
Abstract
Objective:
This study aimed to compare the Society of Fetal Urology (SFU) guidelines, the anteroposterior pelvic diameter (APD), and the urinary tract dilation (UTD) classification criteria for predicting the prognosis of antenatal hydronephrosis (AH).
Materials and Methods:
This was a retrospective analysis of the relationship among the three classification criteria and their contribution to the diagnosis and prognosis of possible AH in a cohort of neonates.
Results:
This study was a retrospective review of 290 neonates. The mean age was 16.4 ± 9.0 days, and 33% of the study population comprised female babies. An image review demonstrated that 35% of the patients had severe vesicoureteral reflux (VUR), 22% exhibited severe obstruction, 40% had transient hydronephrosis, and 9% required surgery. The antenatal SFU grading criteria demonstrated a significant relationship with severe obstruction, and the postnatal SFU grading was related to the severity of VUR. The highest sensitivity for the presence of VUR for surgical intervention was obtained for prenatal SFU-1 (100%). The highest specificity was for prenatal SFU-4 (96%) for the presence of VUR, prenatal SFU-4 (99%), and postnatal SFU-4 (94%) for surgical intervention.
Conclusion:
No reliable sonographic findings were found to predict VUR or severe ureteropelvic junction obstruction. The SFU grading during the postnatal period may predict VUR with low sensitivity and specificity. However, all three classification criteria contributed to the evaluation of the need for treatment in this cohort.
Keywords
Antenatal hydronephrosis (AH) is a common and significant finding in prenatal sonography. Hydronephrosis is routinely detected in 0.5% to 2% of prenatal sonographic examinations.1,2 Transient hydronephrosis, ureteropelvic junction obstruction (UPJO), and vesicoureteral reflux (VUR) are the three most common causes that are assessed. 3 The findings of AH offer some opportunities for earlier diagnosis and treatment and can improve the prognosis of congenital anomalies of the kidney and urinary tract (CAKUT). Urinary tract infection (UTI) is one of the most common presentations of CAKUT. By diagnosing AH in the first weeks of life, patients may experience diminished infection and a lower risk of permanent kidney damage.
There are several classification criteria for the severity of AH. The Society of Fetal Urology (SFU) classifies hydronephrosis into four grades based on the level of dilatation and cortical thinning. 4 Measuring the anteroposterior pelvic diameter (APD) is another way of assessing severity (Table 1). 5 Recently, a more detailed grading system based on both APD and cortical, ureter, and bladder appearance was presented as a classification system for urinary tract dilation (UTD; Table 1).3,6
Comparison of the use of Urinary Tract Dilation and Anetroposterior Pelvic Diameter diagnostic criteria to detect antenatal hydronephrosis.
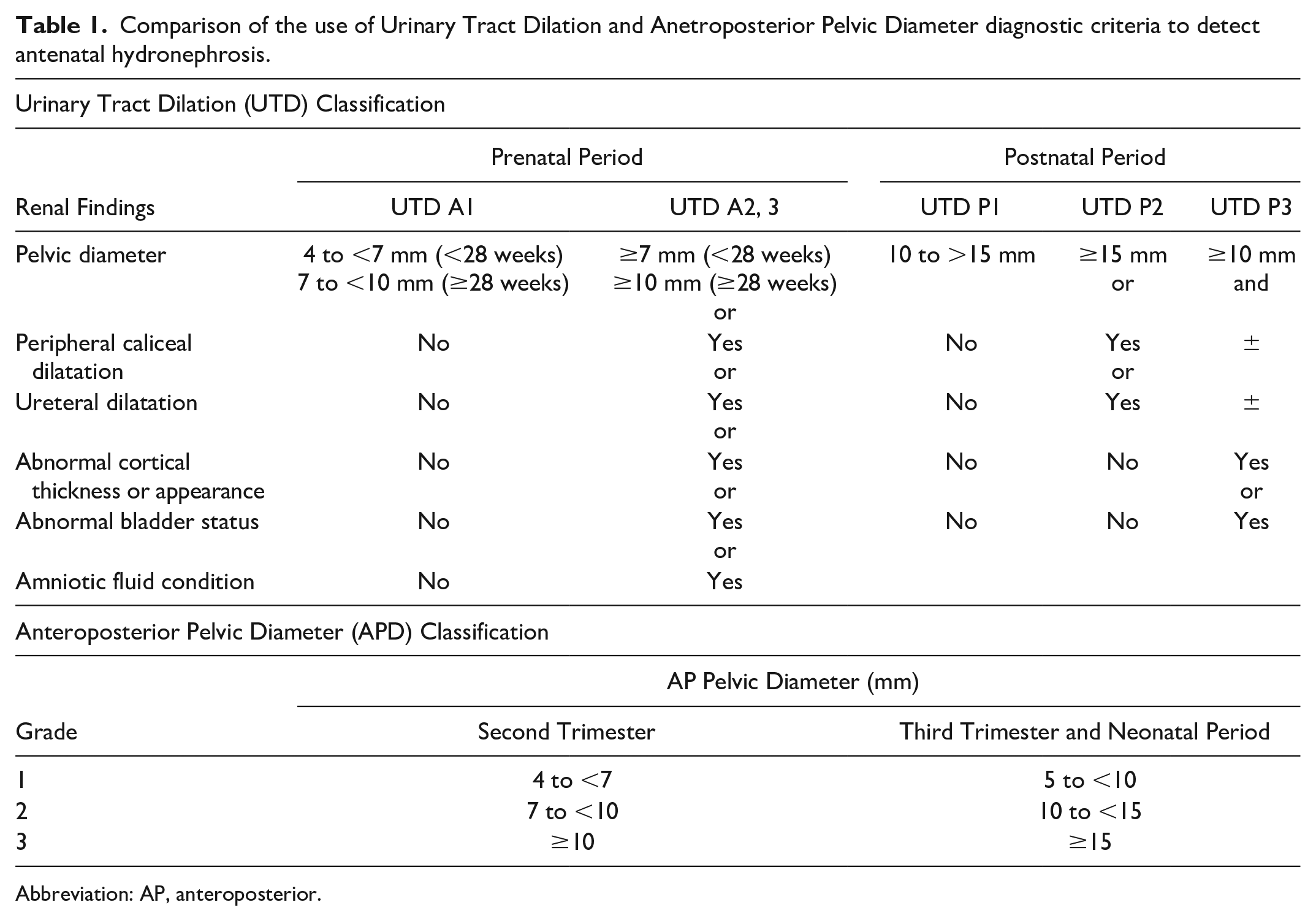
Abbreviation: AP, anteroposterior.
Important diagnostic questions to consider are the types of diagnostic imaging techniques that should be used when evaluating these patients. Many neonates with AH have a normal postnatal sonography examination; therefore, a repeat imaging study may be unnecessary. 7 Conversely, some critical entities, such as severe UPJO, VUR, and posterior urethral valve (PUV) require early diagnosis and treatment to prevent severe patient complications.8,9 It is yet to be established as to which of these classification systems (e.g., SFU, APD, or UTD) or a combination could provide improved pathologic detection. Hence, this study aimed to determine the value of the data generated using these criteria in detecting the cause and prognosis of AH and assess and compare the SFU guidelines, APD, and UTD classification criteria for predicting the long-term prognosis of AH.
Materials and Methods
This cohort study was designed as a retrospective study of patient data to detect AH. This study was reviewed and approved by the Mazandaran University of Medical Sciences (approval no./ID: IRMAZUMS.REC.1399.7912). Medical records of all neonates with a history of antenatal or neonatal hydronephrosis between March 2016 and March 2019 were reviewed. The operational definition of hydronephrosis was defined as dilatation of the pelvicalyceal tract, ureter, or bladder.
Hydronephrosis was classified based on SFU guidelines, APD, and UTD criteria. In the SFU grading system, hydronephrosis was classified as grade 0 (normal), grade 1 (slight separation of the renal sinus), grade 2 (increased separation of the central renal complex), grade 3 (dilation of the minor calyces), or grade 4 (severe dilatation and cortical thinning; Figure 1). According to the APD criteria, the severity of hydronephrosis was classified as mild (APD = 5–9 mm), moderate (APD = 10–14 mm), or severe (APD ≥15 mm; Table 1).
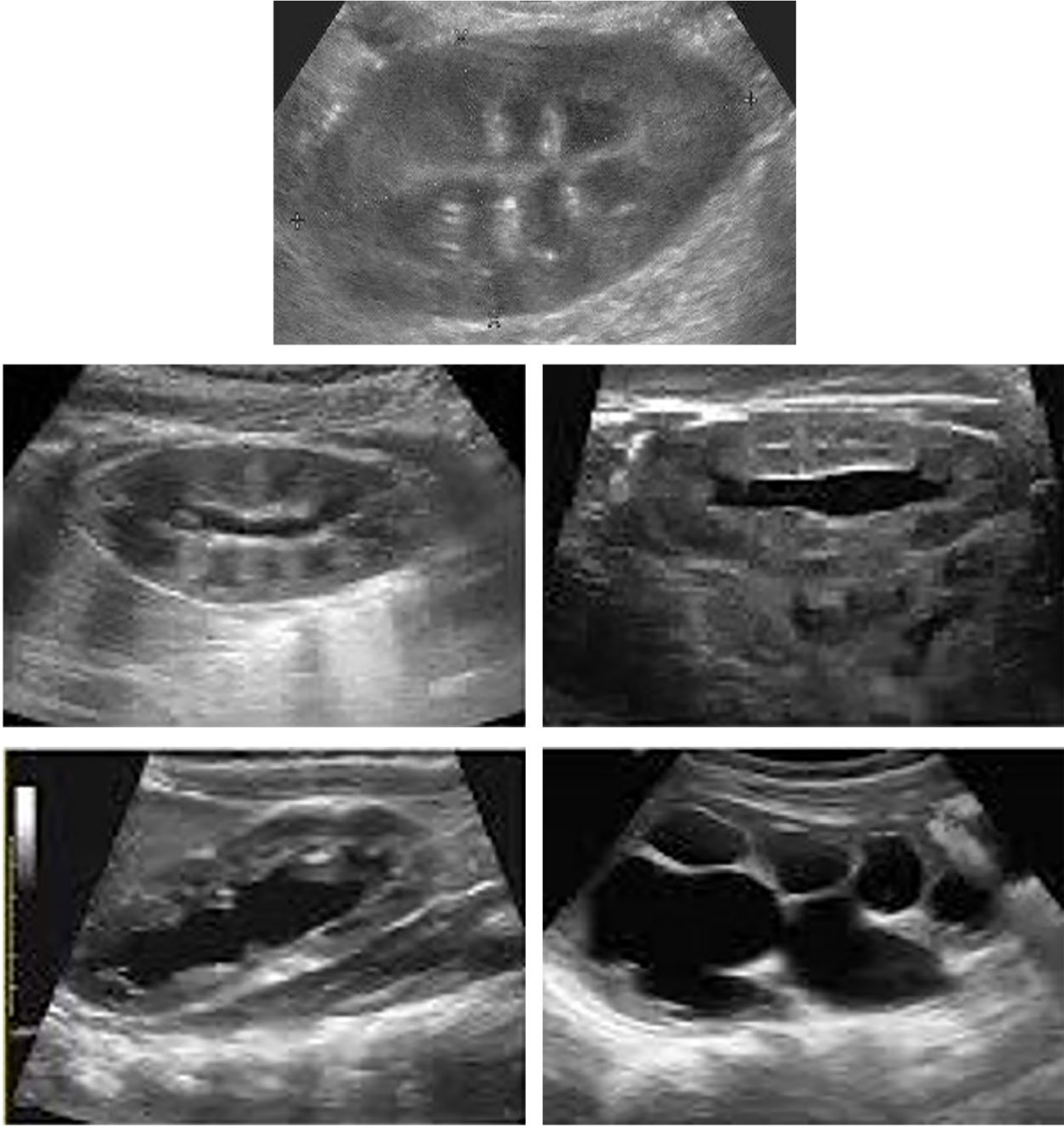
The Society of Fetal Urology (SFU) grading classification system for antenatal hydronephrosis and associated sonographic image examples. Grade 0 = normal sonographic appearance. Grade 1 = sonographic depiction of a slight splitting of the renal sinus. Grade 2 = sonographic depiction of the splitting of the central renal complex. Grade 3 = sonographic depiction of the dilatation of the minor renal calyces. Grade 4 = sonographic depiction of an enlarged renal collection system associated with renal cortical thinning.
Using the UTD criteria, the severity of the following items was assessed during the prenatal period: (1) pelvic diameter, (2) peripheral calyceal dilatation, (3) cortical thickness, (4) cortical appearance, (5) ureteral dilatation, (6) bladder status, and (7) amniotic fluid condition. All seven parameters, except the amniotic fluid condition, were also analyzed during the postnatal period. Overall, the findings were collected in two grades prenatally: milder cases (A1) and more severe cases (A2 and 3) prenatally and three grades in the postnatal period (P1, P2, and P3; Table 1).
In addition to reviewing the cohort’s medical records, all neonates with at least SFU grade 1, APD diameter >5 mm, or UTD A1 or P1 were checked for diagnostic follow-up. Based on the host facility’s protocol, sonography was ordered for all patients ages 3 to 30 days, except for neonates with moderate or severe bilateral hydronephrosis. Sonography and conventional voiding cystourethrography (VCUG) were performed during the first 48 hours of life in severe bilateral cases. Sonography was performed after the first 48 hours of life in neonates with unilateral or mild bilateral hydronephrosis.
Antibiotic prophylaxis and VCUG were ordered for patients with APD >10 mm, A2 and 3, P2, P3, and SFU grades 2 to 4. A dynamic nuclear medicine renal study using DTPA (TC99m–diethylenetriamine pentaacetic acid) or EC (TC99m–ethylenedicysteine) was performed in infants with grades 3 and 4 SFU, APD >15, and P3 UTD. The VCUG and nuclear medicine studies are usually completed after 2 months of age. The VUR was graded as mild (grades 1 and 2), moderate (grade 3), or severe (grades 4 and 5).
The cohort results were analyzed to determine whether there was a relationship between each of the three classification criteria based on the causative diagnosis and prognosis of AH. For the purpose of this study, prognosis was classified into four diagnostic grades. Grade 1 was defined as transient hydronephrosis and was operationally defined as complete resolution of hydronephrosis at 2 months of age without any treatment. Grade 2 was defined as mild kidney involvement, mild VUR, pelvic dilatation, or hydroureteronephrosis without kidney damage or the need for surgery. Grade 3 was defined as moderate kidney involvement, moderate VUR or hydronephrosis, or hydroureteronephrosis without any functional impairment or need for surgery. Finally, grade 4 was defined as severe kidney involvement, severe VUR, or severe obstruction with functional impairment or any need for surgery.
Statistical Analysis
The categorical and noncategorical variables were reported as percentages and means (±SD), respectively. Statistical analysis of the differences between groups was performed using the t test, Fisher exact test, and one-way analysis of variance (ANOVA). Moreover, the χ2 test was used for further data analysis and nonparametric tests, such as the Mann-Whitney and Kruskal-Wallis tests, were also used. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS software (IBM Corp., V 21).
Results
This cohort study was based on the review of 290 neonates, with a mean age of 16.4 ± 9.0 days, and 33% were female babies. The severity of AH in the prenatal and postnatal periods based on the three criteria is presented in Table 1. Most fetuses had mild hydronephrosis; 89% had grade 0 and 1 SFU classification, 67% had mild or no hydronephrosis based on APD, and 74% had A1 based on the normal UTD classification. The severity of AH increased during the first postnatal sonography based on the APD and SFU classifications. One third of infants had moderate/severe or grades 2 to 4 hydronephrosis, respectively. Based on the UTD, P2 and P3 levels were observed in 17% of the neonates. There was a significant relationship between prenatal and postnatal findings for each criterion.
In addition, 94 infants were found to have persistent moderate/severe hydronephrosis (SFU2–4, APD moderate or severe, and UTD P2 and P3) for VUR assessment. Thirty percent of patients had no evidence of VUR. However, nine (10%), 24 (26%), and 33 (35%) patients had mild, moderate, and severe VUR, respectively. Dynamic renal nuclear medicine examinations were performed on 72 infants with moderate and severe hydronephrosis. Approximately half of the patients showed no signs of dysfunction or obstruction. Thirteen (18%) patients had stasis, five (7%) had obstruction without hypofunction, and 19 (22%) had severe obstruction with hypofunction. The prognosis of this subset of patients with the four levels of AH is shown in Table 2.
Severity of Antenatal Hydronephrosis in Prenatal and First Postnatal Sonography, Based on Urinary Tract Dilation, Anteroposterior Pelvic Diameter, and the Society of Fetal Urology criteria.
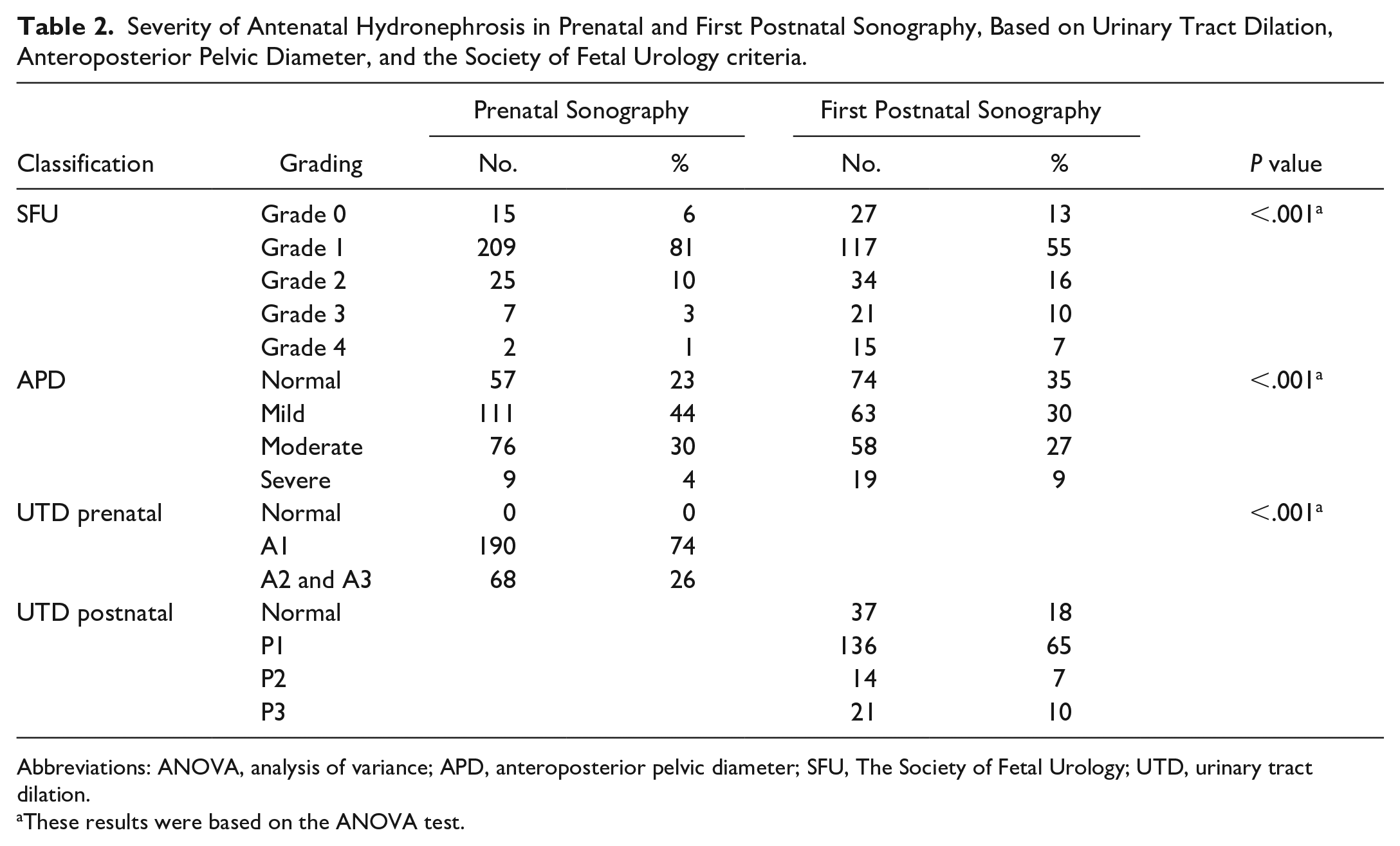
Abbreviations: ANOVA, analysis of variance; APD, anteroposterior pelvic diameter; SFU, The Society of Fetal Urology; UTD, urinary tract dilation.
These results were based on the ANOVA test.
Based on these criteria, it was possible to demonstrate the relationship between the severity of hydronephrosis and the level of renal involvement. There was no relationship between the severity of hydronephrosis and the severity of kidney involvement on prenatal or postnatal sonographic classification based on any criteria. Additional assessment was performed based on the relationship between nuclear medicine imaging and severe abnormalities. Only antenatal SFU grade showed a significant relationship with severe obstruction (P = .03). Postnatal SFU grade was the only sonographic parameter that showed a significant relationship with VUR severity.
The prognosis of the cohort based on the four aforementioned levels is shown in Table 2. In this study, no evidence of hydronephrosis was observed during the postnatal period. Evidence showed that 40% of the cohort had transient hydronephrosis, 94 (32%) had mild kidney involvement, 26 (9%) had moderate kidney involvement, 18% had severe kidney impairment, and 26 (9%) required surgery.
As previously mentioned, it is important to combine different prognostic determinants to form a pattern of the four diagnostic grades. The relationship between hydronephrosis severity and long-term prognosis is shown in Table 3. These results demonstrate that all three criteria have valuable prognostic adequacy in both prenatal and postnatal periods.
Severity of Vesicoureteral and Nuclear Medicine Imaging Impairments That Are Based on Prenatal and the First Postnatal Sonographic Findings.
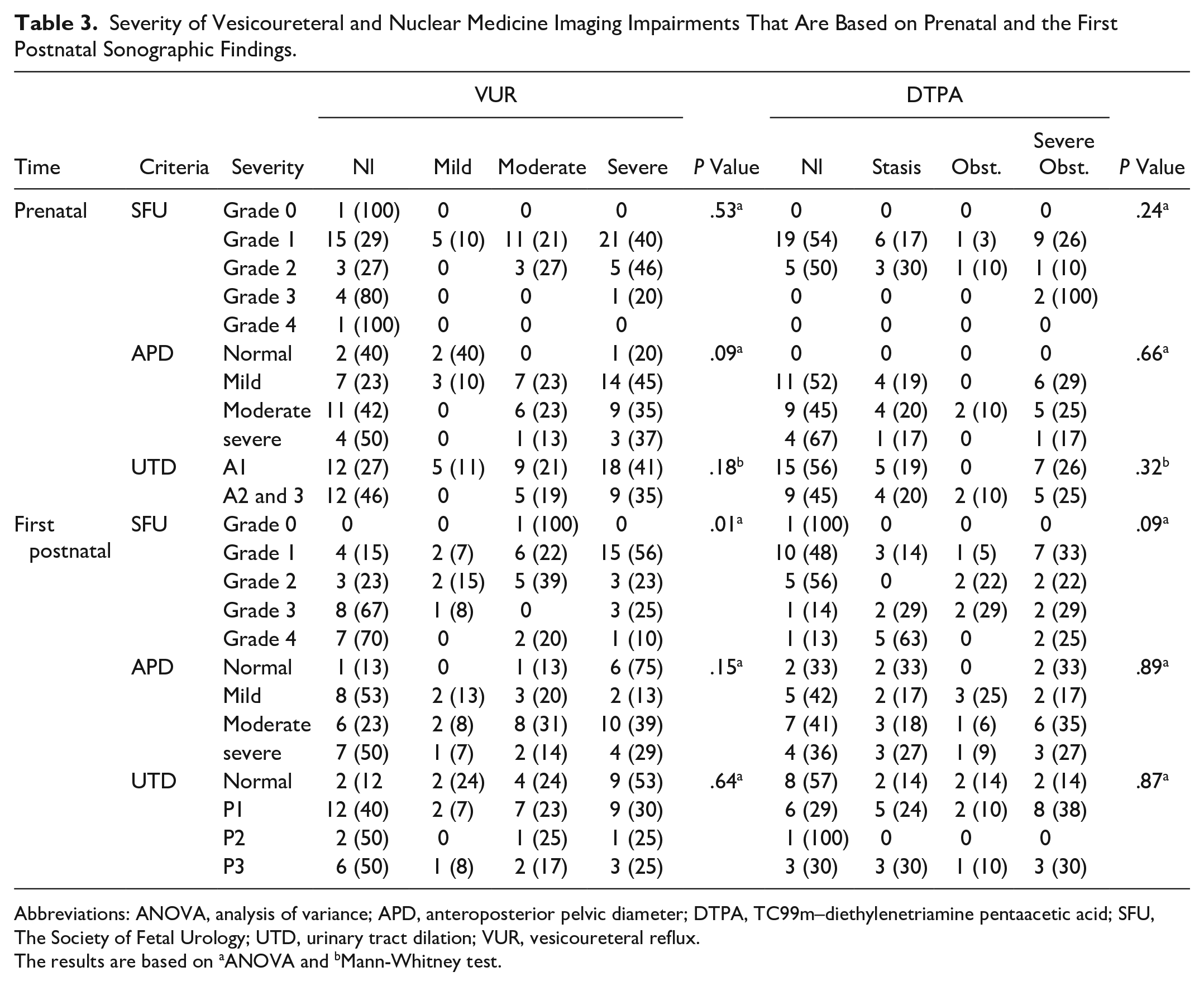
Abbreviations: ANOVA, analysis of variance; APD, anteroposterior pelvic diameter; DTPA, TC99m–diethylenetriamine pentaacetic acid; SFU, The Society of Fetal Urology; UTD, urinary tract dilation; VUR, vesicoureteral reflux.
The results are based on aANOVA and bMann-Whitney test.
In addition, further analysis was performed on the accuracy of all three criteria with different cutoff values for predicting significant morbidities: VUR, dilating VUR, significant functional impairment on DTPA, the need for surgical intervention, and severely unfavorable prognosis (Table 4). The cutoffs for SFU were grades 1, 2, 3, and 4 in the prenatal and postnatal periods, respectively. The cutoff values for APD were pelvic diameters ≥10 mm and ≥15 mm in the prenatal and postnatal periods, respectively. The diagnostic cutoff for UTD was UTD-A2 and 3 at prenatal and UTD-P1, UTD-P2, and UTD-P3 during the postnatal period.
Long-term Prognosis of Neonates With Antenatal Hydronephrosis, Based on Prenatal and the First Postnatal Sonographic Findings.
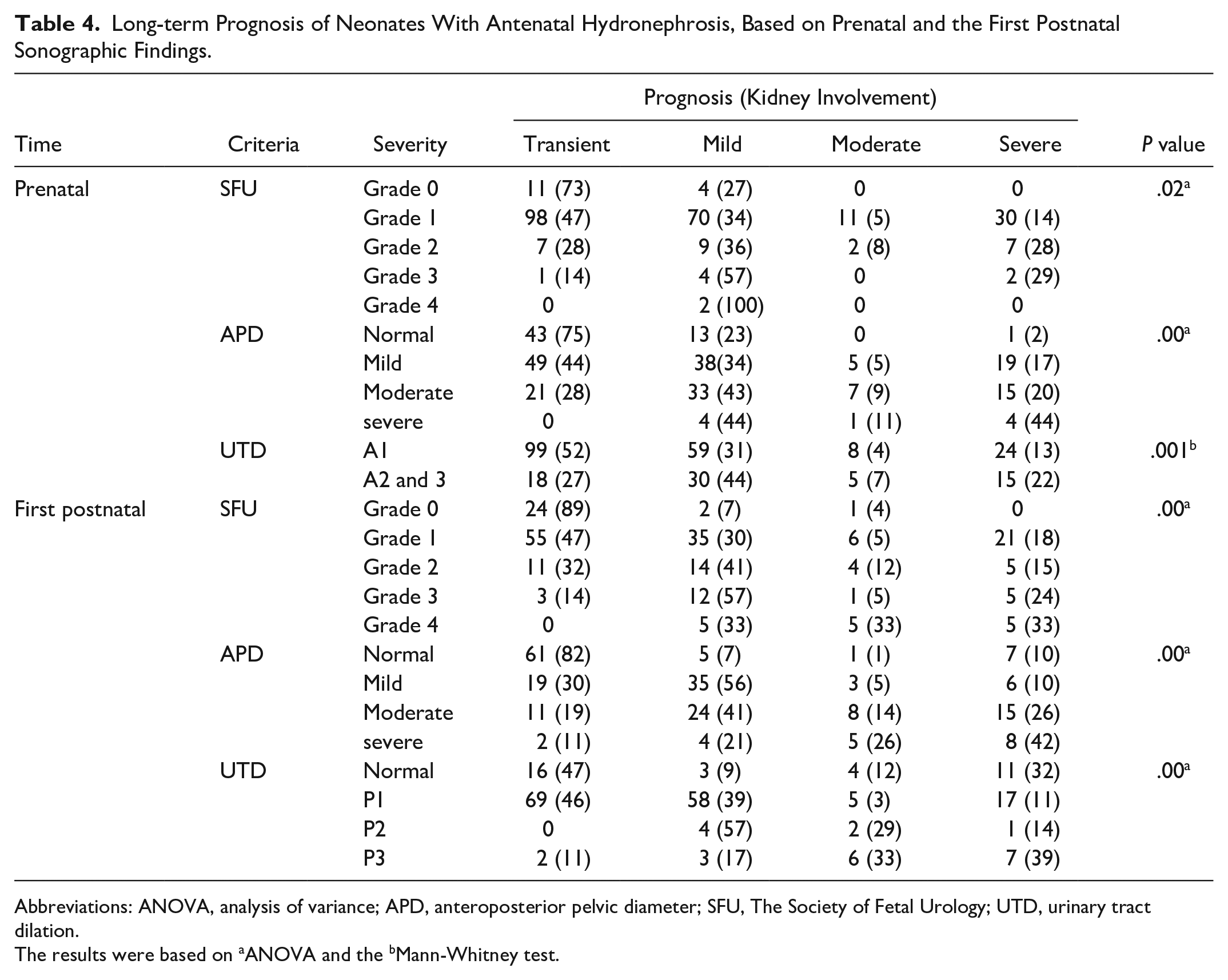
Abbreviations: ANOVA, analysis of variance; APD, anteroposterior pelvic diameter; SFU, The Society of Fetal Urology; UTD, urinary tract dilation.
The results were based on aANOVA and the bMann-Whitney test.
A summary of this cohort’s findings demonstrated the following:
On prenatal sonography, SFU-3 showed a significant relationship with the presence of VUR, SFU-2, and APD with severe unfavorable prognosis, and UTD with surgery.
On postnatal sonography, SFU-3 showed a significant relationship with all but functional impairment; UTD with VUR presence, severely unfavorable prognosis, and surgery; and APD with severely unfavorable prognosis and surgery.
No prenatal or postnatal sonographic indices could predict kidney functional impairment.
The highest sensitivity of each morbidity item was prenatal SFU-1 (100%) and postnatal SFU-1 (98%) for VUR presence, prenatal SFU-1 (100%) and postnatal SFU-1 (97%) for dilating VUR, prenatal and postnatal SFU-1 (100%) for surgery, and a severely unfavorable prognosis (table 5).
The highest specificity of each morbidity item was prenatal SFU-4 (96%) and postnatal UTD-P3 (73%) for the presence of VUR, prenatal SFU-4 (97%) and postnatal SFU-4 (74%) for dilating VUR, prenatal SFU-4 (99%) and postnatal SFU-4 (94%) for surgery, and prenatal SFU-4 (99%) and postnatal SFU-4 (94%) for severe unfavorable prognosis (table 5).
Sensitivity and Specificity of the Three Criteria (Urinary Tract Dilation, and Anteroposterior Pelvic Diameter, and The Society of Fetal Urology) With Different Diagnostic Cutoff Points for the Prenatal and Postnatal Period for Suggesting the Prognosis of Hydronephrosis.
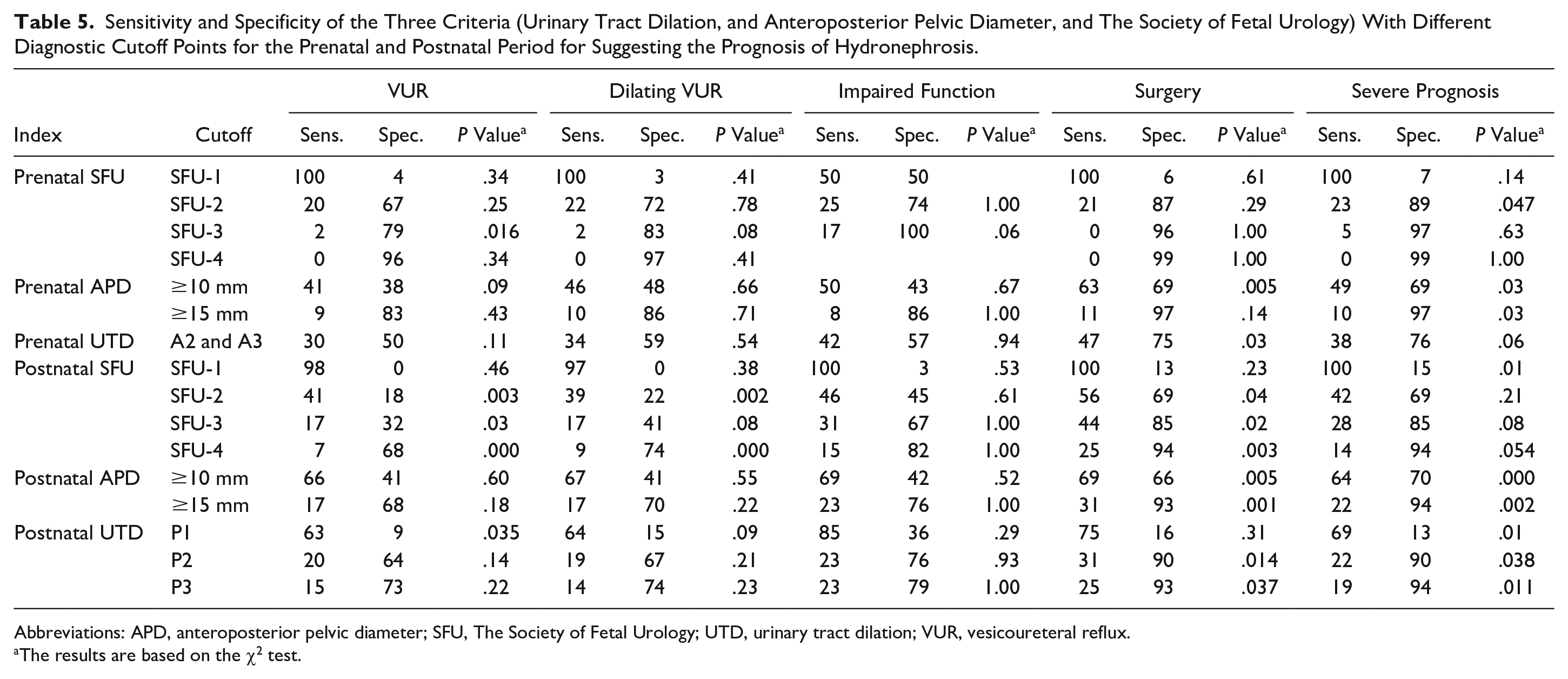
Abbreviations: APD, anteroposterior pelvic diameter; SFU, The Society of Fetal Urology; UTD, urinary tract dilation; VUR, vesicoureteral reflux.
The results are based on the χ2 test.
Discussion
Fetal hydronephrosis is a prenatal concern in 0.5% to 2% of pregnant women. As part of the antenatal assessment of this uncommon fetal pathology, determining the most sensitive imaging techniques for diagnosis and follow-up is still warranted. Renal and urinary tract sonography is considered the most widely available imaging method for screening this type of fetal compromise. 10 In this study, it was important to compare the sensitivity of three specific AH criteria (SFU, APD, and UTD) to determine the proper cause and prognosis of infants at risk. This study underscores the fact that prenatal and initial postnatal sonographic findings are significantly associated with the presence or severity of VUR. This study also found that all three criteria had high sensitivity and specificity for predicting the long-term prognosis. To put these findings into context, a literature review was conducted to better understand this set of cohort results.
Zhang et al completed a sonographic screening of a cohort of pregnant women and found 34 cases of AH, of which 62% were men, 71% with UTD-A1, and 29% (n = 10) with A2 and 3 severity. 11 In those patients, VUR was the most common cause, and two patients (6%) needed surgery. 11 A compatible study by Nelson et al reviewed the radiologic records of 494 infants (75% male infants), who were selected due to a history of AH. 12 In that cohort, the patients had a median age of 28 days and a median diagnostic follow-up of 19.8 months. 12 Higher than grade 2 VUR was observed in 12.1% and UPJO in 6.3% of that cohort of patients. 12 There was a significant difference between the grades of UTD in anticipating dilating VUR and UPJO (both P < .001). 12 Green et al studied the persistence of AH detected in the second trimester to the third or postnatal trimester. They followed 347 fetuses with second-trimester hydronephrosis. Hydronephrosis persisted in 150 (43%) patients in the last trimester and in 49 (17%) infants postnatally. The persistence rate was significantly higher in UTD-A2 and 3 than in UTD-A1. 13
In this study, the male-to-female ratio was 2:1, and most patients indicated a mild degree based on all three criteria. In the prenatal group, 81% of the sonography reports were SFU grade 1, 44% were mild APD, and 74% were UTD-A1. In the postnatal period, 55% of the sonography reports were SFU grade 1, 35% were normal APD, and 65% were UTD-P1. Only 4% of the patient cases had prenatal SFU ≥3 or APD ≥15 mm. These values were 17% for SFU ≥3, 9% for APD ≥15 mm, and 10% for UTD-P3. These results are similar to those reported previously. This may indicate that most cases of AH are due to mild and insignificant anomalies of the kidneys and urinary tract. Sonographic findings for AH are impactful as they may aid in detecting mild cases, which may require no further diagnostic or therapeutic interventions.
Prenatal and postnatal sonographic findings may also be helpful in cases with the potential for more significant pathologies, moderate/severe VUR, or significant obstructive processes. In this cohort, prenatal sonographic findings indicated an inability to diagnose VUR or severe obstructive UPJO. Postnatal APD was not significantly associated with the diagnosis of VUR or UPJO. The SFU can predict VUR with a sensitivity of 41% and a specificity of 68%. The values for UTD-P1 are 63% and 9%, respectively. Therefore, sonographic indices have limited ability to predict VUR or UPJO, except for SFU, which has low sensitivity and specificity. This body of evidence suggests that sonography may not be reliable for postnatal assessment of AH.
In a retrospective study by Serhan et al, out of 44 infants, 54% had grade 3 AH, and 46% had grade 4 AH, based on the SFU criteria. In their cohort, 10 patients (23%) patients required surgery. 14 In a similar study by Rickard et al, data from 193 infants with grades 3 and 4 SFU hydronephrosis without VUR were analyzed. Their study assessed the renal parenchyma area (RPA), hydronephrosis area (HA), parenchymal-to-hydronephrosis area (PHAR), APD, and SFU grade. In that study, 58 (30%) infants underwent surgery and the SFU, APD, UTD, HA, and PHAR scores were significantly higher in the surgery group (all P < .001) but RPA (P = 0.5). 15 Kiener followed 179 neonates with a history of AH. The UPJO was the cause in 26 (15%) infants, and VUR was the cause in 10 (6%). Surgery was performed for 32 patients. The APD with a cutoff of 11.7 mm had a sensitivity of 79% and specificity of 66% for predicting significant nephropathy requiring surgery. The SFU grades 3 and 4 showed a sensitivity of 59% and a specificity of 86% for detecting a surgical outcome. 16 Kwiatkowski assessed the predictive value of measured medullary pyramid thickness (PT) in 91 infants with grades 3 and 4 SFU hydronephrosis. Overall, a smaller PT was associated with an increased risk of surgery, but PT measured in the first 3 days of life did not have much predictive value. A PT of <3 mm after the third day of life showed higher relation with pyeloplasty. 17 In a retrospective study, Hwang assessed the relation between sonographic findings and the need for surgery in 504 sonographic records from 336 neonates with a history of AH. Fifty-eight sonographic records led to surgical intervention. Sonographic findings based on UTD showed significant differences between the two groups of surgical or conservative therapy (P < .001). The presence of APD ≥15 mm, peripheral calyceal dilation, ureteral dilation, parenchymal thickness abnormality, and bladder abnormality was significantly associated with the surgical approach to therapy. 18 Melo, in a study spanning 30 years, followed up 447 infants with isolated AH for a mean of 9 years. The mean APD was 10 mm, and the frequencies of cases based on SFU grades were 41%, 16%, 12%, and 31% for grades 1, 2, 3, and 4, respectively. The UTD grading was 57% UTD-P1, 21% UTD-P2, and 22% UTD-P3. A total of 131 (29%) infants underwent surgery. All three classifications provided excellent information for predicting surgery. The sensitivities and specificities for APD, SFU, and UTD were 99%, 82%, and 100%, and 81%, 100%, and 81%, respectively. 19
In this study, surgical intervention was indicated in 26 infants (9%). These differences were likely due to the neonates involved in this review. In this cohort, all infants with AH were included, except those with significant pathology. This study reported on all neonates with AH; therefore, the surgery rate was lower than that in studies with selected patients with severe hydronephrosis. Furthermore, APD ≥10 mm and UTD-A2, 3 were significant prenatal predictors of the need for surgery. The APD had a sensitivity and specificity of 63% and 69%, respectively. The sensitivity and specificity of UTD for predicting the need for surgery were 47% and 75%, respectively. The sensitivity and specificity were similar to those of other studies, which may be a reasonable but not confirmatory finding. In the postnatal period, SFU grade 2, APD ≥10 mm, and UTD-P2 significantly predicted the need for surgery. The SFU grade 2 had a sensitivity of 56% and specificity of 69%; however, when other grades of SFU were reviewed, it reached a sensitivity of 100% for SFU grade 1 and a specificity of 94% for grade 4. An APD ≥10 mm had a sensitivity of 66% and a specificity of 69%, while the specificity for an APD ≥15 mm was 93%. The UTD-P2 offered a sensitivity of 31% and a specificity of 90%, with a sensitivity of 75% for UTD-P1. Therefore, based on this study, all three criteria had reasonable but not excellent sensitivity and specificity in predicting the need for surgery in the postnatal period. In addition, the SFU classification may not be a reliable index for the prenatal period.
Singh et al retrospectively assessed prenatal and postnatal sonographic data of 70 infants with AH. In their work, they defined severe renal impairment as perinatal morbidity and mortality, duration of neonatal intensive care unit (NICU) stay, and the need for neurosurgical intervention in neonates. The most common cause was UTD of transient hydronephrosis in 39 patients (55.7%), followed by UPJO in 13 patients (18.5%), and VUR in only five patients (7.1%). None of the fetuses with normal or A1 prenatal sonograms showed any significant postnatal UTD abnormalities. In contrast, 70% of neonates with a history of prenatal UTD A2 and 3 risk in a previous prenatal scan had persistent postnatal UTD pathology. Indeed, all infants with abnormal postnatal UTD underwent prenatal UTD A2 and 3 scans (increased risk). Surgery was performed in nine infants (12.8%), with all patients categorized as having UTD A2 and 3 prenatally and P3 postnatally. 20
Kaspar et al reviewed the sonographic data of 203 neonates with AH. Urinary tract abnormalities were observed in all 36 infants. Thirty patients had available prenatal data and 27 (90%) had abnormal prenatal sonography findings. The UTD-A (with a cutoff of A1) had a sensitivity of 77% and a specificity of 84% for detecting an abnormal urinary tract. 21
Previous studies have not yet reported on the prediction of impaired renal function using nuclear medicine renal examination. Hence, this study proposes a prognostic scale by combining items such as the severity of VUR or obstruction and the need for surgery. All indices significantly predicted severe unfavorable prognoses during both prenatal and postnatal periods. The sensitivities of prenatal SFU, APD, and UTD were 100%, 49%, and 38%, and their specificities were 89%, 97%, and 76%, respectively. The sensitivities of postnatal SFU, APD, and UTD were 100%, 64%, and 69%, respectively, and their specificities were 15%, 94%, and 94%, respectively. Therefore, all three classifications had reasonable sensitivity and specificity for the prognostic assessment of AH.
Limitations
This study has a major limitation owing to its retrospective design and threats to internal and external validity. In addition, the participants were convenience samples who attended a single health center, which included only a limited number of neonates and focused primarily on the clinical aspects of AH. Other diagnostic aspects, such as the technical and visual qualities of the sonograms, were not considered. The results of this cohort study were specific to this group of patients.
Conclusion
This cohort study, which was designed to assess AH, demonstrated that there were no reliable prenatal sonographic findings that predicted VUR or severe UPJO. This study found that SFU grading during the postnatal period predicted VUR with low sensitivity and specificity. All three criteria for grading AH provided prognostic referrals, such as the need for surgery. The only exception was prenatal SFU classification, which predicted the need for surgery. This study provides limited evidence that sonography can provide prognostic information about AH, but not causative information. Sonologists and sonographers should review this set of diagnostic criteria for AH and determine how they can be applied in the patient population. Therefore, it may be wise not to rely solely on sonographic information for the diagnostic workup of AH. Further studies and additional evidence are required to guide clinicians and patients with suspected AH.
Footnotes
Ethics Approval
This study was reviewed and approved by the Mazandaran University of Medical Sciences (approval no./ID: IRMAZUMS.REC.1399.7912).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not Applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.