
Abstract
Midgut malrotation is a congenital condition resulting from incomplete normal intestinal rotation after physiologic gut herniation. While it can remain asymptomatic over an entire lifetime, midgut volvulus is most likely to occur during early life. While an upper gastrointestinal series is the imaging modality of choice for definitive diagnosis, sonography is a safe and effective modality capable of indicating midgut malrotation, especially in pediatric patients. This case study illustrates the sonographic findings associated with intestinal malrotation with volvulus and discusses the etiology, signs, symptoms, and treatment of the condition. In addition, the sonographic findings are correlated with upper gastrointestinal results, which confirmed midgut malrotation. The diagnosis of volvulus secondary to midgut malrotation was confirmed by a laparoscopic Ladd procedure performed to treat the neonate.
Midgut malrotation can occur in several degrees, all as a result of incomplete or abnormal rotation of the midgut structures. 1 The majority of cases of midgut malrotation remain asymptomatic, with volvulus occurring most often within the first month of life. 2 Fluoroscopic upper gastrointestinal (UGI) contrast imaging is typically used to diagnose midgut malrotation by identifying the improper course of the duodenum. Although gastrointestinal sonography is not classically used to detect midgut malrotation, gray-scale and Doppler sonography can detect a reversed relationship between the superior mesenteric artery (SMA) and superior mesenteric vein (SMV) that is commonly associated with the condition. 3 A case of neonatal midgut malrotation and volvulus is presented that was initially identified on sonography. Inversion in the SMA/SMV relationship was identified sonographically, followed by fluoroscopic UGI contrast study. Upon treatment of the condition by a laparoscopic Ladd procedure, the diagnosis of volvulus secondary to midgut malrotation was confirmed. This report details the initial sonographic findings and the follow-up studies used to diagnose and treat midgut malrotation with volvulus. Sonography is an invaluable diagnostic imaging modality in the pediatric population, and this case is offered to review the imaging features associated with midgut malrotation and volvulus and the role that sonography can play in the evaluation of pediatric gastrointestinal disorders.
Case Report
A 4-day-old, 37-week gestational boy presented to a pediatric emergency department with a history of one episode of nonprojectile bilious emesis earlier that morning. Abnormal laboratory values included elevated levels of the following: absolute granulocyte, absolute monocyte, absolute eosinophil, absolute basophil, mean corpuscular hemoglobin concentration, red cell distribution width, total bilirubin, and indirect bilirubin. Elevated levels of these blood components generally indicate infection. Bilirubin is excreted through bile into the duodenum and is elevated in cases of intestinal obstruction. A limited abdominal sonogram was ordered for suspected pyloric stenosis. Sonography was performed with a GE LOGIQ E9 ultrasound machine with an ML6-15 MHz linear-array transducer (GE Healthcare).
The sonogram revealed a normal pyloric channel length and normal transverse muscle diameter, measuring 0.18 cm (Figure 1). Air was visualized coursing from the stomach to the duodenum and documented with a cine clip (Figure 2). These findings indicated that the neonate tested negative for pyloric stenosis. Per hospital protocol, documentation of the relationship of the SMA, SMV, and third section of the duodenum is required following evaluation of the pylorus. Normal sonographic presentation of this anatomy includes the SMA on the left, the SMV on the right, and the third section of duodenum coursing between the SMA and aorta. Examination of the SMA and SMV revealed a reversed relationship, with the SMA visualized on the right and the SMV on the left (Figures 3 and 4). The whirlpool sign of the SMV was visualized and captured in its entirety while sweeping superior to inferior (Figure 5), which is indicative of midgut volvulus. 4 The whirlpool sign describes the appearance of the SMV wrapping around the SMA and is best visualized with color Doppler imaging.
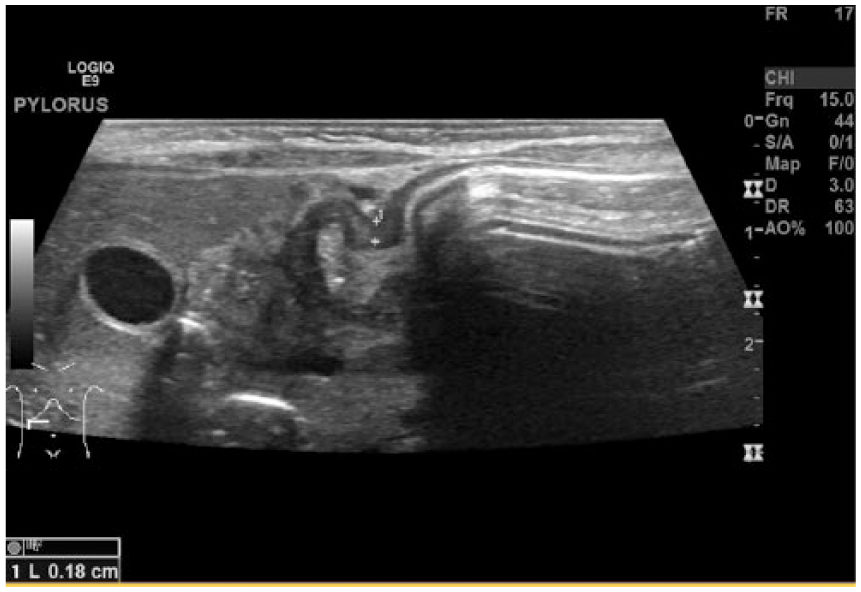
Transverse gray-scale sonogram of the pylorus showing a normal pyloric muscle diameter, measuring 0.18 cm.
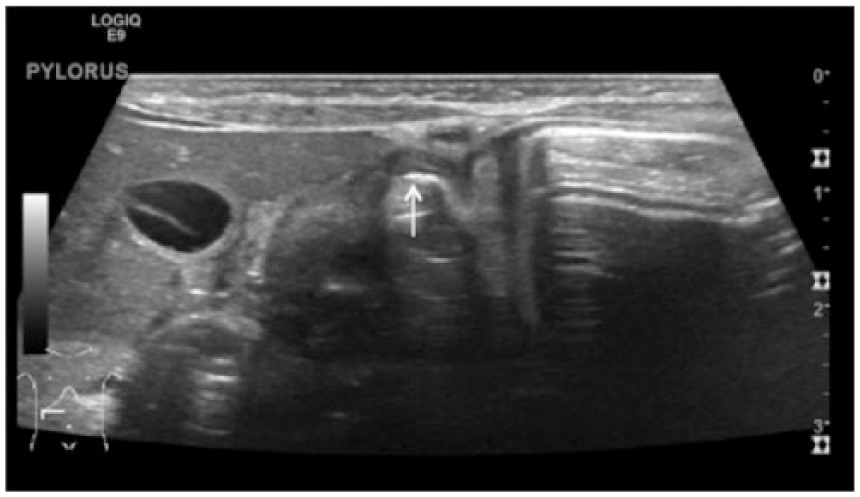
Transverse gray-scale sonogram of the pylorus demonstrating air coursing through the pylorus.
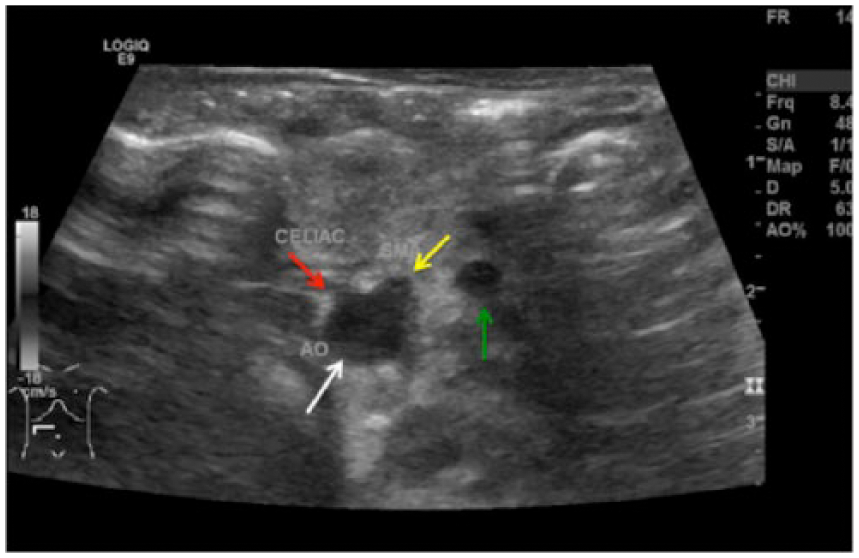
Transverse gray-scale sonogram of the aorta (AO; white arrow), celiac axis (red arrow), SMA (yellow arrow), and SMV (green arrow), showing a reversal in the relationship of the SMA and SMV. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
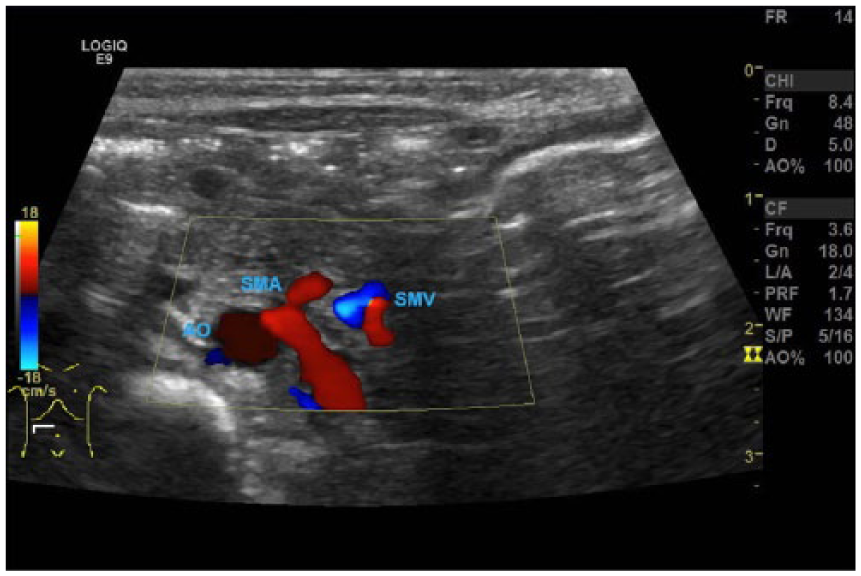
Transverse color Doppler sonogram showing a reversed SMA/SMV relationship, with the SMA on the right and the SMV on the left. AO, aorta; SMA, superior mesenteric artery; SMV, superior mesenteric vein.
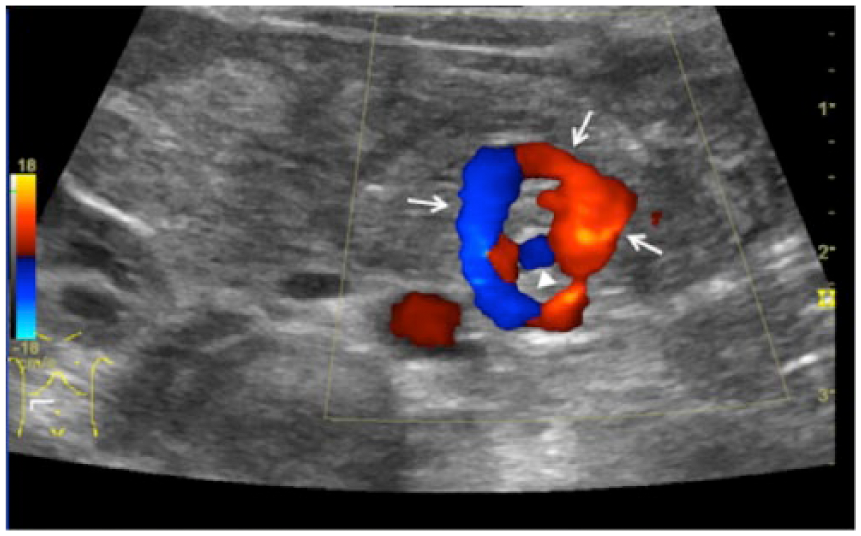
Transverse color Doppler sonogram showing the swirling pattern of the superior mesenteric vein (arrows) wrapping around the superior mesenteric artery (arrowhead), known as the whirlpool sign.
As visualization of a reversed SMA/SMV relationship is concerning for midgut volvulus, a fluoroscopic UGI contrast study was recommended to confirm the diagnosis. The UGI series was performed on the same day, and it showed contrast emptying into the proximal duodenum normally, confirming sonographic visualization of a normal pylorus. Contrast did not cross midline to the left and never extended posteriorly, which is expected of a normally rotated duodenum (Figure 6). Based on these findings, a diagnosis of high-grade upper intestinal obstruction was made, and underlying malrotation of the midgut previously identified on sonography was confirmed.
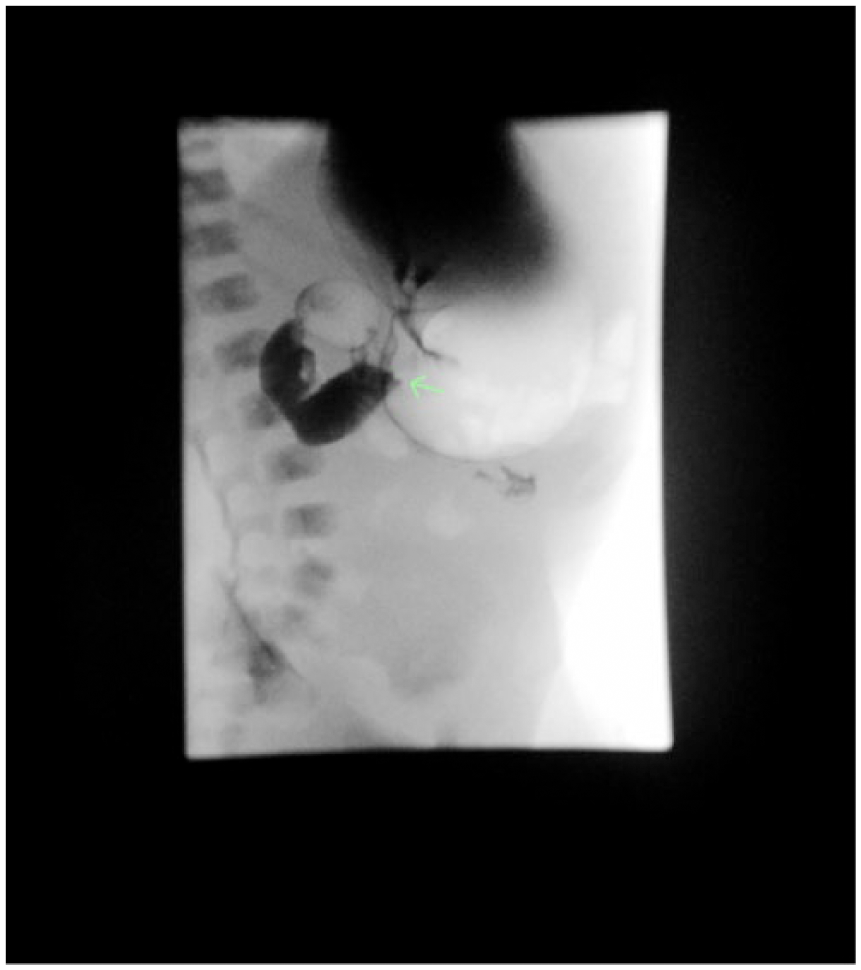
Fluoroscopic upper gastrointestinal contrast study showing obstruction at the duodenum as indicated by a lack of contrast continuing through the distal duodenum, with the arrow demarcating the level of midgut obstruction.
Surgical intervention with diagnostic laparoscopy and the Ladd procedure was performed the same day. Upon entry into the abdominal cavity, malrotation and volvulus were clearly identified, with a large amount of fluid. The surgeon identified the small bowel largely on the right of the abdomen and the large bowel mostly on the left, indicative of malrotation. A substantial number of adhesions and Ladd bands were identified and removed successfully. The bowel was mobilized throughout its length twice, and volvulus was decompressed. The patient tolerated the procedure well and was extubated in the postanesthesia care unit before being taken back to the neonatal intensive care unit. After an uneventful hospital stay of 18 days, the patient was discharged. A follow-up appointment was scheduled 2 weeks after discharge, and the parents reported the infant feeding well without presence of any new symptoms.
Discussion
Congenital intestinal malrotations occur in 1 per 200 to 500 live births, 1 with the majority of individuals remaining asymptomatic throughout the lifetime. Incomplete or abnormal rotations present in many ways, but all involve atypical rotation of the midgut structures around the SMA (Figure 7). 1 During embryology, extremely rapid growth of the bowel causes physiologic gut herniation, where the bowel protrudes into the base of the umbilical cord for a time before returning to the abdominal cavity. Normal physiologic gut herniation results in the duodenojejunal junction being positioned at the left side of the body, and return of the bowel in the 10th week results in the cecum being positioned on the right.1,3 Fixation subsequently occurs by week 12, attaching the midgut to the abdominal wall. 5 As this represents a rotation of 180° counterclockwise from the former position of the intestines, this process is known as intestinal rotation. Any time the intestines do not rotate a full 180° is known as malrotation. 3
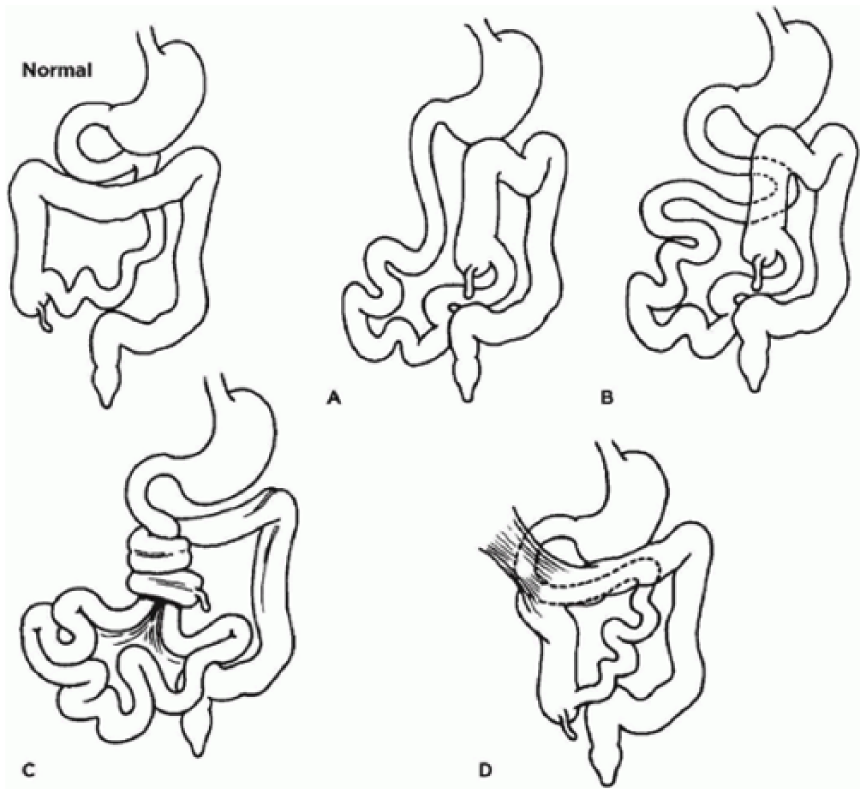
Drawing of various midgut rotation abnormalities. (A, B) Nonrotation. (C) Midgut malrotation. (D) Ladd bands. Source: Basic Medical Key, https://basicmedicalkey.com/the-gastrointestinal-tract-7/.
Malrotation comes in many forms, including nonrotation, reverse rotation, malrotation with volvulus, and malrotation without volvulus. 3 Nonrotation occurs as a result of the proximal foregut returning to the abdomen before the cecocolic loop. When this occurs, the duodenum and jejunum are not forced to rotate, resulting in nonrotation of the midgut. 3 Least commonly, the fetus may have reversed rotation, in which the bowel turns 90° clockwise instead of counterclockwise. In this case, the SMA will lie posterior to the duodenum and may result in vascular or lymphatic obstruction. 3
Midgut malrotation with volvulus has classically affected males more than females but has also been reported as having the same predominance. 6 Associated anomalies include situs inversus, right isomerism, left isomerism, and cardiac defects. 7 Symptoms of midgut malrotation with volvulus include bilious vomiting, abdominal pain, hematochezia, peritonitis, and death. Bilious vomiting occurs as a result of Ladd bands, duodenal atresia, or midgut volvulus. 3 In this case, Ladd bands and midgut volvulus were both present. Ladd bands, or abnormal peritoneal bands, fix the bowel to structures of the right upper quadrant, such as the gallbladder or liver, and must be dissected to correct the malrotation and volvulus. 3 Midgut malrotation does not always lead to volvulus and is often asymptomatic. However, when symptoms do occur, they are most common in the first few months of life, with 75% to 85% of symptomatic malrotations diagnosed within the first year of life. 1
Volvulus is corrected with the Ladd procedure, and a laparoscopic Ladd procedure was performed in this case. Ladd bands are common and numerous in these patients and can cause duodenal obstruction and abnormal fixation of the malrotated bowel to the abdominal wall or other abdominal organs. During the procedure, these bands are dissected completely. The bowel is then mobilized completely and returned to the abdomen in the correct fashion. Appendectomy is also performed during a Ladd procedure. A recent study compared open and laparoscopic Ladd procedures and found the latter just as safe and effective as the former. 3 The laparoscopic Ladd procedure led to earlier postoperative feeding, decreased wound infections, earlier discharge, and smaller risk of incisional hernia.3,8 The Ladd procedure has an 11% risk of perioperative mortality, with 22.2% total mortality. 6 Possible postoperative complications include short gut syndrome, wound infections, malabsorption, abdominal pain, bowel obstruction, and adhesion formation. 9 Postoperative complications occur in 46% of individuals who have undergone the Ladd procedure. 9
On the sonogram, the SMV typically lies posterior to the pancreatic neck and anterior to the uncinate process, with the SMA lying posterior to the pancreatic body (Figure 8). When this relationship is reversed, it is suspicious for midgut malrotation. A classical sign of midgut malrotation with volvulus is the whirlpool sign of the SMV wrapping around the SMA. When volvulus occurs, the twisting of the mesentery brings the SMV along, and the SMV becomes wrapped in a circular fashion around the SMA. 4 The term whirlpool describes the visualization of the SMV swirling on color Doppler as it is wrapped around the SMA. This sign is best visualized with color Doppler and can be confirmed with venous spectral Doppler tracings.
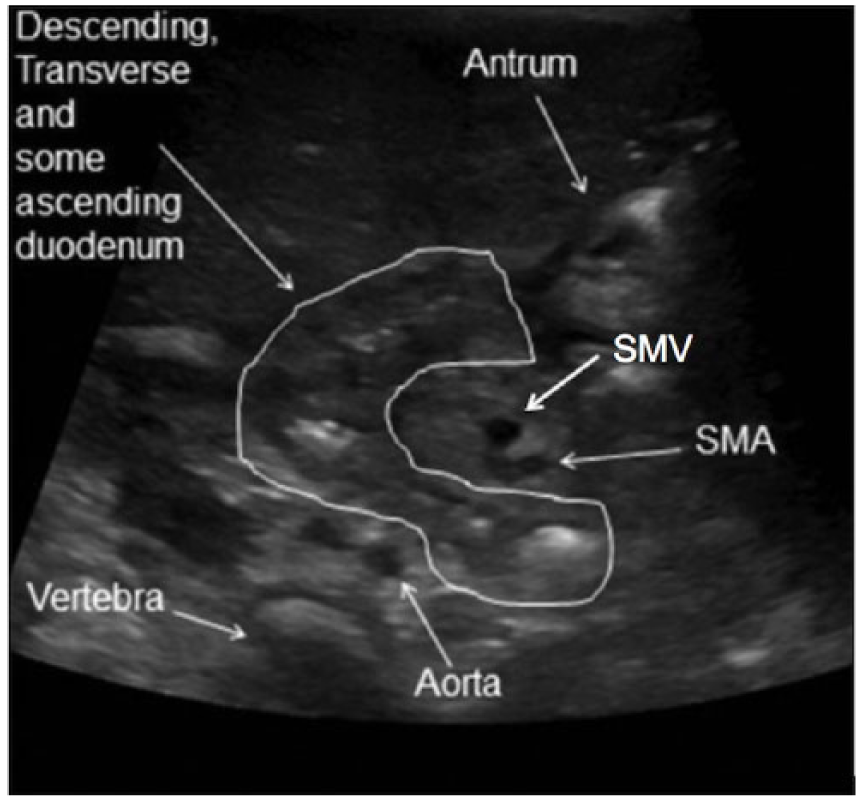
Transverse ultrasound image of the normal relationship of the superior mesenteric artery (SMA) and superior mesenteric vein (SMV). Source: Journal of Clinical Imaging Science, http://www.clinicalimagingscience.org/article.asp?issn=2156-7514;year=2011;volume=1;issue=1;spage=19;epage=19;aulast=Herliczek.
The gold standard for diagnosis of malrotation with volvulus is a fluoroscopic UGI contrast study, and sonography is not typically recommended for diagnosis. However, to minimize the exposure of pediatric patients to ionizing radiation and contrast, sonography may be used as a first-line imaging modality for diagnosis. If a reversed SMA/SMV relationship is noted sonographically, a UGI series is performed as the next step in the patient’s care. A UGI series does not typically evaluate the relationship of the SMA and SMV, but the alimentary tract itself is assessed. In a normal digestive tract, the ingested contrast is visualized throughout the length of the tract. However, in a patient with midgut malrotation and volvulus, the contrast halts at the level of the obstruction and does not continue any farther. As this examination evaluates the digestive tract itself, it is the diagnostic imaging modality of choice for midgut malrotation and volvulus.
As stated earlier, the patient was referred to the sonography department with suspicion of pyloric stenosis. As pyloric stenosis is common in newborns, it is a likely differential diagnosis for a neonate experiencing vomiting. Additionally, neonatal appendicitis should not be ruled out, as this diagnosis presents with vomiting, fever, and abdominal distention, 10 similar to midgut volvulus. Intussusception should also be considered when the neonate presents with symptoms of intestinal obstruction. Although rare in neonates—with small bowel intussusception being more common in this age than large bowel—intussusception is most associated with demise of the bowel. 11
Conclusion
Midgut malrotation is fairly common, and most patients remain asymptomatic throughout their entire lives. Midgut volvulus secondary to malrotation is uncommon and primarily treated with the Ladd procedure. Evidence has shown the effectiveness of the laparoscopic Ladd procedure in reducing length of stay and complications from surgery. This case demonstrates that sonographic visualization of an opposite SMA/SMV relationship, combined with the patient’s primary symptom of bilious vomiting, can play an important role in diagnosis of midgut malrotation with volvulus. A quicker diagnosis leads to prompt surgical intervention and better outcomes for patients with such anomalies.
Footnotes
Acknowledgements
We thank Kayci Mount, RDMS, RVT, Patricia Jackson, RDMS, RVT, Lindsey Tegeler, RDMS, RVT, and Rachelle David, RDMS, RVT, for their assistance and guidance in obtaining information and images for this case study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.