
Abstract
Bladder cancer is a rare finding in young adults. This case demonstrates a 17-year-old female with an incidental bladder mass seen during a first-trimester obstetrical sonogram. Sonographic examination revealed a nonmobile, echogenic mass in the inferior portion of the patient’s bladder. The patient subsequently went to surgery at 18 weeks’ gestation where a cystoscopic resection was performed. The tumor was found to be a low-grade papillary urothelial cell carcinoma. The patient delivered at term without further complications. Early diagnosis of this bladder carcinoma led to prompt diagnosis and treatment for the patient. This diagnosis may not have been possible without the bladder being fully distended.
Urothelial carcinoma is the most common malignancy of the urinary tract and is the second most common cause of death among genitourinary tumors. However, bladder cancer rarely occurs in the first two decades of life; the average age at diagnosis is 65 years. 1 Young patients tend to present more frequently with noninvasive low-grade tumors, as in this case being presented.2,3
Case Report
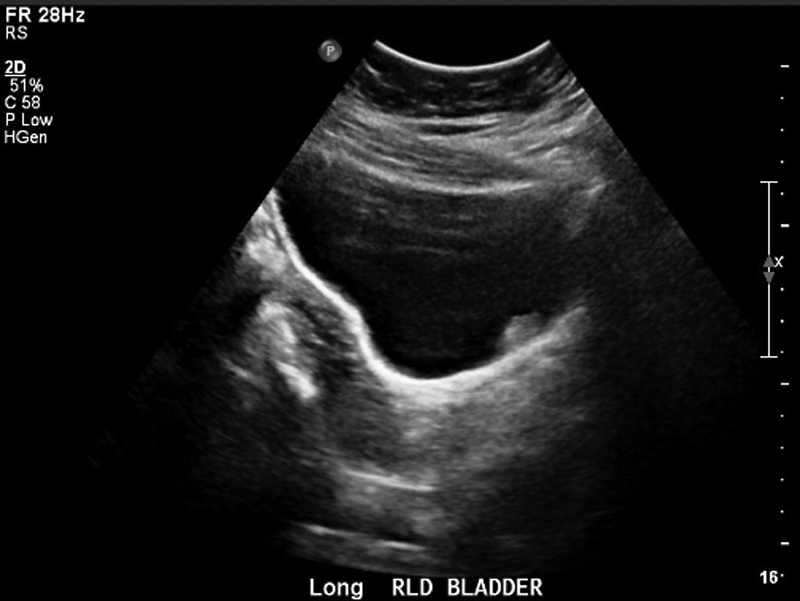
A 17-year-old female, gravida 1, para 0, presented to the emergency room with low back pain and spotting in her first trimester. An early obstetrical sonogram was ordered to evaluate the pregnancy. Prior to the examination, the patient’s bladder was filled with saline using a Foley catheter. A transabdominal sonogram was performed using a Philips I-U22 machine (Philips Healthcare, Bothell, Washington) with a C 5-1 probe. Upon examination, an echogenic, nonshadowing lesion measuring 1.5 × 1 × 1.2 cm was incidentally noted in the patient’s bladder (Figures 1 and 2). There was no mobility seen with position changes (Figure 3). In addition, the lesion had no flow demonstrated by color Doppler imaging (Figure 4). The patient had an otherwise normal early pregnancy, and sonographic dating estimated the gestational age to be 10 weeks, 2 days. The patient was later referred to an urologist where a cystoscopy was performed at 18 weeks’ gestation for resection of the tumor. Pathology confirmed the tumor to be low-grade papillary urothelial cell carcinoma. The patient later delivered at term without further complications. Of note, without the image quality provided by a full bladder, this diagnosis may have been missed, resulting in delayed treatment for the patient.

Sagittal view of the bladder demonstrating an echogenic mass in the posterior aspect of the bladder.

Transverse view of the bladder demonstrating the same mass.
Right lateral decubitus position showing mass still positioned to left of midline, demonstrating that the lesion is nonmobile.
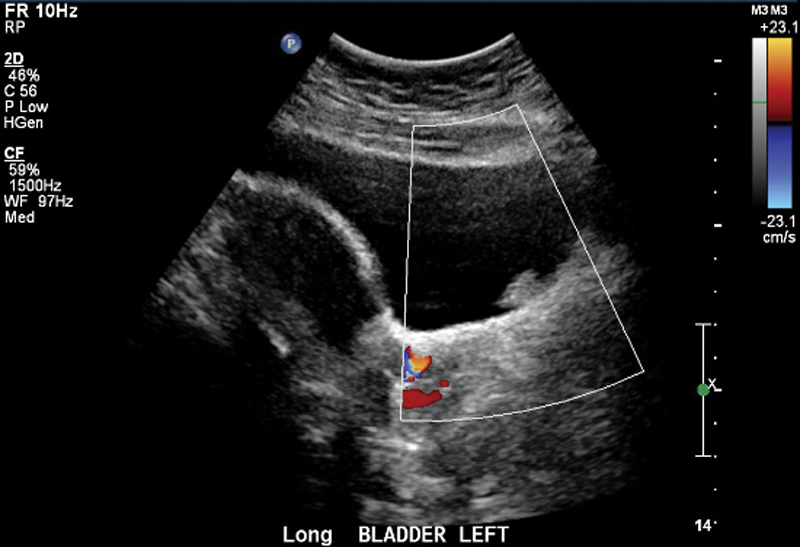
Sagittal view of the bladder with color Doppler imaging, showing no flow within the mass.
Discussion
Bladder cancer is rare in people younger than 40 years, and urothelial carcinoma typically has a male to female ratio of 4:1, 2 making this an unusual case in both aspects. Younger patients do present more frequently with noninvasive, low-grade tumors, as was seen in the case presented. 2 Most patients with bladder cancer present with hematuria. Gross, painless hematuria is the primary symptom in 85% of patients with a newly diagnosed bladder tumor, and microscopic hematuria occurs in virtually all patients. 3 A large number of patients have additional symptoms such as irritative voiding, including urgency, frequency, and dysuria, with their symptoms mistakenly attributed to urinary tract infections. 4 In this case, urothelial carcinoma was identified early, and the patient did not have any of these symptoms. Her urine was negative for hematuria, and there were no voiding or frequency complaints.
An important feature of the sonographic examination that made the early diagnosis possible was the full bladder; without this, the diagnosis may have been delayed until symptoms occurred. Although there remains some controversy over the need for complete bladder distension during obstetric sonography, a number of authors have cited the advantages of this in providing improved visualization of the uterine-bladder interface. Adequate bladder distension is considered one of the factors influencing the sensitivity in detecting bladder tumors, along with lesion size and patient obesity.5–7
A full hematuria evaluation for bladder cancer consists of cystoscopy, urine cytology, upper-tract imaging (primarily computed tomography [CT] of the abdomen and pelvis), and a prostate-specific antigen (PSA) blood test. The principal diagnostic test for bladder cancer is cystoscopy and biopsy. Prompt cystoscopy with transurethral resection is the treatment of choice for small superficial bladder tumors, a treatment that can be easily and safely performed even during pregnancy. 7 A PSA blood test is recommended because 10% of patients with recurrent gross hematuria will have prostate cancer. Microscopic hematuria carries a 5.4% risk of urological malignancy and a 4.1% risk of bladder cancer. 3 Patients with microscopic hematuria require a full evaluation, including cystoscopy, but low-risk patients do not require repeat evaluations. Risk factors for urothelial cancer are classified into one of three categories: (1) a genetic abnormality that results in perturbations in cell cycle regulatory process, (2) chemical exposure, and (3) chronic irritation. 8 High-risk patients and those with a smoking history should be evaluated every 6 months.
Conclusion
This case presents an incidental finding of bladder cancer in a young patient during an early obstetrical sonogram, which was confirmed with cystoscopy. The case was a rare finding of bladder cancer presenting without the usual symptoms and early in life in a female patient. One key to good visualization of this incidental finding was having a full bladder for the obstetrical sonogram. Although CT is considered the primary imaging examination for evaluation of suspected bladder cancer, such lesions can be found with sonography when good technique is used, reducing patient cost and radiation exposure.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.