
Abstract
Fetal urinary tract dilation (UTD), also known as fetal hydronephrosis, is one of the most common sonographically identified malformations in the prenatal period. The leading cause of UTD is a variety of obstructive uropathies. The literature on the management and classification systems for UTD is widespread and varied. Diagnosis by sonography benefits the outcome of the affected fetus because early recognition assists in determining further need for prenatal monitoring and postnatal care.
Urinary tract dilation (UTD) is identified sonographically in 1% to 2% of pregnancies. 1 The obstructive uropathies that commonly lead to UTD are uretero-pelvic junction (UPJ) and uretero-vesical junction (UVJ) obstructions. 2 In 50% to 70% of cases, the etiology of UTD detected by prenatal sonography is transient dilation, meaning it resolves on its own.1,3 The occurrence of fetal UTD is more prevalent in the male population, with a ratio of 2:1 compared with females. 2 Pyelectasis is another common renal anomaly that can lead to UTD, and the classification to differentiate between them involves the correct anteroposterior renal pelvis diameter (AP RPD) for determining severity. 2 The normal threshold for minimal risk of UTD and a diagnosis of mild pyelectasis is an AP RPD of 4 mm in the second trimester and 7 mm in the third trimester. The sensitivity rate is 100% using this threshold; however, a 21% false-positive rate was found for cases that led to persistent postnatal congenital UTD and associated morbidity. 2
The classification system for UTD varies widely in the literature for management, prognosis, and treatment. A multidisciplinary consensus resulted in an accurate system of classification. This combines sonographic features, such as parenchyma thickness, visualization of the normal bladder, visualization of the ureters, and amniotic fluid index, alongside the AP RPD measurements.1,2 Low-risk (UTD A1) and increased risk (UTD A2) urinary tract dilation are distinguished by gestational age and anteroposterior renal pelvis diameter, which provide an essential system to determine the need for continued management and postnatal care (Figure 1). 1
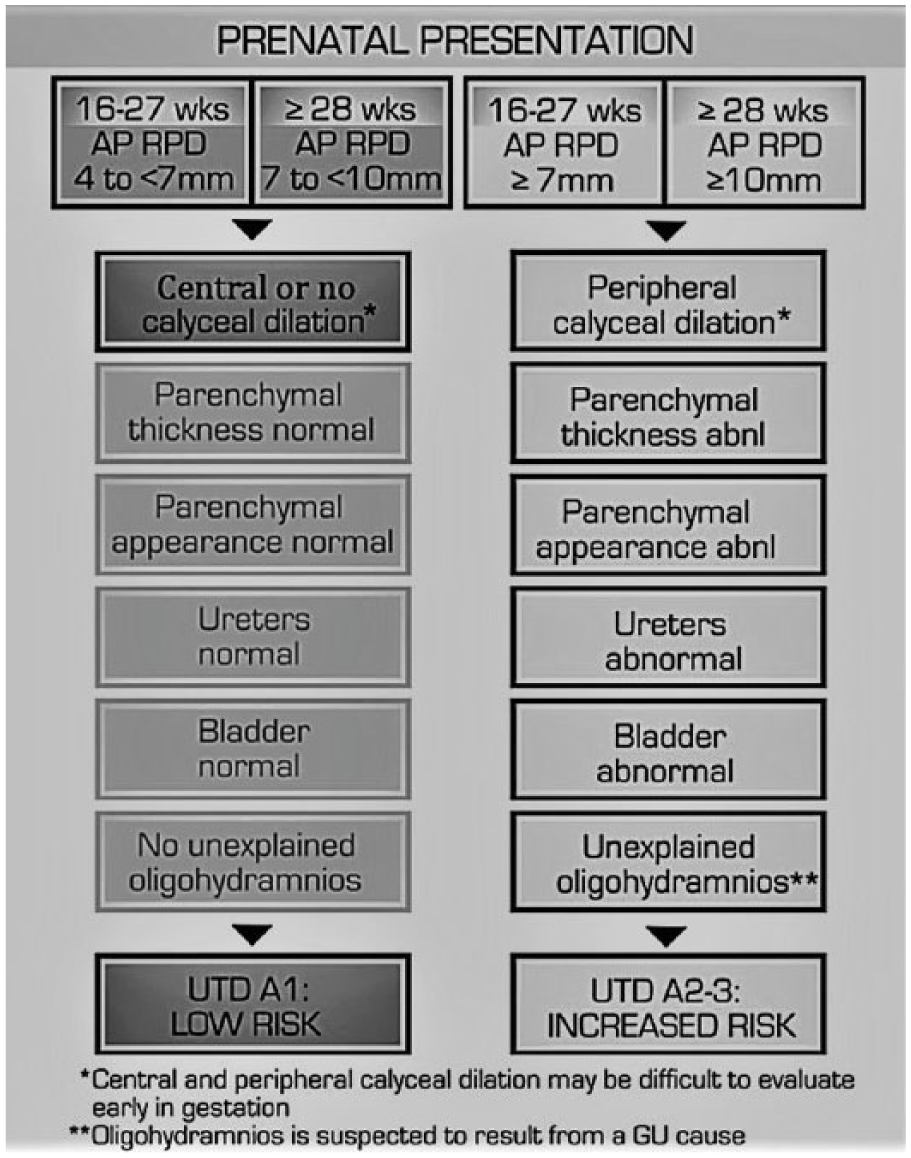
Urinary tract dilation (UTD) risk stratification: prenatal presentation for UTD A1 (low risk) and UTD A2-3 (increased risk).
A significant correlation is found between persistent UTD and timing for surgery. 4 The prenatal identification of renal anomalies results in options for prospective parents and allows the physician to determine management for improved prognosis. 5 The present case outlines a fetus with progressively worsening UTD throughout pregnancy, demonstrating the importance of obstetric sonography in patient diagnosis and treatment.
Case Report
A 35-year-old woman, G2P1000, was referred to the Maternal Fetal Medicine department due to advanced maternal age. The patient presented at 18 weeks 6 days of gestation for a detailed fetal anatomy examination. There was bilateral pyelectasis detected with the right renal pelvis AP RPD measuring 6.2 mm and the left measuring 7.2 mm. No other abnormalities were visualized during the examination. The classification of risk for UTD for the fetus was low (UTD A1) based on the minimal AP RPD and normal sonographic appearance of the urinary tract. 1 A follow-up sonogram was completed at 25 weeks, which demonstrated the right renal pelvis AP RPD dilated to 14.8 mm and the left dilated to 18.1 mm. At this appointment, the diagnosis was confirmed as UTD. The presumed cause was defined as bilateral ureteropelvic obstruction due to there being no visualization of the ureters and the normal bladder (Figure 2). At this time, the fetus was in the increased risk category, UTD A2-3, due to the AP RPD measurements and calyceal dilation. 1

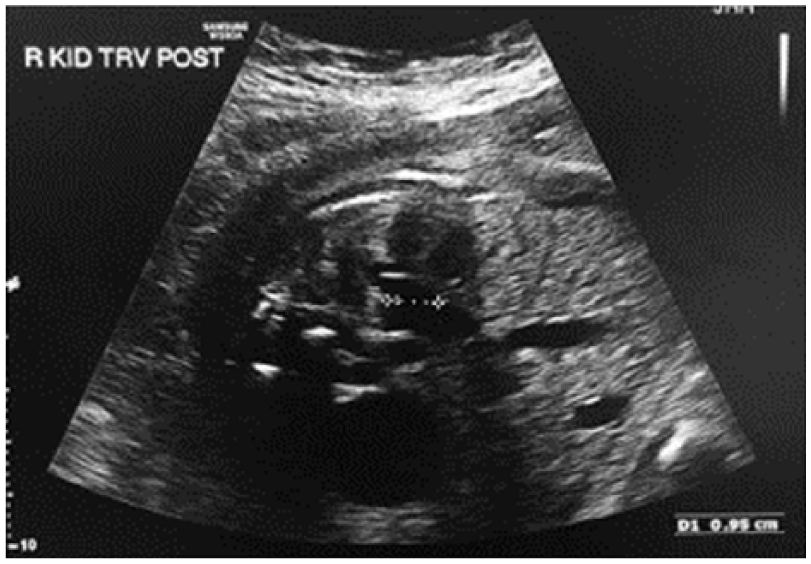
Transverse gray-scale image of the kidneys showing bilateral renal pelvis dilation.
Another sonogram was performed at 29 weeks’ gestational age that showed progression of bilateral UTD with the AP RPD up to 36 mm for the right and 22 mm for the left renal pelvis (Figure 3). There were spontaneous findings of anhydramnios, nonvisualization of the bladder (Figure 4), bilateral thinning of the parenchyma, and dilated calyces. These findings led to an even more severe risk category for UTD A2-3 as almost all the criteria were present, except for the normal ureters. The gender of the fetus was confirmed to be male on this sonogram, and no other abnormalities were seen aside from the UTD and subsequent diminished amniotic fluid. The physician recommended DNA testing and an amniocentesis be performed. Instead, the patient underwent cell-free fetal DNA screening, which revealed no risk for fetal chromosomal abnormalities. However, the mother was found to be a carrier for cystic fibrosis. The patient then came in for an amniocentesis for a more detailed chromosomal evaluation. Because of the presence of anhydramnios, fluid was instead removed from the fetal right renal pelvis because of its anterior location and accessibility. An amnio-infusion was also attempted at the time of the procedure to place fluid between the fetus and placenta to protect the umbilical cord. However, after attempts in two separate sites, the amnio-infusion was determined to be unfeasible. After the renal tap was performed, the right renal pelvis measured 9.5 mm and the calyces remained dilated (Figure 5). A follow-up sonogram at 29 weeks 5 days, only 2 days after the renal tap, showed fluid had reaccumulated in the right renal pelvis, which was dilated measuring 33 mm (Figure 6). The mother was induced, due to severe anhydramnios and UTD, thus delivering at 34 weeks 3 days. There was a need for immediate intubation of the neonate, and he was sent to a dedicated children’s hospital for treatment.

Gray-scale image of the right renal pelvis anteroposterior renal pelvis diameter (AP RPD) measuring 36 mm.
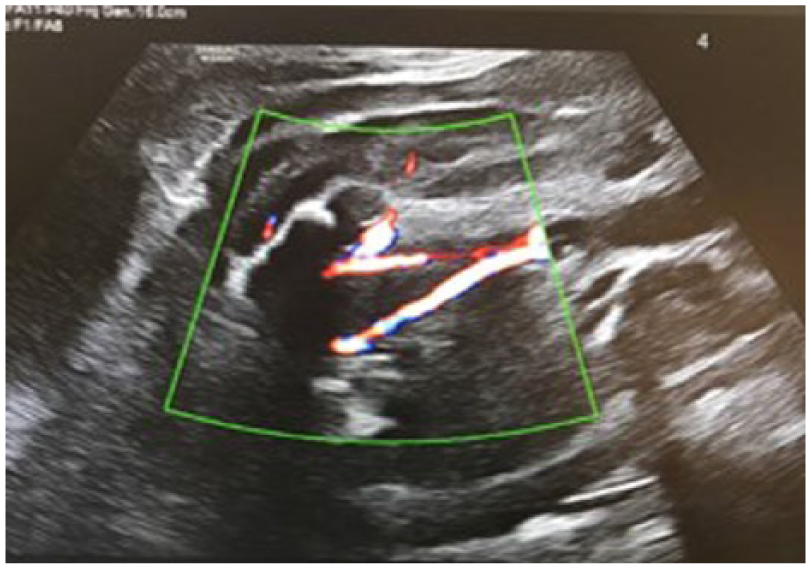
Color Doppler image showing the presence of a 3-vessel umbilical cord but no visualization of the bladder.
Gray-scale image showing the right renal pelvis anteroposterior renal pelvis diameter (AP RPD) after the renal tap measuring 9.5 mm.

Gray-scale image of the right kidney 2 days after the renal tap was performed. The right renal pelvis anteroposterior renal pelvis diameter (AP RPD) is shown measuring 33 mm.
Discussion
Fetal UTD is a common finding on prenatal sonography. The main concern arises from the differential diagnoses for the cause of UTD due to the diverse outcomes of the prognosis. Thus, it is imperative that accurate identification of the fetal kidneys is confirmed at the time of second trimester anatomic assessment. In the presence of suspected UTD, the AP RPD should be measured. Abnormalities of the renal parenchyma, bladder, ureters, and amniotic fluid level should be thoroughly assessed.
In this case study, the presumed diagnosis was UPJ obstruction, secondary to the findings of mildly dilated renal pelvices at the time of the second trimester detailed anatomy examination. However, the spontaneous nonvisualization of the bladder and anhydramnios are not common findings in upper urinary tract obstructions as the bladder is normally visible. The standard sonographic finding of proximal obstruction is a dilated renal pelvis. 1 Proximal urinary tract obstructions can be either unilateral or bilateral, with bilateral leading to a more severe prognosis and oligohydramnios. 5 The patient in this case presented with an even more severe form of obstruction resulting in the spontaneous findings of anhydramnios and nonvisualization of the bladder. This case demonstrates the importance of considering all plausible differential diagnoses.
Distal urinary tract obstructions have different sonographic signs that are used for determining the diagnosis. The presence of oligohydramnios, a dilated bladder, and dilated ureters are distinct findings of distal obstruction. 5 Distal urinary tract abnormalities include megacystitis, posterior urethral valves, and UVJ obstructions, which carry the worst prognosis rates as they can lead to pulmonary hypoplasia secondary to oligohydramnios. 5 However, these types of obstructions are not a possible diagnosis for the patient in this case because the bladder was not visualized.
Another differential diagnosis for UTD is multicystic dysplastic kidneys (MCDK). 5 The appearance of this pathology is enlarged, hyperechoic kidneys with large cystic spaces. 5 The condition can be bilateral and lead to pulmonary hypoplasia and a poor prognosis. 5 The appearance of MCDK and UTD are very similar; thus, the two are the most commonly confused anomalies. However, the differentiating factor is that in MCDK, the cysts do not communicate as they do with UTD. 5
Considering all the differential diagnoses, a proximal urinary tract obstruction was still suspected in the presented case. Based on the pattern of abnormal findings, it was presumed to be a severe prognosis. A crucial factor of this study was the close follow-up sonographic examinations that were performed. Because of routine second trimester sonographic screenings and follow-up examinations of the fetal kidneys, approximately 60% of children have surgery for renal or urinary tract problems in their first 5 years of life due to diagnosis from prenatal sonography. 2 This statistic shows the benefit of definitive prenatal diagnosis and the ability to manage treatment or request surgical intervention if necessary. 6 The classification system used in Figure 1 provides guidance for postnatal management planning. 1 If the risk for UTD is low (UTD A1), then two additional sonograms should be performed after birth, with the first one between 48 hours and the other no more than 6 months after birth. However, if there is an increased risk for UTD (UTD A2-3), follow-up should be prompt, with an ultrasound performed 48 hours after birth and an additional sonogram 1 month after birth. Furthermore, a urologist or nephrologist specialist consultation should be coordinated. 1 The use of antibiotics and surgical intervention with UTD A1 is at the discretion of the physician. However, with UTD A2-3, antibiotics are strongly recommended. 1
Notably, it has been found that one in three neonates with severe UTD persisting into the third trimester require postnatal surgery. 7 Also, infants with postnatal AP RPD of 10 mm or more have been found to have a significantly increased risk of infections when compared with infants with mild UTD. 7 These infants with UTD A2-3 have a substantial risk of developing a UTI and pyelonephritis. 7 In a meta-analysis by Sinha et al, 7 from a total of 3876 infants, it was found that neonates with high-grade UTD who were receiving antibiotic prophylaxis have a significantly lower rate of UTI compared with untreated neonates. Therefore, treatment by medication or surgical intervention is imperative for the optimal outcome of the patient postnatally.
This case provides an example on the importance of completing a full anatomic survey to verify any factors of anomalies or malformations. It is especially important in cases of urinary tract malformations since 25% of cases with obstruction are associated with other urologic abnormalities. 4 In addition, 12% of cases have other extrarenal abnormalities, such as anorectal anomalies, congenital heart disease, VATER syndrome, and esophageal atresia. 4
Conclusion
UTD is a common finding that generally resolves. This case provides a rare and severe exception. Obstetric sonography has high sensitivity for detection of urinary tract malformations and should be used consistently for evaluation. The classification system demonstrated in this study (Figure 1) is necessary to assess the need for follow-up and provide guidance for the best options for management and treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.