
Abstract
This case presentation describes the early diagnosis of an invasive urinary bladder cancer in a woman in her late 60s with no history of cancer, hematuria, dysuria, smoking, or hormone replacement therapy. This was confirmed on histopathology after tumor resection. The case report demonstrates the importance of including scanning the urinary bladder in all pelvic sonography examinations, even in the low-risk population. The following study also discusses the prevalence, etiology, diagnostic tools, prognosis, and treatment of bladder cancer. Different types of bladder tumors, staging, and grading criteria are also described.
Bladder cancer is one of the 10 most frequently diagnosed types of cancer. 1 Among men, it is the fourth most common cancer, and it is the ninth leading cause of death from cancer. The ratio of men to women who develop bladder cancer is 3:1. 2 Bladder cancer has a tendency to recur, and with recurrence, a significant number of cases progress, which makes the detection of high-risk patients extremely important. 3
The most common type of bladder cancer is urothelial (transitional cell) carcinoma. 4 Out of newly diagnosed bladder cancer cases, about 70% to 80 % will be non–muscle-invasive disease. Despite treatments, approximately 50% to 70% of these will return, and 10% to 30% of these cases will progress to muscle-invasive disease.5,6 Most recurrences appear within five years. 7 Over the years, staging and grading criteria have been used to predict progression. Accurate and reliable imaging is also critical in the management of bladder cancer. A delay in diagnosis of bladder cancer increases the risk of death from this illness independent of tumor grade or disease stage. 8
The following case represents sonographic detection in a woman with non–muscle-invasive bladder carcinoma.
Case Report
A woman in her late 60s was referred by her primary care physician to a gynecology office with symptoms of pinching sensations in the suprapubic area. The patient had a history of four cesarean sections, no history of vaginal bleeding, no gross hematuria, and no history of cancer. Her recent Papanicolaou test (Pap smear) was negative. Other history included a urinary tract infection approximately one year ago, normal laboratory values for standard blood tests, and a negative urinalysis. In general, the patient was healthy, was a nonsmoker, did not use alcohol, and woke up to urinate once or twice during the night.
A pelvic transabdominal sonogram was performed with a full bladder using a GE Voluson Expert System (General Electric, Milwaukee, Wisconsin) sonography unit with a curved linear multifrequency (2–7 MHz) probe. The uterus and ovaries were noted to be normal. The contour and texture of the endometrial lining was unremarkable, with a normal thickness of 1.2 mm. Color Doppler imaging showed no vascular flow within the endometrial stripe. There was no free fluid present anywhere in the pelvic area. The full bladder was scanned in multiple longitudinal and transverse planes. The bladder wall was normal in thickness (3 mm); however, upon careful observation of the right lateral wall, an echogenic, irregular, and partially vascularized mass measuring 1.7 × 1.5 cm was seen (Figures 1 and 2). Evaluating the patient’s kidneys showed no evidence of hydronephrosis. The right kidney had a bilobed cyst measuring 4.6 × 3.45 cm extending into the renal pelvis. No other renal abnormality was seen. Postvoid sonography showed complete emptying of the bladder. The patient was not able to tolerate an endovaginal examination secondary to significant discomfort.
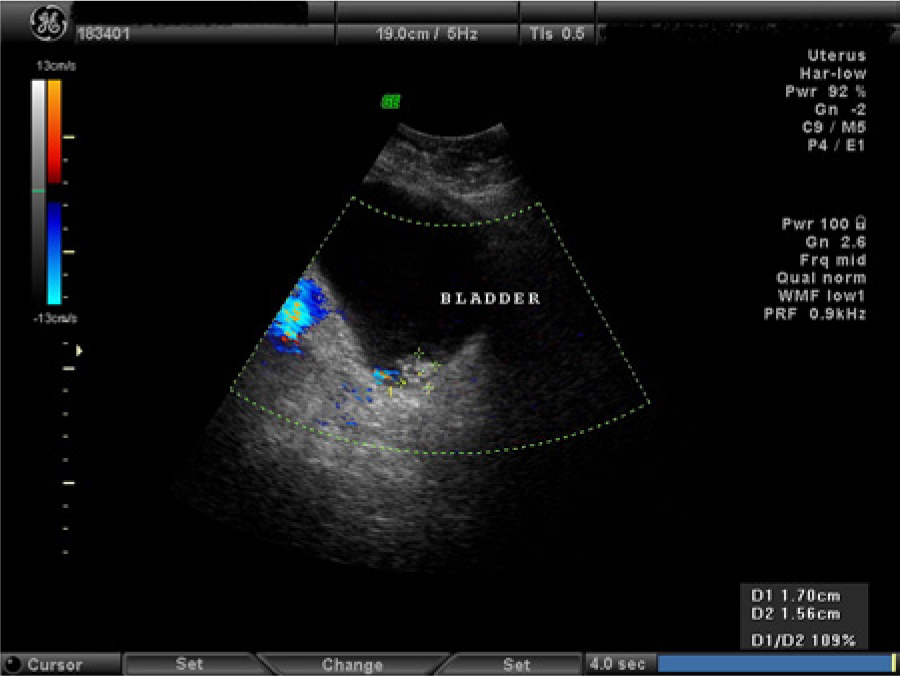
Parasagittal image of the bladder wall showing the irregular echogenic tumor, with color Doppler demonstrating partial vascularity within the mass.
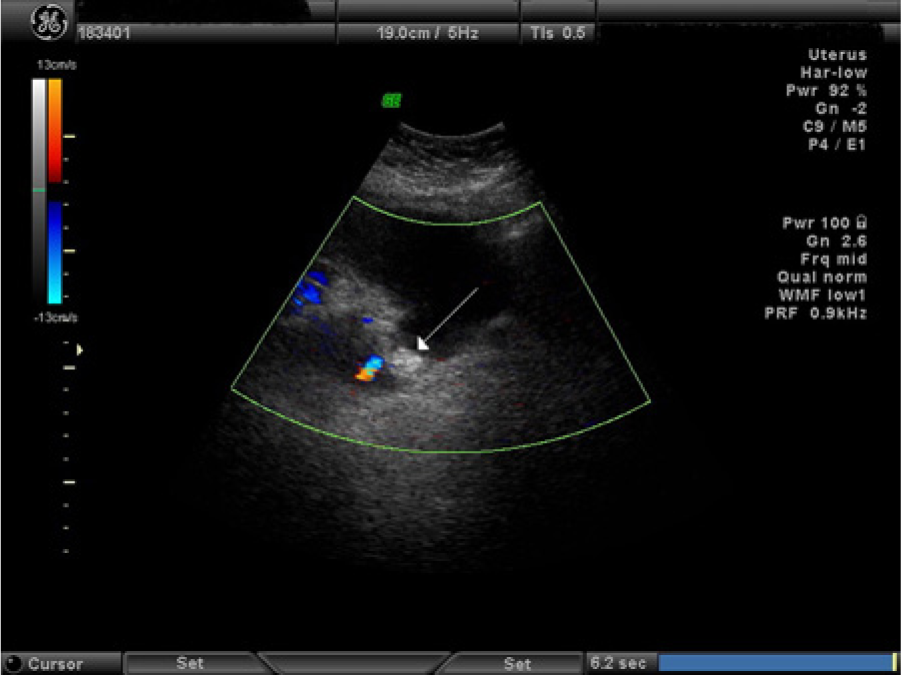
Transverse color Doppler image of the bladder showing the bladder wall mass (arrow).
The patient was referred to a urologist, and a cystoscopy procedure was performed, which confirmed the location and size of the mass as seen on the sonography examination. A transurethral resection of the bladder tumor (TURBT) was done, and the postsurgical pathology examination of the excised tumor confirmed low-grade papillary (non–muscle-invasive) urothelial carcinoma.
A few weeks following the surgical procedure, the patient was advised to start intravesical Bacillus Calmette-Guerin (BCG) therapy, with future cystoscopies scheduled to evaluate for any recurrence.
Discussion
Bladder cancer has many known risk factors, although many cases arise with no obvious exposure to carcinogens. 9 Age itself is a risk factor for developing bladder cancer as it is more prevalent in older patients. The median ages of men and women presenting with bladder cancer are 72 and 74 years, respectively. 10 Cigarette smoking is the strongest risk factor for acquiring bladder cancer. 11 After four years of smoking cessation, the risk of bladder cancer has been noted to be reduced by up to 40%, 12 which emphasizes the physician’s significant role in counseling patients who smoke. Although the specific carcinogens in cigarette smoke responsible for increasing the risk of bladder cancer are largely unknown, aromatic amines are suspected at this time to be responsible factors. 13 Many chemicals also are considered carcinogens for bladder cancer, including aniline dyes often used in color fabrics and chemicals applied in the painting and leather industries, paper and rubber factories, dry cleaning stores, and hair salons.14,15 Bladder cancer from occupational exposures often does not occur until 30 to 40 years after exposure. 9 Urinary tract infections, chronic irritation from catheters, bladder stones, or a nonfunctioning bladder are also associated with an increased risk of certain types of bladder cancer.16,17 Family history of bladder cancer is a known risk factor for bladder cancer, but new data have shown a family history of other types of cancer can be a contributing factor as well. 18
Bladder cancer may be detected incidentally or due to symptoms. Hematuria occurs in up to 85% of patients with bladder cancer. 19 Urinary frequency or dysuria can also be the presenting symptoms. Since urinary tract infections are more common in women, misinterpretation of hematuria and irritative voiding symptoms can result in delayed diagnosis in women, therefore resulting in a more advanced stage when bladder cancer is ultimately diagnosed.20,21
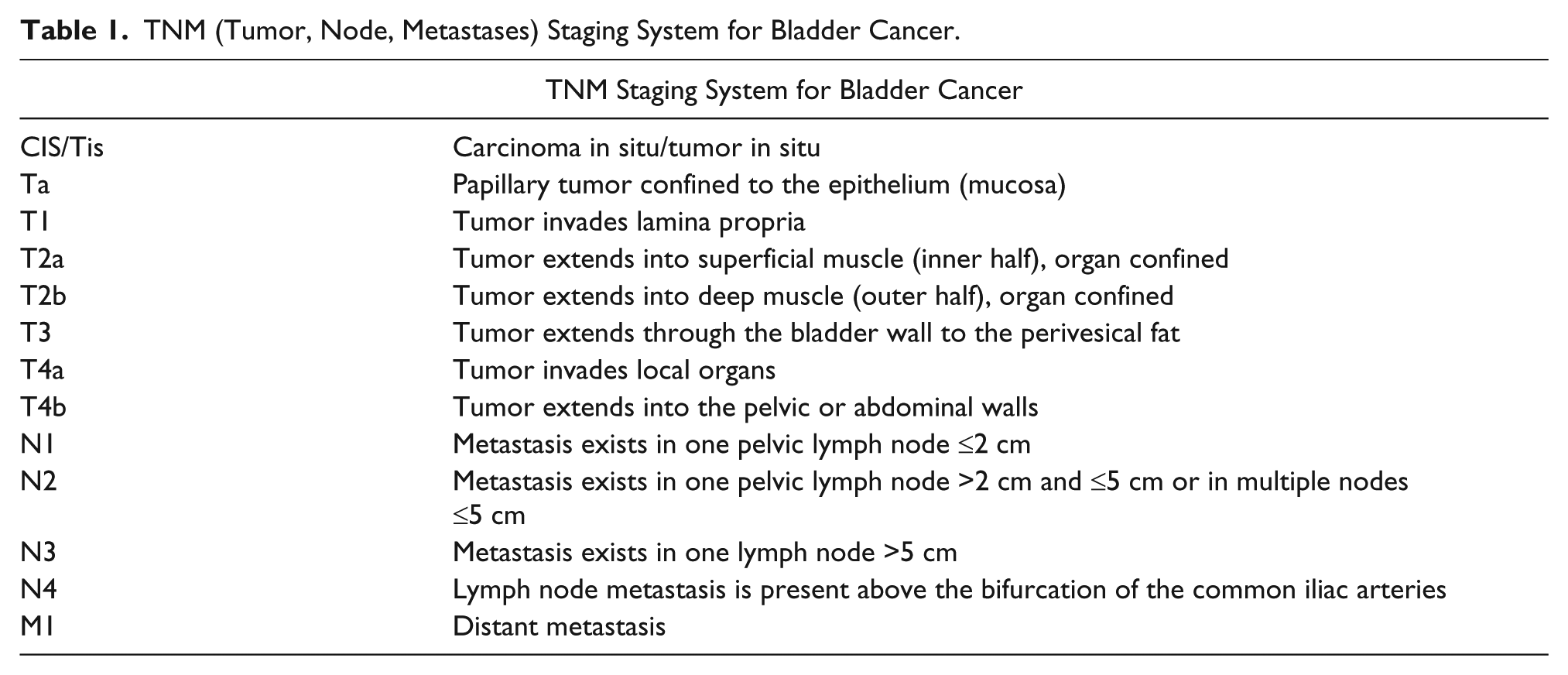
The original pathologic TNM (tumor, node, and metastasis) staging system is explained below and shown in Table 1. Non–muscle-invasive tumors do not invade the muscularis propria; they include lesions that are confined to the mucosa (Ta), such as the patient in the case report above and carcinoma in situ (CIS or tumor in situ [TIS]), and those that invade below the basement membrane into the lamina propria (T1). Carcinoma in situ (CIS or TIS) is a flat, high-grade, noninvasive bladder cancer with a very high rate of recurrence and advancement within five years if not treated. 22 All lesions that invade the lamina propria are called T1 lesions. Organ-confined disease (T2a and T2b) has a better prognosis than disease that has extended through the bladder wall to the perivesical fat (T3). 23 Urothelial carcinomas that invade local organs (T4a) and those that extend into the pelvic or abdominal walls (T4b) indicate a challenging disease stage that often requires multimodality therapy. Studies have shown that overall survival is worse with higher-staged cancer.24,25 Lymph nodes are also more likely to be involved in higher stages of primary bladder cancer, and in these cases, the overall five-year survival (34%) is extremely worse. 24
TNM (Tumor, Node, Metastases) Staging System for Bladder Cancer.
In addition to pathological staging of bladder tumors, the World Health Organization (WHO) has the most extensively employed classification system for grading urothelial neoplasms.
26
Grade 1: (A) PUNLMP (papillary urothelial neoplasm of low malignant potential and (B) low-grade papillary urothelial carcinoma Grade 2: Low grade or high grade depending on the interpretation of the pathologist Grade 3: All high grade
The current TNM pathologic staging system has also changed to low-grade and high-grade categories to match the WHO grading system. 27 The patient in the above study had the low-grade classification.
Conventional cystoscopy is the “gold standard” for the detection of bladder cancer. 28 Urinary cytology or markers are also used in the detection of bladder cancer, but they cannot safely replace cystoscopy. The limitation of urinary cytology is its low sensitivity for low-grade recurrences. 29 Imaging plays a critical role in the evaluation of patients with bladder cancer, especially for diagnosis, local and distant staging, and treatment follow-up. Sonography is now being accepted as a first-line imaging technique with increased sensitivity in the detection of masses compared with an intravenous pyelogram (IVP). Sonography has the additional advantages of being noninvasive, readily available, and cost-effective. 30
Careful and thorough imaging must be done when sonography shows a focal bladder mass. An essential technique in differentiating a fixed lesion versus an entity that demonstrates movement would be to image the “mass” in both decubitus views. Additional imaging with real-time “cine-clip” acquisition is most beneficial to demonstrate this characteristic. Bladder stones with or without shadowing, layered sludge, a collection of urinary crystalline casts from long-term urinary bladder catheters or stents, and retained ureteral stent fragments often display movement. Potential pitfalls for a fixed bladder wall focal mass can be inflammatory thickening of the ureteral orifice as well as an inflammatory pseudolesion. Color and spectral Doppler imaging further aids in differentiating a tumor mass from other possible findings, such as a blood clot, by demonstrating blood flow within a neoplasm. 31
After the initial assessment with sonography, recent technical advances in multidetector computed tomography (CT, especially CT urography) establish it as the preferred imaging modality for diagnosis and staging of bladder cancer. Computed tomography provides valuable findings about local, lymph node, and distant metastases in a single test. 32
At initial diagnosis, 80% of urothelial tumors are located at the bladder base; 60% are single, and more than 50% measure less than 2.5 cm at cystoscopy. 31
In patients with non–muscle-invasive bladder carcinoma, complete transurethral resection of the bladder tumor (TURBT) is diagnostic, prognostic, and often therapeutic. 33 This procedure is performed to prevent cancer recurrence and possible advancement to muscle-invasive disease for the purpose of decreasing cancer-specific mortality. In managing a patient with non–muscle-invasive bladder cancer, a clinician may decide to perform a repeat TURBT along with intravesical chemotherapy preoperatively, postoperatively, or at the time of tumor resection. Supplementary intravesical immunotherapy is another treatment option to diminish the risk of recurrence. 34 In general, after tumor resection, frequent cystoscopy at designated intervals is recommended. This allows the detection of recurrence at an earlier stage, thus lowering the progression rate and advancement to muscle-invasive disease. 35
For organ-confined muscle-invasive bladder cancer, most patients are treated with a radical cystectomy, with the possibility of neoadjuvant chemotherapy. 24 Studies report a 45% to 66% five-year overall survival rate after radical cystectomy. Partial cystectomy is a bladder-sparing surgical option for very carefully selected patients with muscle-invasive bladder cancer. 36 The presence of CIS on an initial TURBT or in the partial cystectomy specimen and the presence of lymph node involvement are highly predictive of tumor recurrence, and these patients are considered poor candidates for partial cystectomy. 37 If the tumor size is equal to or less than 4 cm and a low stage (equal to or less than T3a) is present, a dual treatment of chemotherapy and radiotherapy is often considered to preserve the bladder. 38
The prognosis for patients with metastatic bladder cancer is poor, with a median survival time of about 12 to 15 months. 39 Patients with muscle-invasive bladder cancer need to be closely monitored. After a cystectomy, urine cytology, electrolyte, and creatinine levels should be done on a regular basis. In addition, a chest x-ray along with abdominal and pelvic imaging is recommended every 3 to 12 months for two years and as clinically indicated.
As many as 31% to 47% of deaths from bladder cancer are potentially avoidable, emphasizing the need for earlier diagnosis of this disease, early cystectomy for highly aggressive tumors, and making earlier therapeutic decisions to increase patients’ survival rates. 40 The challenge for sonographers will be to offer the best care possible for our patients by consistently imaging the bladder wall and its contents in all pelvic sonograms. This case report showed a malignant bladder tumor at a very early stage where the cancer was still organ confined. No lymph nodes were affected, and there was no angiolymphatic invasion. In this study, because of the very early diagnosis, the bladder could be preserved.
Footnotes
Acknowledgements
Special thanks to Terre L. Osterkamp, MD, FACOG, at Verdugo Hills Obstetrics and Gynecology for her support and help with the manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.