three-dimensional sonography with volume rendering showing an anechogenic cystic lesion (white arrow) located on the medial right cathus and below the fetal orbit (o).
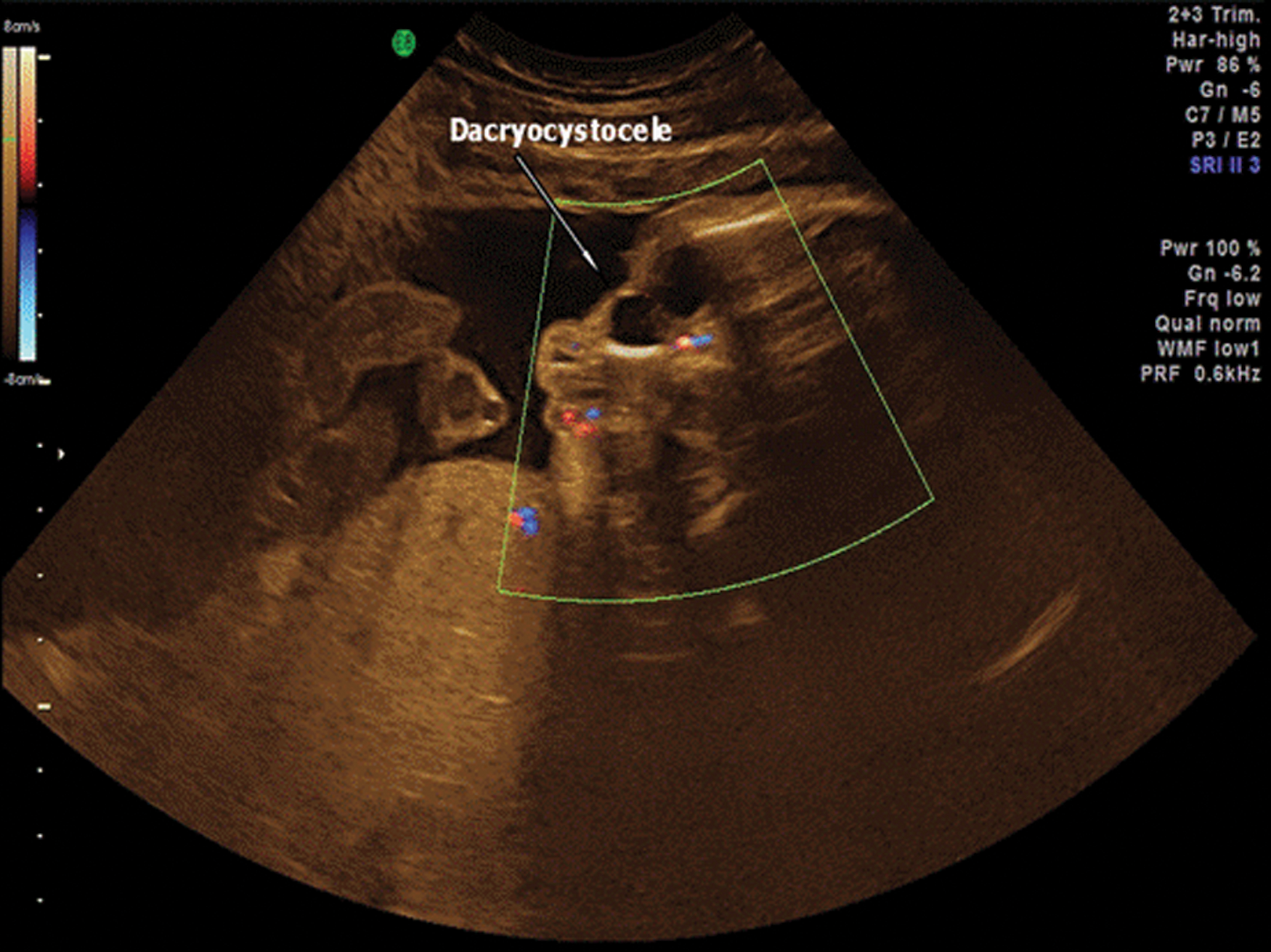
Three-dimensional Doppler sonography demonstrating absent blood flow within the cystic lesion.
Case 2
A primigravida woman in her mid 20s with no history of consanguinity had a negative first-trimester combined screening for Trisomy 21 (1:4561) and Trisomy 18/13 (1:5561) according to Fetal Medicine Foundation guidelines. A routine second-trimester sonographic examination was also negative. A third-trimester sonographic examination performed at 30.5 weeks’ gestation was carried out with the sonography system and 2D setting as described in case 1. Two-dimensional sonography showed bilateral, paraocular cystic masses, and a provisional diagnosis of dacryocystocele or possible dermoid cysts was made. Adjuvant 3D applications were then done with care taken to avoid fetal movements and shadow artifacts. The volume angle was set at 75°, and the scan quality was set at the maximum level. Using these settings, the 3D volume transducer swept mechanically over the defined region of interest (ROI), sampling between 95 and 255 (median, 227) consecutive slices per volume. Three-dimensional sonography with multiplanar volume reconstruction (Figure 3, Figure 4), tomographic sonography imaging with slices of ±1 mm (Figure 5), and an OmniView algorithm (Figure 6) were applied. The presence of isolated, bilateral cystic masses located on the medial portion of the canthus was confirmed after this 3D sonographic reconstruction. Magnetic resonance imaging was planned at 32 weeks’ gestation using a Philips Achieva 1.5 Tesla scanner (Philips, Eindhoven, The Netherlands) with a flexible surface coil. Multiplanar, single-shot, fast-spin echo, T2-weighted images were obtained at the level of the fetal head, with the following parameters: repetition time, 15,000 ms; echo time, 120 ms; field of view, 34 cm; echo train length, 140; matrix of 139 × 256; and slice thickness, 0.75 mm. Each pulse sequence lasted 30 s. No maternal or fetal sedation was required. Magnetic resonance (MR) imaging confirmed the presence of bilateral cystic masses in the medial portion of the canthus with a high and homogeneous signal on T2-weighted images. The MR imaging demonstrated all three components of the dacryocystocele anomaly: enlargement of the lacrimal sac, enlargement of the lacrimal duct, and intranasal cele, either in axial (Figure 7A–C) or in frontal planes (Figure 8A,B).
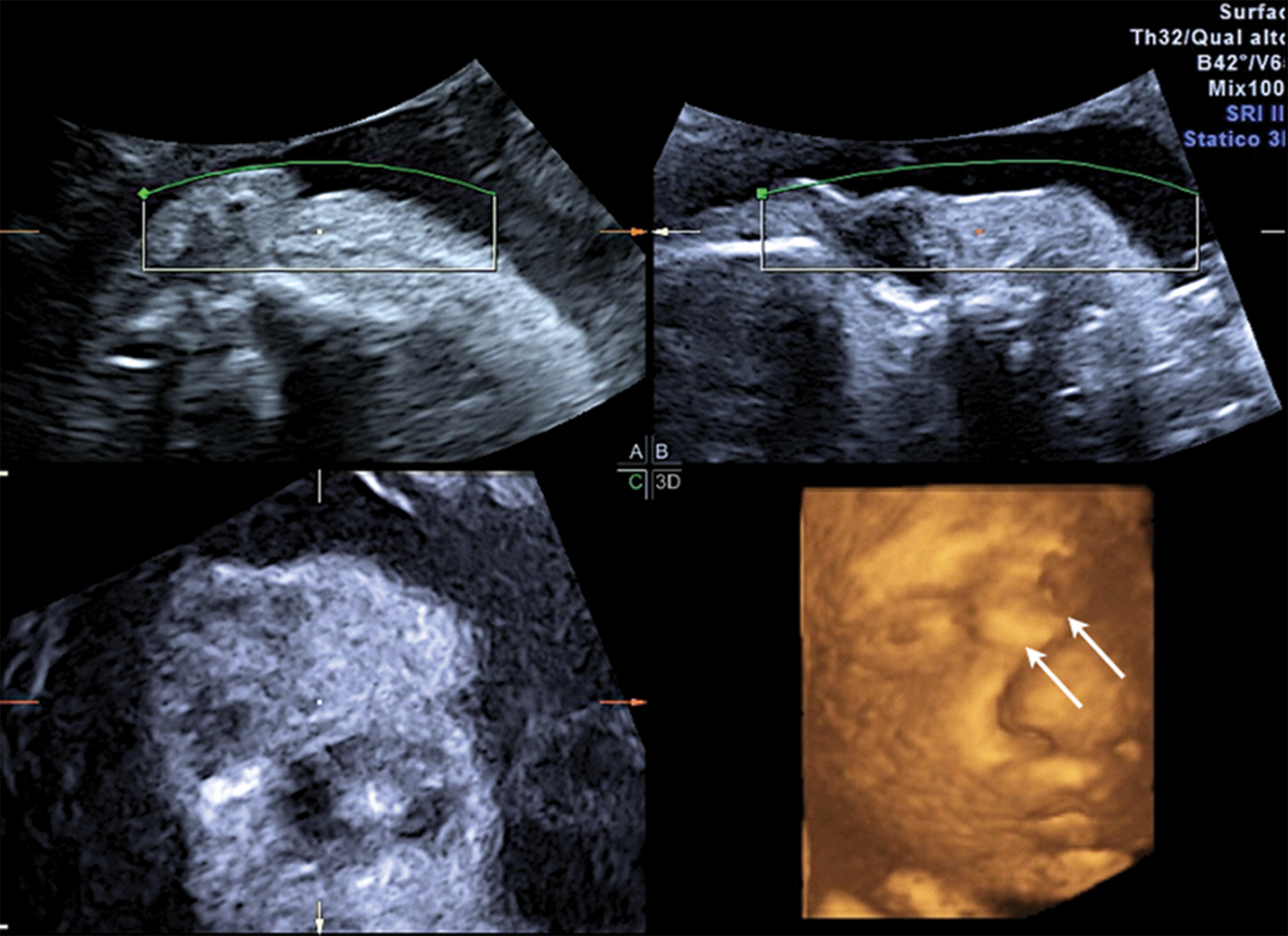
Three-dimensional sonography with volume rendering demonstrating bilateral congenital dacryocystocele (white arrows).
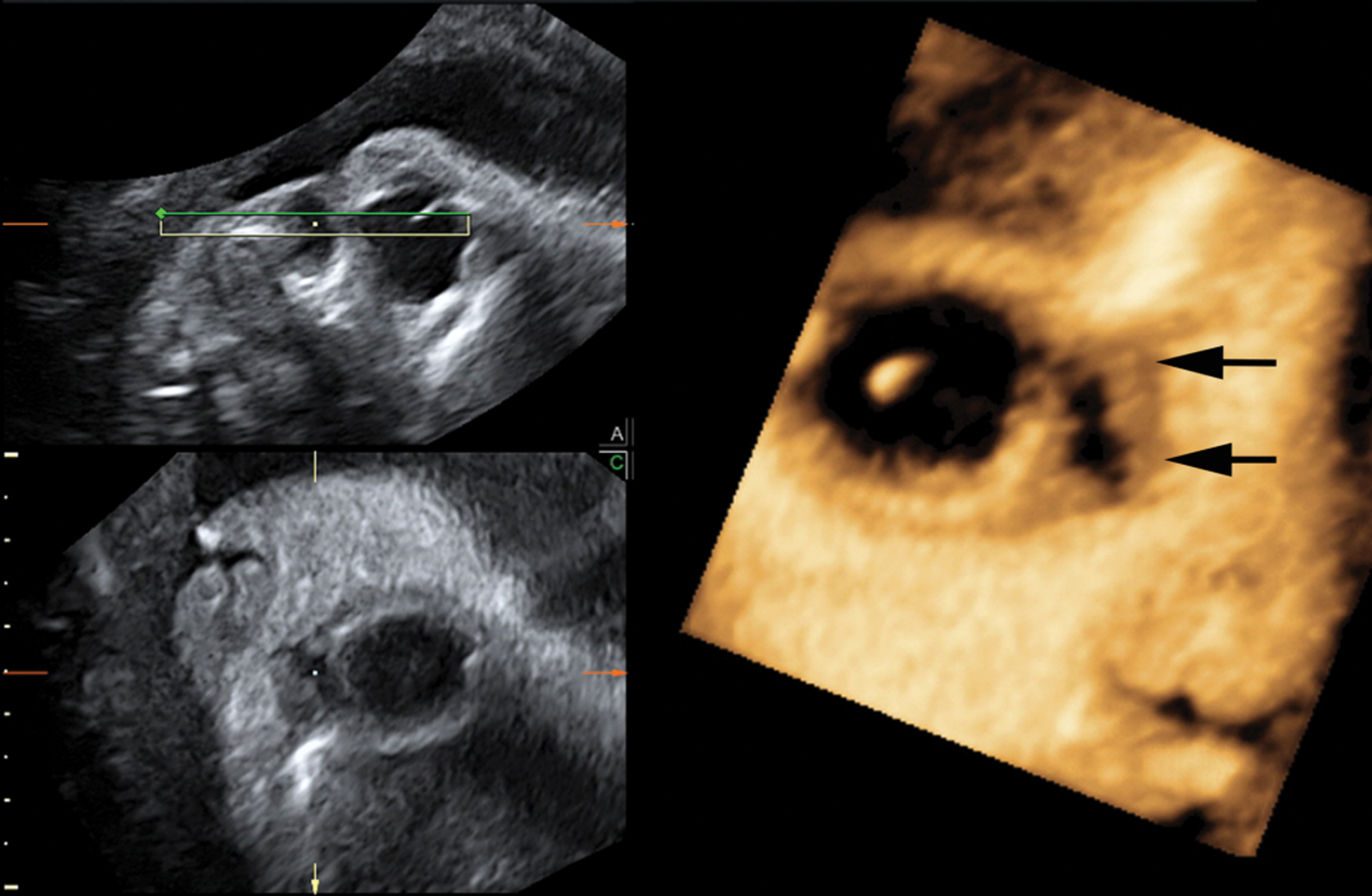
Three-dimensional scan in minimum surface mode clearly demonstrating absence of the lesion to the fetal lens. The cystic mass is located in the medial portion of the right canthus (black arrows).
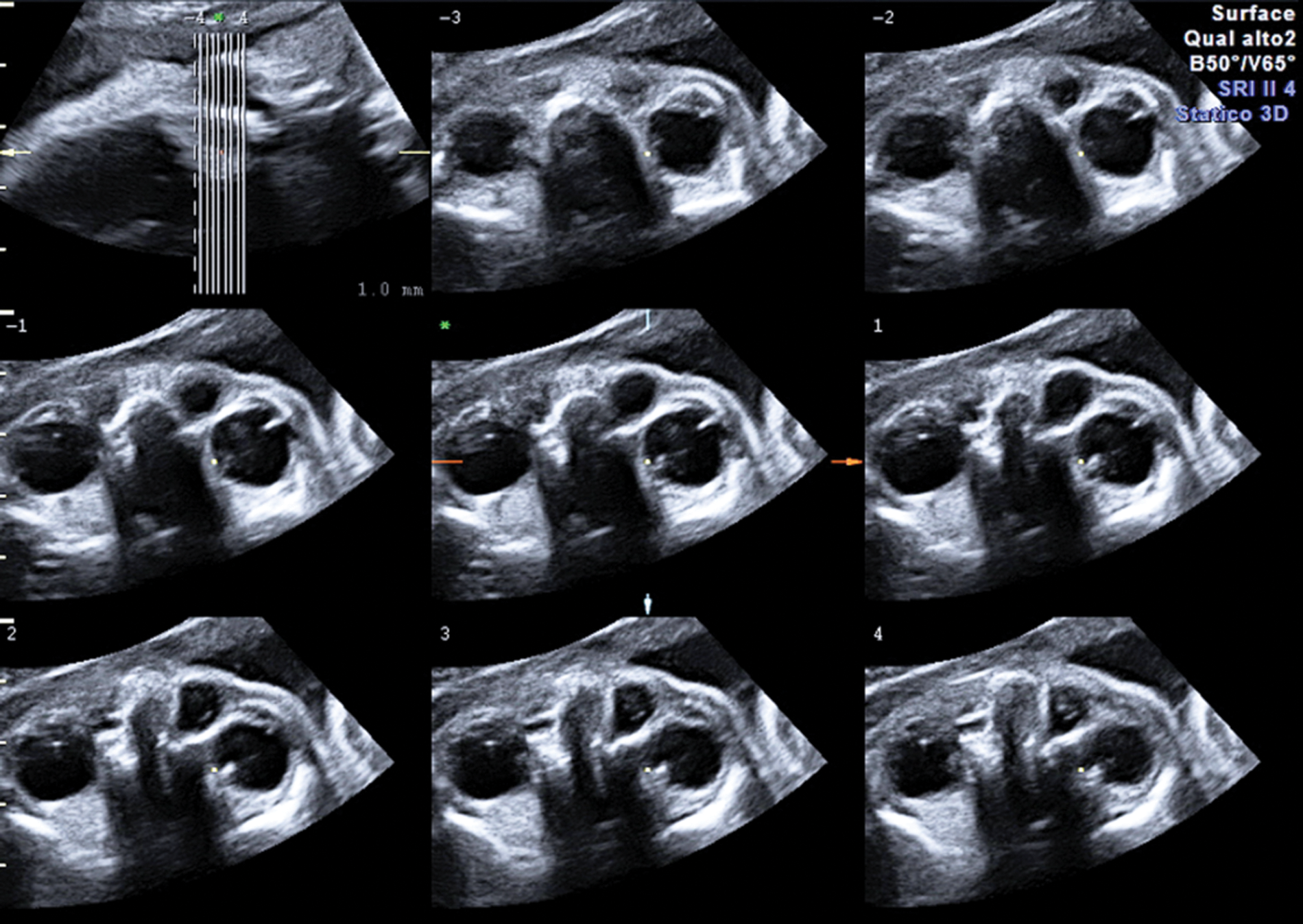
Tomographic sonographic imaging performed with slicing of 1 mm in the axial plane easily demonstrates the location and the relationship of the cystic mass with the surrounding anatomical structures.
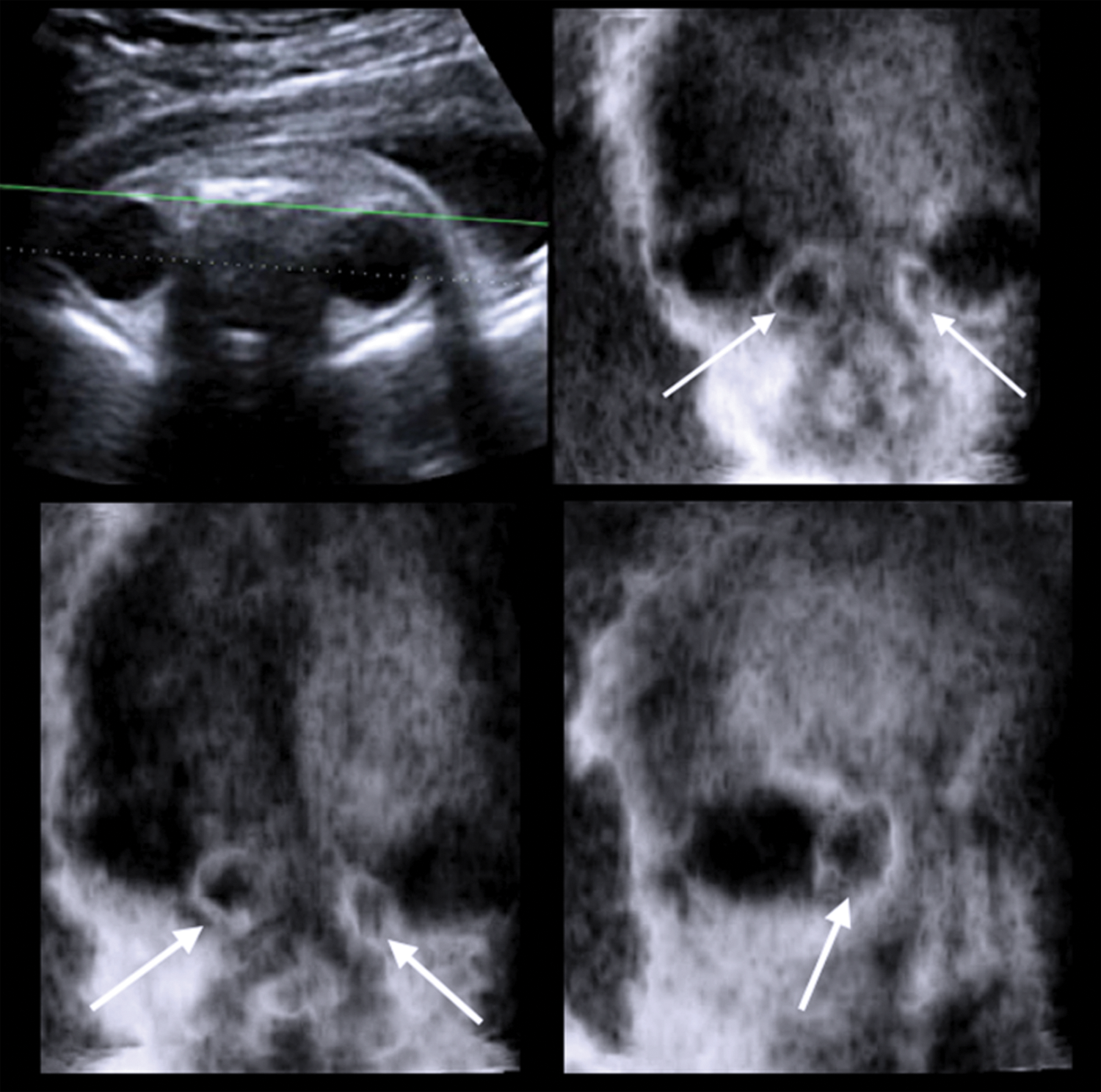
Three-dimensional sonography in the multiplanar modality using the OmniView algorithm (green line) easily demonstrates the cystic mass in the coronal planes (white arrows).
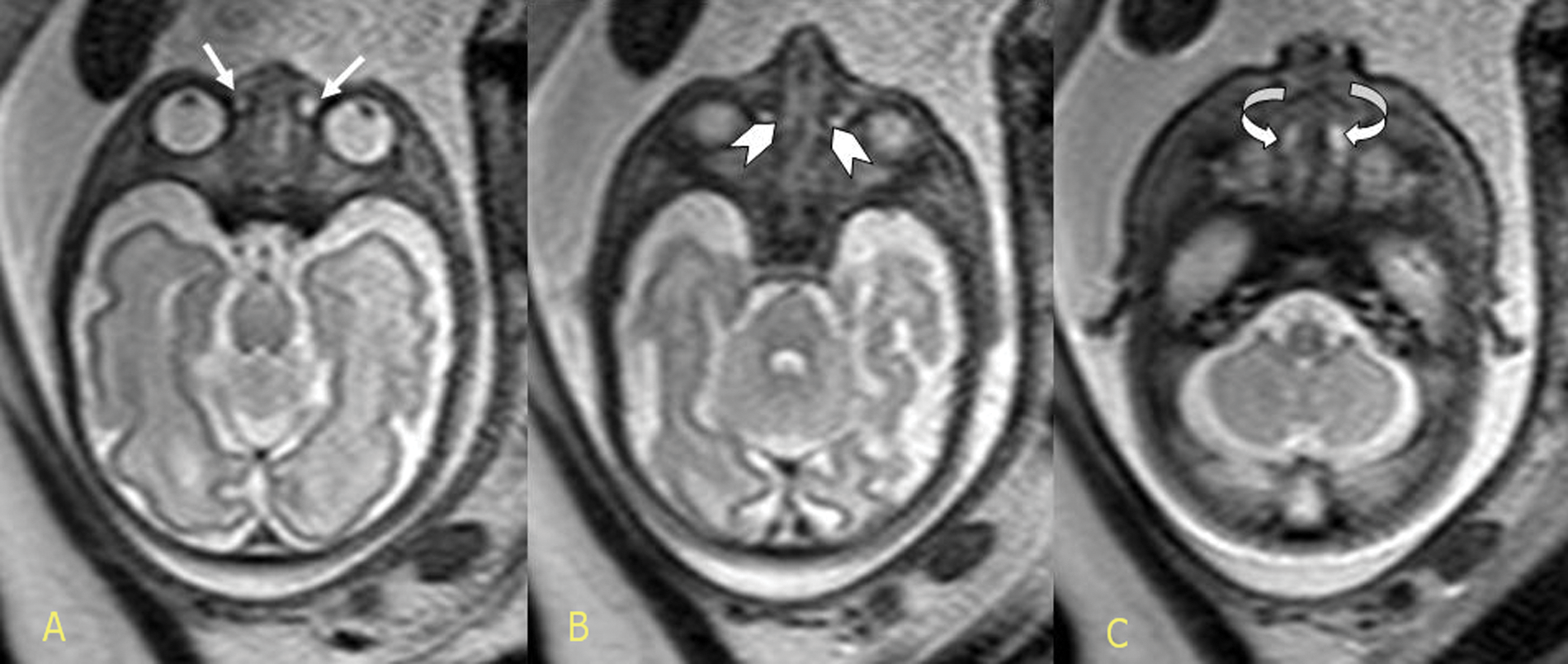
T2-weighted antenatal single-shot, fast-spin echo magnetic resonance imaging in the axial plane demonstrating all three components of the dacryocystocele anomaly: enlargement of the lacrimal sac (A), enlargement of the lacrimal duct (B), and the intranasal cele (C), respectively. The arrows represent intranasal mucocele.
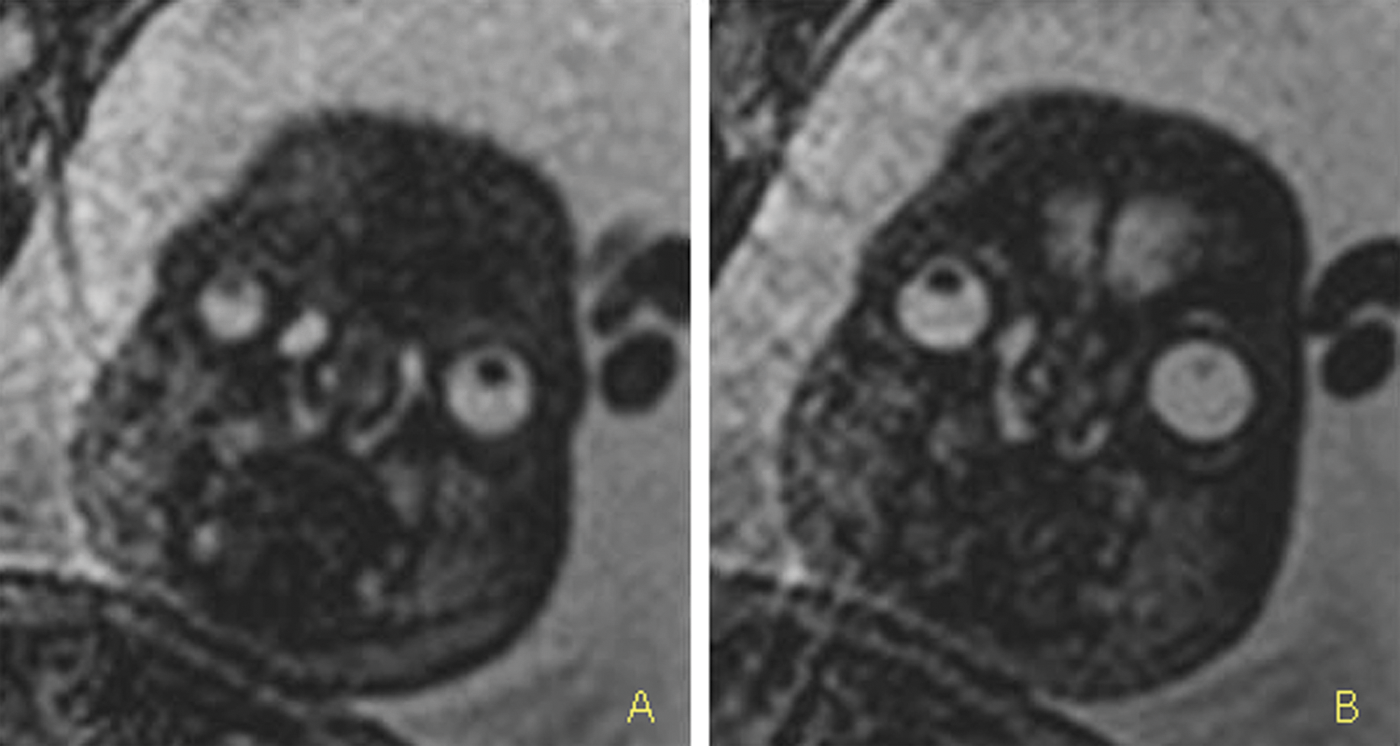
Antenatal T2-weighted single-shot, fast-spin echo magnetic resonance imaging in the frontal section: note the enlargement of the lacrimal sac, enlargement of the lacrimal duct (A), and the intranasal mucocele (B).
The follow-up examination, conducted at 34 and 38 weeks’ gestation, documented a regression and a spontaneous in utero resolution of the cystic masses. The neonate was delivered at term vaginally with normal Apgar scores at one and five minutes and was discharged back home on the third postnatal day with no complications.
Discussion
Embryology and Etiopathogenesis
The lacrimal drainage apparatus begins in the medial aspect of the orbit with two orifices, known as the superior and inferior puncta. These orifices drain into two canaliculi—namely, superior and inferior—which then form a common canaliculus. The valve of Rosenmuller, which lies at the junction of the common canaliculus and the lacrimal sac, prevents the reflux of tears back into the canaliculus. The lacrimal sac is located within the inferomedial wall of the orbit known as the lacrimal sac fossa. The nasolacrimal duct is a membranous canal extending inferiorly for about 18 mm from the nasolacrimal sac to the inferior meatus of the nasal cavity. 9 Congenital dacryocystoceles are a relatively rare variant of nasolacrimal duct obstruction (NLDO), accounting for only 0.1% of infants with congenital NLDO. 10 NLDO is a result of a blockage at the distal end of the nasolacrimal system at the valve of Hasner; dacryocystocele occurs when the mesoderm fails to canalize distally, and along with the distal obstruction, there is a functional or mechanical proximal obstruction. 6 Historically, dacryocystocele was thought to occur as a consequence of amniotic fluid trapped within the lacrimal system in utero, thus giving rise to the term amniotocele. 11
Sonographic Techniques and Prenatal Diagnosis
Any cyst in the lacrimal duct or lacrimal sac is most appropriately called a dacryocystocele because the term encompasses a continuum of anomalies. 12 Although the antenatal diagnosis of dacryocystocele has been reported using 2D sonography,3–5, 7,8, 13–19 the use of 3D sonography has been documented only in two cases previously.2,20 OmniView (GE Medical System, Zipf, Austria) is a new imaging modality for 3D–4D sonography that allows interrogation of volume data sets and the simultaneous display of up to three independent and nonorthogonal planes. Section planes are obtained by manually drawing lines selected from menu options as follows: line, curve, polyline, and trace. Moreover, OmniView enables operators to obtain virtual planes because curvilinear planes can be imaged. OmniView can also be used in association with VCI software (GE Medical System) that displays a thin slice from an acquired volume where the slice thickness can be adjusted to improve contrast resolution. This differs from more conventional tomographic sonography imaging, where volume data sets are automatically sliced and displayed in multiple images. In the cases presented, the axial plane was used to depict the enlarged nasolacrimal duct, which is considered an important criterion for the diagnosis. Tomographic sonography imaging provides information about the anatomy of the lacrimal pathway not otherwise obtainable at the time of examination. 21 Sepulveda et al. 2 reported 10 fetuses with a prenatal diagnosis of a congenital dacryocystocele at a median gestational age of 30.1 weeks (range, 27–33 weeks). The cystic lesion was unilateral in six cases and bilateral in four, with a mean largest diameter at the time of diagnosis of 7.5 mm (range, 4–11 mm). Three-dimensional sonography, carried out in three patients, clearly depicted the anomaly, the degree of intranasal extension, and swelling below the medial canthal area. Spontaneous resolution was documented prenatally in five fetuses, and one additional case resolved between the last prenatal scan and the delivery. The authors concluded that 3D sonography provides a noninvasive method for evaluating these cystic masses and may contribute to the avoidance of additional diagnostic testing in the neonatal period. The prenatal visualization of dacryocystocele raises the rare possibility of associated anomalies as the lesion can be a marker of a genetic syndrome such Canavan disease and polycystic kidneys. 5
Differential Diagnosis
Differential diagnoses include anterior encephalocele, nasal glioma, facial teratoma, dermoid cyst, hemangioma, rhabdomyosarcoma, and retinoblastoma. 5 Retinoblastoma may appear as a heterogeneous mass that arises directly from the eye and has an irregular echogenic structure surrounded by a sonolucent area covered by a membrane.22,23 Hemangiomas are heterogeneous masses that protrude from and typically form an obtuse angle to the skull. They exhibit significant blood flow within the lesion on color Doppler analysis. 24 Nasal teratomas usually have an outward direction that involve the tip of the nose without extension into the nose, nasal passages, or nasopharynx. 25 Nasal gliomas must be differentiated by their frontal encephalocele that usually involve the space directly above the nose 26 ; antenatal MR imaging may be of value in such cases by ruling out underlying bone defects.27,28 Dermoid cysts have a complex appearance on sonography with areas of calcifications frequently present. 29
Dacryocystocele may also be secondary to sinonasal cancer or may be related to ablative surgery, radiation therapy, or chemotherapeutic drugs with canalicular stenosis as a side effect.30–35 The most worrisome alternative diagnosis in patients previously treated for head and neck cancer is recurrent sinonasal cancer or a second primary tumor in the medial canthal region. However, the characteristic imaging appearance of dacryocystocele differs from that of a recurrent tumor, which should be associated with a solid enhancing mass. A careful search for a recurrent tumor along the course of the lacrimal duct, down to the inferior meatus in the nasal cavity, should be performed to exclude a tumor as a cause of the dacryocystocele. 9
Computed Tomography and Magnetic Resonance Imaging
Dacryocystocele presents on computed tomography (CT) and MR imaging as a fluid collection with thin rim enhancement along the course of the affected nasolacrimal duct, with no adjacent solid components. Meyer et al. 36 stated that the CT criteria for dacryocystocele in infants include the following triad: cystic medial canthal mass, dilation of the nasolacrimal sac, and a submucosal nasal cavity mass. Rand et al. 28 reported that the CT findings in four infants with congenital dacryocystoceles were cystic dilation of the lacrimal sac and a thin-walled cystic mass with slight rim enhancement.
The accuracy of prenatal MR imaging aids a definitive diagnosis by depicting the characteristic triad of dacryocystocele: paraocular cystic mass in the medial canthal region, nasolacrimal duct enlargement, and intranasal cyst. 29 Bianchini et al. 29 described the appearance of a prenatal dacryocystocele on MR imaging without contrast enhancement as a T2-weighted homogeneous, hyperintense cystic mass within the medial canthal region. Farrer et al. 37 reported that a congenital dacryocystocele in a three-year-old child appeared on MR imaging as a low signal intensity on T1-weighted images and T2-weighted signal hyperintensity. The differentiation between dacryocystocele and other less benign periorbital masses is often not possible only with sonography, especially when the lesion is unilateral. Prenatal MR imaging better defines the location of the various components of lacrimal system dilatation and their relation to the nasal cavity. This information may provide indications about the risk of postnatal respiratory distress. MR imaging can clarify the relation between the lesion and the upper airways to a greater extent, thus contributing to an adequate plan for management at birth. 29
Treatment and Prognosis
Treatment of congenital dacryocystocele is by light compressive massage, probing with a fine (#00-0000) Bowman probe to ensure prolonged permeability of the system, 38 or marsupialization of the nasal cyst (necessary for those with an intranasal component). 39 The resolution rate after a short course of antibiotics, warm compresses, and massage has been reported to be 76%.40,41 In some cases with intranasal extension of dacryocystocele, collaboration with an otolaryngologist may be necessary. 42 Moreover, in a retrospective study conducted by Wong and VanderVeen 10 on 46 infants with congenital dacryocystoceles presenting at a median age of 7 days of life, 65% presented with cellulitis or dacryocystitis and required systemic antibiotics. Four (9.5%) infants presented with respiratory compromise. Resolution occurred with conservative treatment for 10 eyes, but 36 (78%) required surgical intervention. If conservative treatment is not successful, a dacryocystorhinostomy may be performed. This procedure involves creating an iatrogenic bypass opening between the lacrimal sac and the middle meatus of the nasal cavity. Silicone tubes may be placed at the time of surgery to act as a stents to improve the likelihood of long-term success for this operation. 43 In the pediatric setting, although dacryocystocele is a benign condition, those with bilateral involvement and intranasal extension might cause respiratory distress syndrome requiring surgical intervention, as neonates are obligate nasal breathers.44–47
Conclusions
A number of clinical conclusions can be drawn from the cases presented and the related literature: (1) congenital dacryocystocele can be detected prenatally, usually in the third trimester of pregnancy, due to its embryologic basis; (2) although 2D sonographic diagnosis has been reported in the literature, only a few reports have documented the role of 3D sonography, Doppler, tomographic sonography imaging, and newer software algorithms in aiding and enhancing the antenatal sonographic diagnostic accuracy; (3) 3D sonography might potentially reduce the need for complementary diagnostic testing in the prenatal period; (4) although the lesion is benign in origin, the prenatal differential diagnosis is of critical importance in the prenatal counseling as dacryocystocele may be also a marker of syndromes and secondary to sinonasal tumors; (5) MR imaging may aid the antenatal definition of the diagnosis; and (6) MR imaging and CT scan are powerful diagnostic tools in the follow-up of patients after surgery for sinonasal cancer, avoiding misinterpreting dacryocystocele as a recurrent tumor.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.