
Abstract
When describing carcinomas, poorly differentiated defines how little the tumor tissue resembles the normal tissue it came from. The origin of these types of tumors cannot be determined by histological findings alone. Imaging findings and patient history play a strong role in determining the source of the patient’s cancer. Imaging features of urothelial cancer of the renal pelvicaliceal system can be challenging for any sonographer or radiologist. When tumors are hyperechoic relative to nearby renal parenchyma, they may be obscured by the surrounding hyperechoic renal sinus fat, causing these carcinomas to be difficult to detect regardless of whether they are well defined or poorly differentiated. This case study delves into the difficulty in sonographically imaging a poorly differentiated transitional cell carcinoma without sonographic evidence of a primary circumscribed mass.
Introduction
Tumor grade is the description of a tumor based on its histology. If the cellular appearance of the tumor and the organization of the tumor’s tissue are similar to those of normal cells and tissue, the tumor is called well differentiated. In contrast, a poorly differentiated tumor will have abnormal-looking cells and may lack normal tissue structures.
Based on the microscopic appearance of the tumors, pathologists assign a numerical grade to most cancers. The factors used to determine tumor grade can vary between different cancer types. 1
Most tumors are assigned a grade of one through four, depending on the amount of differentiation. In grade one tumors, the cells and the organization of the tumor tissue are well differentiated and appear close to original cell structure. These tumors are slow growing and spread very gradually. In contrast, the cells and tissue of grade three and four tumors do not look like normal cells and tissue. These are considered poorly differentiated or undifferentiated. 1
An undifferentiated carcinoma is a cancer in which the cells are immature, unrefined, and do not look like cells they originated from. These cancers are a heterogeneous group of high-grade carcinomas composed of cells lacking distinct histological or cytological evidence of more specifically differentiated neoplasms. 2 Because the cells do not reveal the carcinoma origin, clinical information is often used to determine the likely primary. An undifferentiated carcinoma is usually more malignant than a cancer that is well differentiated because it grows and spreads aggressively. Poorly differentiated tumors account for approximately 2% of all malignancies diagnosed in the United States. 2 There is little information regarding how an undifferentiated carcinoma can change the medical imaging appearance of the tumor other than it is usually found in later stages and can alter the typical appearance in unusual ways.
Case Report
An elderly male presented to the hospital complaining of shortness of breath and dyspnea on exertion. He had also noticed occasional, mild abdominal pain for 2 months and an unintentional weight loss of about 40 pounds. An abdominal sonogram was ordered due to his elevated liver functions and prior abdomen pain. The patient also had bladder cancer several years prior with bladder resection.
The sonogram revealed a normal right kidney. Additional images showed an echogenic renal sinus in the left kidney with spiculations extending well into the renal parenchyma (Figures 1, 2), multiple enlarged abdominal lymph nodes, and ascites. Pyelonephritis was suggested as a possible differential, and a computed tomogram (CT) was performed as a follow-up procedure. Despite the unusual appearance of the left kidney on the sonogram, no obvious mass was demonstrated on the noncontrast CT (Figure 3). The CT images revealed a confluent nodal mass in the retroperitoneum surrounding the aorta at the level of the renal hilum. The appearance of the nodal mass was suggested as suspicious for lymphoma.

Longitudinal sonogram showing a homogeneous, prominent-appearing renal sinus with spiculations extending into the renal parenchyma (white arrow) without a well-circumscribed mass or disruption of the normal renal contours.
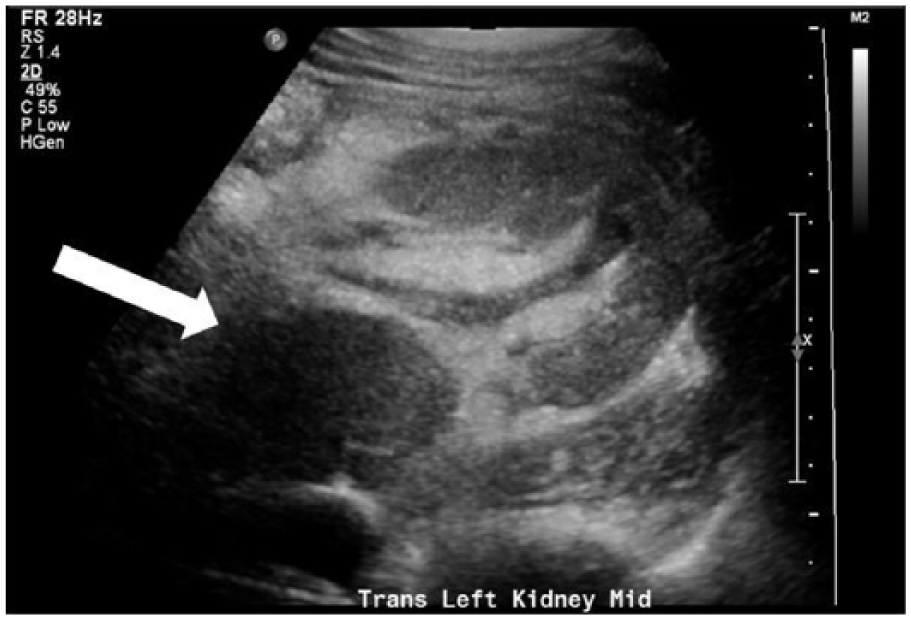
Transverse sonogram showing a homogeneous, prominent-appearing renal sinus without a well-circumscribed mass or disruption of the normal renal contours. Enlarged lymphnode seen as well (white arrow).
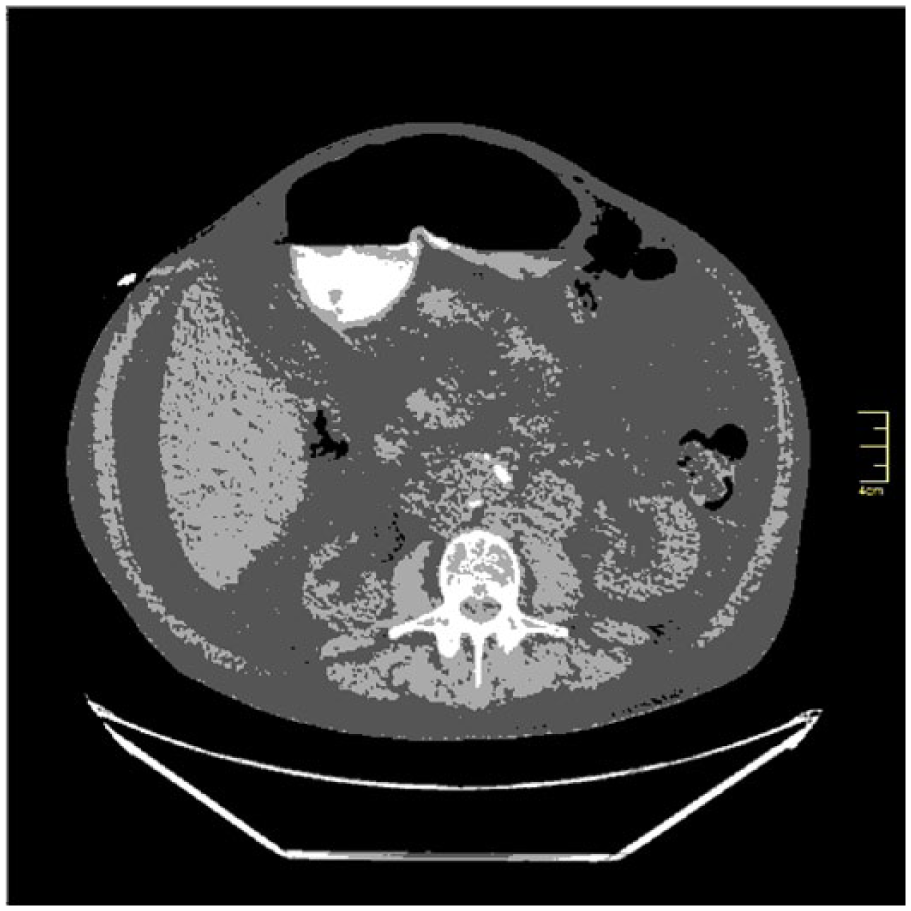
Transverse computed tomographic image of the renal pelvises.
A paracentesis was performed, and the cell count for ascites showed atypical epithelial cells consistent with metastatic carcinoma. A biopsy was planned for the nodal mass, but the patient died before it could be performed. An autopsy was conducted shortly postmortem, revealing a poorly differentiated carcinoma in the left renal pelvis with extensive lymphatic space involvement. The tumor infiltrated the left renal pelvis and left adrenal gland. Cause of death was determined as tumorlysis of a left kidney poorly differentiated carcinoma with widespread disseminated disease. Although the carcinoma was poorly differentiated, transitional cell carcinoma originating in the ureter or renal pelvis was determined the most likely cause given the patient’s history and the location of the tumor.
Discussion
Transitional cell carcinoma (TCC) is a type of cancer that typically occurs in the urinary system: the kidney, urinary bladder, and accessory organs. 3 Transitional cell carcinoma develops from the urothelium, which lines the renal pelvis, ureter, and bladder. Approximately 7% of diagnosed kidney cancers are TCCs.4,5 Smoking, chemical exposure, and certain medications can increase the risk of TCC. According to American Cancer Society, an estimated 64 000 kidney cancers will be diagnosed in the United States in 2017; however, deaths from urothelial malignancies have been decreasing since 1995. 6 Transitional cell carcinoma of the renal pelvis is uncommon compared to renal cell carcinoma and can be difficult to perceive with imaging. 7
Due to this patient’s infiltrating renal mass and past history of urinary transitional cell carcinoma, it was determined that TCC was most likely his cancer type. The most typical sonographic appearance of renal TCC is a hypoechoic, hypovascular mass in the renal collecting system that infiltrates the renal pelvis, splitting the central echo complex to varying degrees. 3
When a TCC infiltrates the renal pelvis, it can enlarge the kidney without distorting its shape. The entire kidney or only a portion of it may be involved. Sonographically, infiltrative processes often demonstrate poorly circumscribed areas of altered echogenicity as the tumor starts replacing renal sinus fat. 8 Although TCC masses can be either increased or decreased in echogenicity when compared to the normal renal sinus, when they are poorly differentiated and infiltrating the renal collecting system, these types of masses can become difficult to perceive sonographically. In this patient’s case, the involved kidney had a uniformly homogeneous, prominent renal sinus without a well-circumscribed mass. Despite its large size, the mass was difficult to distinguish with imaging.
Renal sonograms are often used to rule out tumors, stones, and hydronephrosis, but without an obvious reason for an unusual appearing kidney, a differential diagnosis can be challenging. Carcinoma may be easily dismissed as a possibility when there is not a circumscribed mass or a blockage causing hydronephrosis. In this patient’s case, after a sonogram revealed some unusual but inconclusive findings, CT was used to search for a primary tumor and evaluate for metastasis. The results of the CT also helped select a possible biopsy site.
Conclusion
Patients with urothelial cancer may present with variable and nonspecific symptoms, creating clinical uncertainty and prompting radiologic evaluation. Therefore, sonographers need to be familiar with both the usual and unusual sonographic manifestations of a poorly differentiated carcinoma. The role of imaging is to detect and diagnose atypical tumors as well as identify metastatic disease and complicating features so that patients receive appropriate staging and management.
Although sonography is useful in diagnosing obstructive uropathy, it is less sensitive for diagnosing early TCC. 2 Renal transitional cell carcinoma can easily be overlooked as hyperechoic or hypoechoic renal pelvis of uncertain significance or a treatable condition like pyelonephritis, despite it being an advanced grade. Transitional cell carcinoma can be isoechoic to or completely replace the renal sinus fat and be nearly imperceptible. When subtle abnormalities are visualized, it is important to consider an unfamiliar appearance of carcinoma as a possibility even when a circumscribed mass is not visible.
Footnotes
Acknowledgements
The author thanks Dr. Bret Abbott for his expertise and mentorship, Dr. Daryl Vogel for his insight into pathology, and Gabe Lopez, R.T(R)(ARRT) for the use of his computed tomography images.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.