
Abstract
Ergonomic training is necessary to help reduce work-related upper limb disorders (WRULD) in sonographers. This study provided an ergonomic training session for sonographers, to determine whether a teaching intervention changed the grip force used to hold a transducer. Thirteen practitioners participated and were placed into two groups (intervention group n = 7). Participants were asked to scan the same simulated transabdominal early pregnancy case. An ergometer was used, which enabled all participants to hear the effect of holding the transducer tightly. Their matched grip force was measured before and after the intervention using a dynamometer. The intervention group reviewed videos and photographs taken during the scan to see if this affected the matched grip force further. Study findings showed that the short ergonomic training session with the use of an ergometer significantly reduced the matched grip force applied to a transducer (P < .05) for all participants. The video/photo review did not result in any further significant changes.
Keywords
Introduction
Work-related musculoskeletal disorders (WRMSD) have been reported in sonographers, with figures of up to 90.5% quoted for sonographers scanning in pain. 1 Transducer grip and grip pressure/force have been reported as contributory factors in the development of WRMSD. 2 Baker and Coffin 3 identified poor posture as an additional factor impacting on the increased incidence of WRMSD, along with other factors such as the workforce age, increased patient throughput, and increased reporting due to improved awareness of WRMSD. Using a pinch grip to hold the transducer increases the strain on muscles when compared with a power grip, with a pinch grip involving five times the applied force of a power grip. 4 Some sonographers working in specialized areas of practice, such as vascular or cardiac, are more likely to have wrist pain,5,6 which has been attributed to using a high grip force. Although not found to be causal, 6 smaller transducers are used in both vascular and cardiac scanning, which may prevent the sonographer using a power grip to hold the probe; this was supported by one participant’s statement in the research by Evans et al. 5
There has been an increase in both the demand for sonography and the number of obese patients,7,8 which can have an impact on grip pressure and potentially WRMSD.2,3 This was reflected in the work by Monnington et al., 9 who reported that sonographers use increased transducer force when scanning obese patients. Gemark Simonsen and Gard 10 reported that cardiac sonographers’ extended examination times and increased transducer pressure when scanning obese patients contributed to increased transducer grip force. The authors of the study 10 found that inexperienced sonographers who take longer to scan also suffer due to increased force applied to the transducer. This was supported by Evans et al., 5 who concurrently reported that pushing when scanning can lead to increased transducer grip and associated injury.
Ergonomic training has been recommended to improve awareness of ways to reduce the risk of injury among sonographers.9,11,12 Hoe et al.’s 13 systematic review suggested no difference in outcome pre- and posttraining for computer workers, although they did find self-reported compliance to be increased after training to use ergonomic equipment in one study. However, their review was challenged by the quality and variance between studies and outcome measures. 13 Fisher 14 used video presentations to determine the effect of training on the working practices of sonographers. In their small study of 16 participants, they found that 62% self-reported to have changed their working practice after reviewing the video. Martimo et al. 15 found a significant difference in self-reported productivity loss in a group of workers who had received conventional health care, compared to those who had additional occupational physiotherapy support but no difference in pain scores. The improved productivity was thought to be due to the changes implemented following advice from the therapist. Despite the limited evidence to support training, the National Institute for Occupational Safety and Health 16 has recommended regular training, to include optimization of posture and use of supportive equipment.
Grip strength has been associated with muscle mass and function, with reduced grip strength affecting injury risk and disability. 17 When assessing the hold of an object, to overcome confounding factors such as age and height, matched grip force can be used.18,19 This involves participants holding an object, in this case a transducer, then matching the grip by holding a dynamometer (a device for measuring grip force) with the same force as they held the transducer.
In 2006, Murphey and Milowski 20 used an ergometer to highlight the reduction in muscle tension when optimizing the scanning position. An ergometer that emits a sound when muscles are stimulated, increasing in intensity when muscles are under strain, was used in this study to assist in the training to help improve the sonographers’ awareness of grip force and reduce their transducer grip. 9 This current study builds on previous work,21,22 which evaluated ergonomic training of student sonographers in an attempt to reduce transducer grip force. The aim was to ascertain if a short intervention training session using an ergometer could reduce the transducer matched grip force among sonographers. This current study also evaluated whether reviewing videos and photos of the hand/wrist, taken while scanning, had an impact on transducer matched grip force. It was hypothesized that a short teaching session might reduce the matched grip force applied to an ultrasound transducer. In addition, utilizing visual feedback in the form of videos or images of the participant scanning could lead to further reductions in matched grip force.
Method
The study was conducted in the ultrasound skills suite at City, University of London, following ethics approval from the School of Health Sciences research ethics committee (ref. Staff/13-14/04). The number of sonographers working in the UK is unknown, so a sample size calculation was not completed. Convenience sampling was used for the study. Volunteers were recruited from sonography clinical supervisors’ training days at City, University of London in 2013 and 2014; participants of a study looking at factors affecting grip strength at the British Medical Ultrasound Society (BMUS) conference in Gateshead 22 ; and advertisements in Ultrapost, the BMUS online newsletter. Inclusion criteria were open to participants having any level of sonography scanning experience. Despite the research being well advertised, the uptake was low; low numbers of volunteers for experimental studies have been found to be common.14,20,23
The technique used was adapted from a study looking at matched grip force among sonography students. 21 Participants were randomized into two groups, a control and intervention group, using a simple randomization method using cards with C or I on them, to provide a similar number of participants in each group. Participants in both groups had their maximum grip strength measured initially using a Jamar dynamometer (Figure 1A), with the highest of three measurements recorded for their scanning arm using the same standardized technique as Roberts et al 17 and Wood et al. 22 Participants were then invited to scan a case on the UltraSim ultrasound simulator, during which time photos and/or videos were taken of their hand, wrist, and arm, with no intervention from the researcher. Immediately following the scan, participants were then asked to grip the dynamometer with the same amount of grip force as they used during the scan; this matched grip force was recorded, following the procedure used by Bao and Silverstein 18 and Bastian et al. 19 Scans were performed using the UltraSim to try to ensure consistency of the scanning environment. The same transabdominal early pregnancy case was used for each participant. The room was equipped with a Bambach saddle chair and a moveable examination couch.
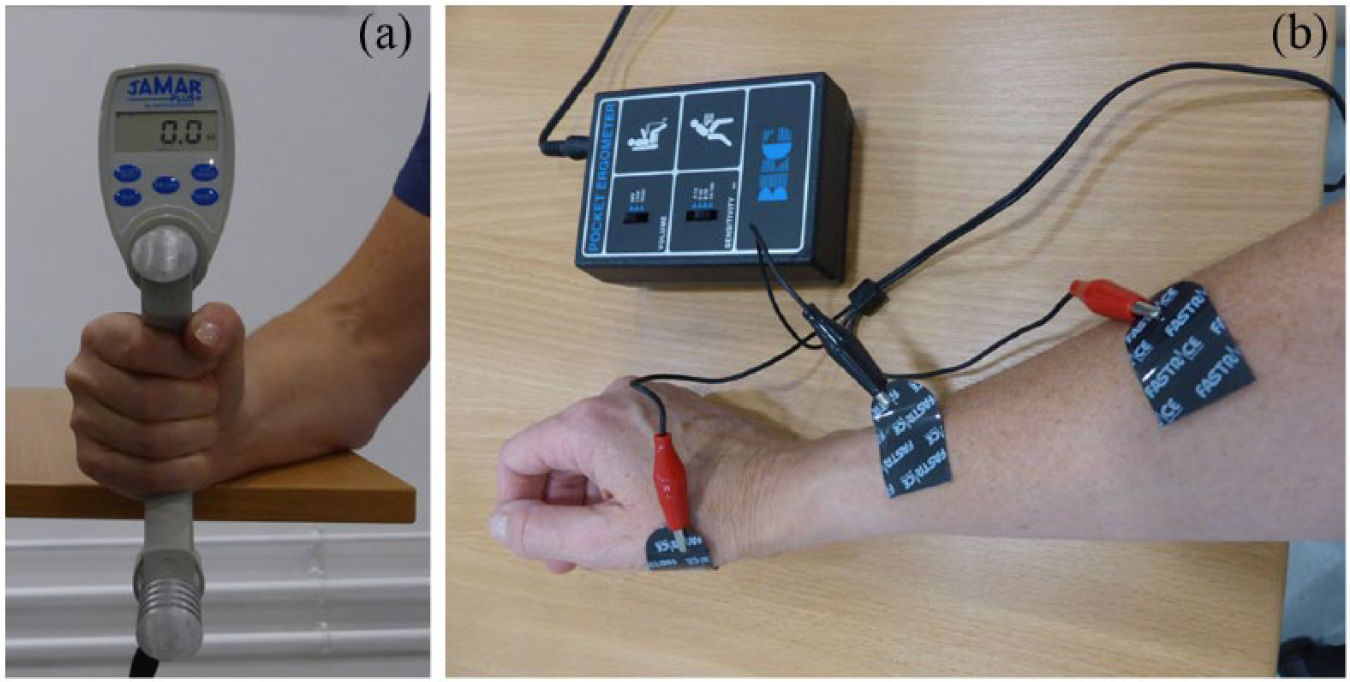
(A) The dynamometer used to measure maximum grip strength and matched grip force. (B) The ergometer attached to the scanning arm to measure muscle activity.
Participants then had the ergometer attached to their forearm, using the same technique as Harris 21 (Figure 1B) to assist in the short teaching session. This allowed participants to hear when the muscles were under strain due to their scanning technique, posture, and grip force, while experienced facilitators worked with the sonographer to improve the ergonomics during the scan. At the end of the short teaching session, participant’s matched grip force was again measured and recorded. The intervention group was shown videos and/or photographs of their hand and wrist taken during the scan to look for “white knuckles” (a sign of a tight grip) and hand/wrist positions while holding the transducer, then asked to scan again before measuring the matched grip force for a third time. The control group were was asked to scan again and the matched grip force measured and recorded (Figure 2).
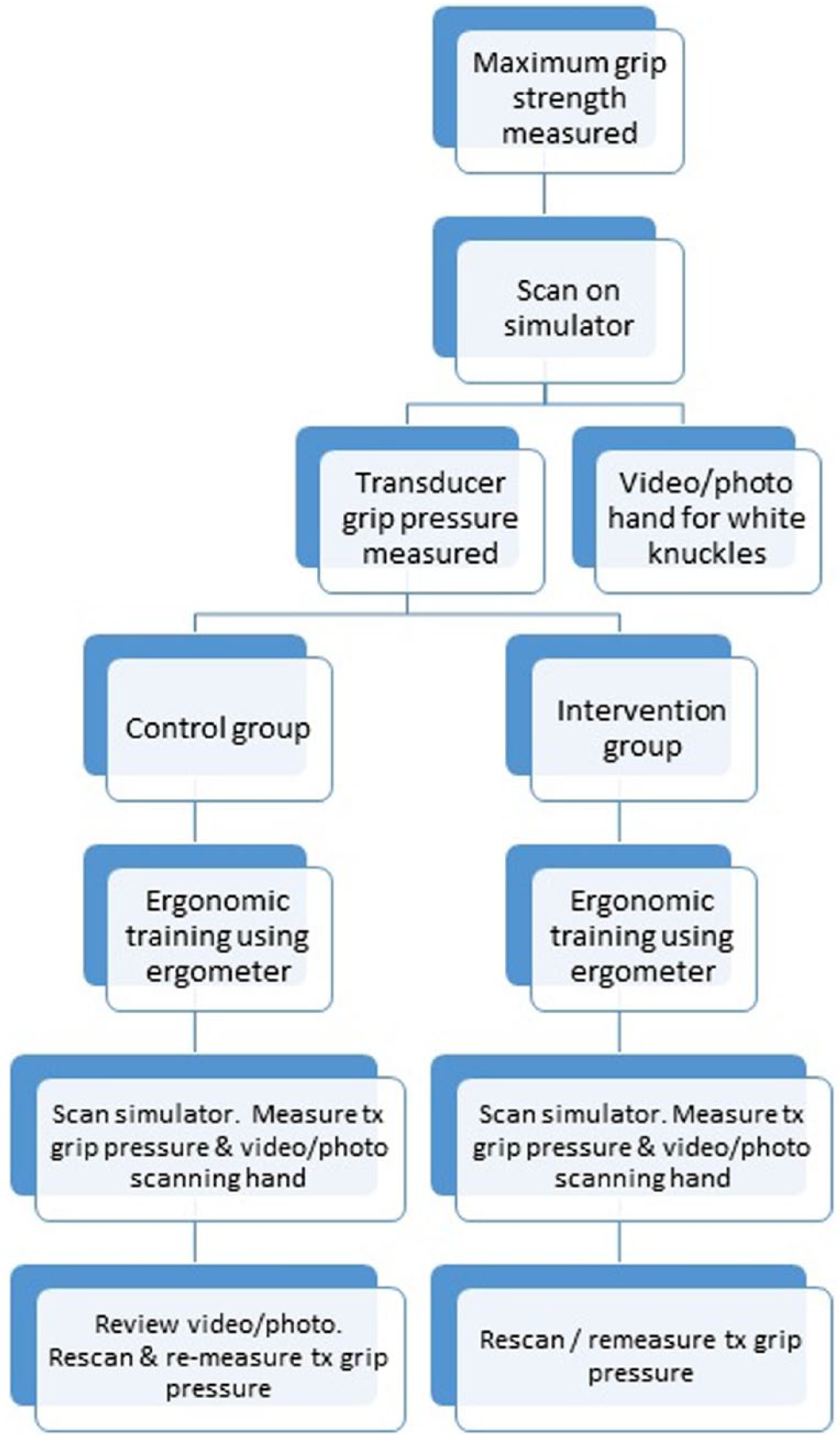
Flow diagram of the study method.
Measurements of maximum grip strength were used with the matched grip force to calculate the percentage of maximum grip force used to eliminate variables such as height, age, and gender, as used by Roberts et al. 17 Data were stored on an Excel spreadsheet, then quantitative analysis was undertaken using SPSS version 22. Parametric and nonparametric tests were used to assess whether the matched grip force changed with ergonomic training and again at final testing, irrespective of participant groups (intervention or control). A value of P ≤ .05 was used to indicate significance in all tests.
Results
Thirteen participants took part in the study, 7 (54%) of which were included within the video/image review intervention group. The subjects demonstrated a higher baseline grip strength for the right hand, mean = 34.33 kg, compared with the left hand, mean = 31.16 kg. No statistical difference existed in baseline grip strength between the two groups, right hand difference 0.057 kg, t = −0.012, P = .991; left hand difference 0.0238 kg, t = −0.0693, P = .946.
All participants scanned with the right hand. Predominant handedness was not assessed in this study. The control group had a slightly higher matched control grip pretraining, 2.63 compared with 2.34 in the study group, although this difference was not significant, t = −0.303, P = .767 (Figure 3). The posttraining grip strength scores did show a greater difference between the two groups, 0.657, than the pretest scores; however, the difference between the two groups was still not significant, t = −1.117, P = .2877. The average reduction in matched grip strength posttraining was 1.531, with both groups showing a significant reduction (t = 4.066, P = .039) of their grip strength after training (1.7 for the intervention group and 1.333 for the control group). All subjects except one (90.9%), who was in the intervention group, showed a reduction in matched grip strength after training.
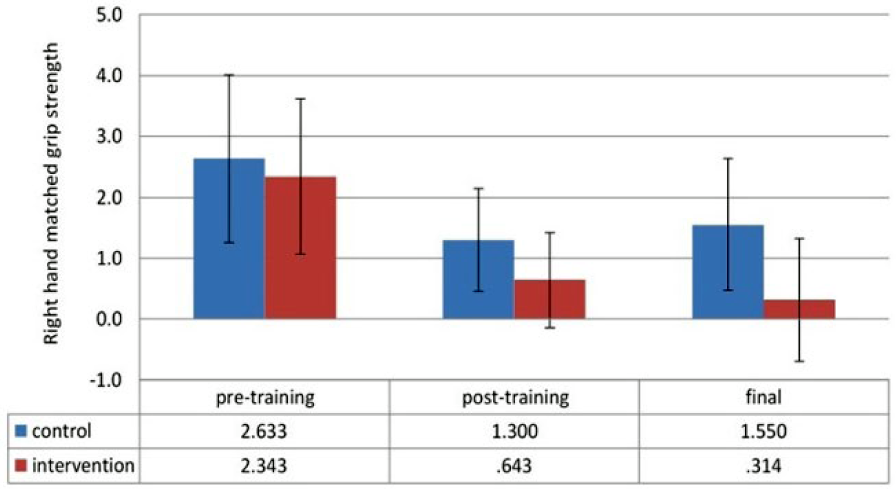
Effect of intervention on matched grip strength scores.
The final stage of the study, to investigate the effect of showing one group videos/photos of their training, demonstrated that showing the photo or video had more effect than doing nothing. The results showed that in the control group, there was a slight increase in average matched grip strength, 0.25, P = .8438, whereas there was a further small reduction, 0.328, P = .250, in matched grip strength for the intervention group (Figure 3).
Discussion
Previous literature suggests that transducer grip can impact sonographers, leading to pain and injury.2,3,5,12 Measurements of transducer grip force using recommended methods18,19 to determine matched grip force and simulate transducer grip force pre– and post–ergonomic training were taken. Matched grip force, as a percentage of maximum grip force, was used in this study to compensate for external factors, such as age, previous injury, and gender, which can all affect the results of maximum grip force. Further demographic data were not collected in this part of the study as data for maximum grip strength were collected as part of a wider study, 22 which limited the ability to compare data with previous work. The results of this study demonstrated that ergonomic intervention had a significant impact on participants’ matched grip force when holding the transducer after training. The hypothesis that review of video/photographs of poor practice in addition to the normal teaching demonstrated (Figure 4) might further reduce grip force was in the study, with a small reduction in the grip force. Monnington et al 9 had suggested that reviewing videos and photographs may be useful in the teaching of ergonomics; however, the results in this study showed that although a slight further reduction was demonstrated in the intervention group, it was not significant.

Photograph used to demonstrate poor transducer grip to a participant in the intervention group.
The findings of a study of information technology (IT) workers 24 demonstrated that direct intervention was more successful in changing habits than photographs without any human intervention. These findings may suggest that someone providing advice and support during the training might have a more profound impact on behavior. Similarly, other studies have demonstrated that ergonomic training with a facilitator in other non–health care settings can reduce the prevalence of WRMDS and strain.25,26 Hoe et al.’s 13 systematic review revealed limited compliance following training in ergonomics, although they found many of the studies to be of poor quality. Younger participants (<40 years) had a higher compliance rate than those over 40. The current study was not able to assess this as demographic data were not collected and numbers in the study were small.
The matched grip strength was calculated for each participant, with the mean percentage being 8%. Two respondents had a matched grip strength that was >17% of the maximum (one was 20%, the other 23%), suggesting that their transducer grip was much higher than many of the other participants. Bao and Silverstein 18 suggested that a matched grip strength over 17% of the maximum grip strength can lead to carpal tunnel syndrome. This information could be useful when teaching sonographers the risks of gripping the transducer too tightly.
It has been suggested that equipment developments may be able to reduce the need for sonographers to assert pressure on the transducer,10, 27 such as robotic echocardiography examinations. 28 Until such equipment developments are commonplace, it is still essential to ensure that sonographers are aware of the risks and ways to minimize these, including the need to reduce the transducer grip force. The use of one-to-one training for ergonomics is time consuming as even in this short intervention study, the trainer needs to be available for at least 30 minutes. This study only reviewed one case of a transabdominal early pregnancy examination. If a range of examinations such as gynecology, obstetrics, abdominal, transvaginal, vascular, and superficial structures was to be assessed, this could potential take one day per participant. However, the cost implications of the intervention should be compared to the individual and the employer should the sonographer sustain a WRMSD.
Ergonomic training has been highlighted as an effective way to reduce the risk of WRMSD.9,11,29,30 There are limited studies into how best to train sonographers in ergonomics, particularly with reference to transducer grip force. In the Health and Safety Executive (HSE) report, 9 it was suggested that local practical training should be incorporated into the practice, but financial support would need to be available to allow this to occur.
Limitations and Further Studies
As this study had a small sample size and a narrow focus, wider generalizations cannot be made. To try and reduce bias, this study used a standardized patient, by using the UltraSim, which has limitations when compared to scanning in the clinical situation. The simulator is less pliable than a patient’s abdomen, and the situation and controls are less familiar than the practitioners’ clinical department and equipment. In using the skills suite, there are no time pressures, unlike the clinical situations many sonographers work in, and the study only assessed one transabdominal case. The results can only be used as an indication that additional large-scale studies relating to ergonomic training may be of value in assessing ways to reduce the risk of WRMSD among sonographers. Further studies of this nature covering a range of different examination types within the participants’ own clinical setting would add to this work. Due to the nature of the study at the university, only one intervention was performed; further studies should consider having a larger sample size so that generalizations can be made and longitudinal follow-up to ascertain the long-term effects of the training intervention. If this study were carried out in a clinical department, it could also assess the effect on the matched grip force when scanning obese patients, which has been shown to impact on transducer grip force.10,31
The dynamometer provides a consistent method of measuring grip pressure, although bias could be introduced as participants were aware that the researchers wanted to determine whether there was any effect from the training. There are also inherent challenges of using matched grip force, as found in the study by Boa et al. 32
Many other factors influence a workers’ chance of developing a WRMSD,1,2,9,33 so further studies would benefit from addressing wider issues in addition to ergonomics and transducer grip.
Conclusion
This study has demonstrated that a short ergonomic teaching session using an ergometer to highlight when muscles are under strain during a sonography examination could reduce transducer grip force. Relaxing transducer grip could help reduce the chance of developing WRMSD among sonographers. The use of videos and photographs to demonstrate poor posture and positioning further reduced the matched grip force, but not significantly, in this small cohort. The study only used a very short intervention without longitudinal follow-up, and as suggested by the literature, WRMSDs are multifactorial, suggesting that more extensive intervention should be considered. Until new equipment developments are introduced to reduce the need for sonographers to use their own force to manipulate the transducer, particularly with the increasing obesity issues in society, sonographers would benefit from some form of education to help them reduce their risk of injury. It appears from this small study and other previous research that immediate instructor feedback and guidance might assist in this process of education.
Footnotes
Acknowledgements
The authors would like to thank all participants who undertook this study and the British Medical Ultrasound Society for disseminating the study information to delegates.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.