
Abstract
Intestinal malrotation is a rare fetal anomaly resulting from the failure of midgut rotation and fixation. Sonography is typically the first modality of choice for assessing pediatric pathology due to its high sensitivity, portability, real-time imaging capability, and non-ionizing technique; however, its role in diagnosing small bowel rotational anomalies remains limited and controversial. Fluoroscopic upper gastrointestinal imaging (UGI) is the primary diagnostic examination at most institutions. However, even on UGI, imaging findings may be equivocal. In such cases, sonography may provide additional information at facilities where it is not used as a primary diagnostic tool. This case report represents the first reported case showing how patient position is important as the typical vascular sonographic features of rotation were normal in one position but abnormal in another. In addition, this case shows how congenital intestinal malrotation was decisively diagnosed using sonographic imaging.
Keywords
There are a wide variety of congenital anomalies that can result in gastrointestinal tract obstruction in newborn infants and older children. Some of these include malrotation, annular pancreas, atresia and stenosis, duplication cysts, meconium ileus, meconium plug syndrome, Hirschsprung’s disease, neonatal small left colon syndrome, neoplasia, and trauma. 1 Congenital duodenal obstruction occurs in half of congenital bowel obstructions.2,3 The prevalence is 1 in 5000 to 1 in 10 000 live births.4,5 Overall, the survival rate is 90%–95% as operative technique and neonatal intensive care units (NICU) improve, while death is typically consequent to a complex congenital heart disease.3,6–9
Bowel obstruction due to malrotation or bowel atresia appears in about 6 per 10 000 live infant births. 10 Malrotation is a congenital anomaly involving the abnormally positioned intestines during fetal development. This may lead to midgut volvulus around a narrow mesenteric root, which is a surgical emergency. Intestinal malrotation is observed in about 1 in 2500 live infant births less than 1 year of age, occurring in 0.2%–1% of the normal population. 10 The following case report describes the use of sonography as a diagnostic problem solver following an equivocal upper gastrointestinal imaging (UGI) examination. Importantly, this case highlights that one of the key sonographic signs of malrotation, that is, the superior mesenteric artery (SMA)/superior mesenteric vein (SMV) relationship, is positionally dependent, that is, normal in one patient position and abnormal in another. To the best of the authors’ knowledge, this has not previously been reported. Familiarity of this positional dependency is imperative to help the sonographer and interpreting radiologist to correctly identify malrotation.
Case Report
A newborn female infant was delivered via elective cesarean surgery at 39 6/7 weeks of gestation. The mother’s pregnancy was complicated by advanced maternal age, but otherwise a healthy infant was delivered. There are no known familial genetic predispositions. Apgar scores were 9 and 9 at 1 and 5 minutes, respectively. Around 40 hours-of-life, the infant developed an episode of bilious emesis, but had regular stools. The patient’s abdomen was slightly distended but remained soft, and the infant appeared in no distress. The medical care team ordered an urgent UGI radiographic examination to assess for volvulus or obstruction (Figure 1). An UGI is a radiographic examination in which the esophagus, stomach, and duodenum are evaluated using a fluoroscopy technique. The study provides a continuous radiographic image of moving anatomic structures and ingested contrast.
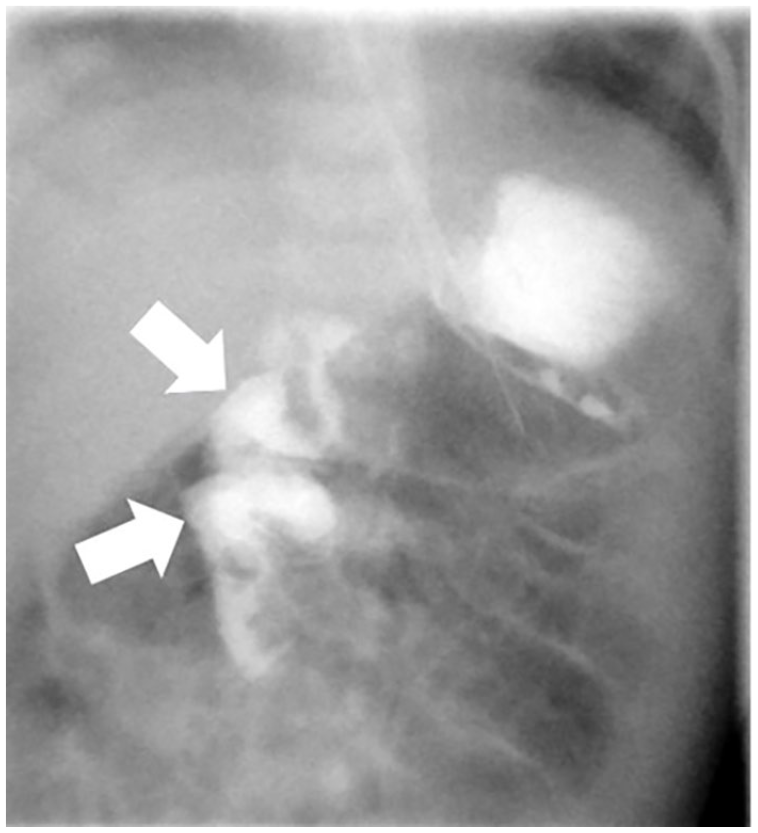
Fluoroscopic upper GI examination demonstrated the abnormal course of the duodenum (arrows), which was highly suggestive of malrotation without obstruction. GI, gastrointestinal imaging.
A 5-Fr feeding tube was advanced through the patient’s left nostril under fluoroscopic guidance into the stomach. A small volume of water-soluble contrast was injected through the tube and into the stomach. The contrast rapidly filled the non-dilated proximal duodenum and entered the bowel loops to the right of the spine with a slightly circular pattern. Eventually, the contrast passed to the left of the spine and up to the level of the duodenal bulb. The normal C-shaped duodenum could not be demonstrated despite multiple attempts including the repositioning of patient and an additional contrast injection (Figure 1). At the conclusion of the UGI, it was felt that the patient was likely malrotated. However, given that the distal duodenum was eventually visualized in a normal position, there was a small possibility that the patient could have a markedly redundant duodenum with normal rotation. As the patient was in no apparent distress, the radiologist recommended a sonographic examination to be performed to evaluate the relationship between SMA and SMV. Notably, at this institution, sonography is not primarily used to evaluate for malrotation, a practice that remains controversial in the pediatric radiology literature, limited to a few pediatric hospitals in North America.
The medical care team ordered an emergent sonogram. Protocol imaging at this institution includes scanning neonates and young children with a high-frequency linear-array transducer, while a low-frequency curvilinear transducer may be used for older children. Fasting for this particular examination is not required, and there are no time constraints after UGI. Fluid is not given to the patient as this institution does not evaluate the course of the duodenal sweep, although some evidence supports this expansion of sonography for malrotation diagnosis in the future. The ideal sonographer scanning technique includes the following:
Begin scanning in the supine position with the transducer midline on the abdomen;
Identify the aorta;
Obtain a gray-scale cine clip of the superior mesenteric vessels from the main portal vein and aorta through the entire course of the SMA/SMV;
Obtain color Doppler images of the SMA/SMV relationship at the origin and at a point halfway between the origin and distal;
If a swirling/“whirlpool” sign is observed, document with color Doppler images and cine clips;
Roll the patient in an oblique lateral position and reimage steps 2–5.
Gray-scale and color Doppler sonography (LOGIQ E9; GE Healthcare) using a 9-MHz linear-array transducer initially demonstrated a normal SMA–SMV orientation when the patient was lying in a left oblique position. The sonographer elected to begin in the oblique position as the infant was comfortably resting in that state. The SMA was visualized posterior and to the left of the SMV (Figure 2). Once the patient was repositioned and laid supine, the SMA–SMV position inverted, consistent with classic vascular findings of intestinal malrotation diagnosis. The SMV was visualized anterior and to the left of the SMA (Figures 3 and 4). The SMV and SMA remained patent throughout the examination with normal-appearing spectral Doppler waveforms (Figures 5 and 6).
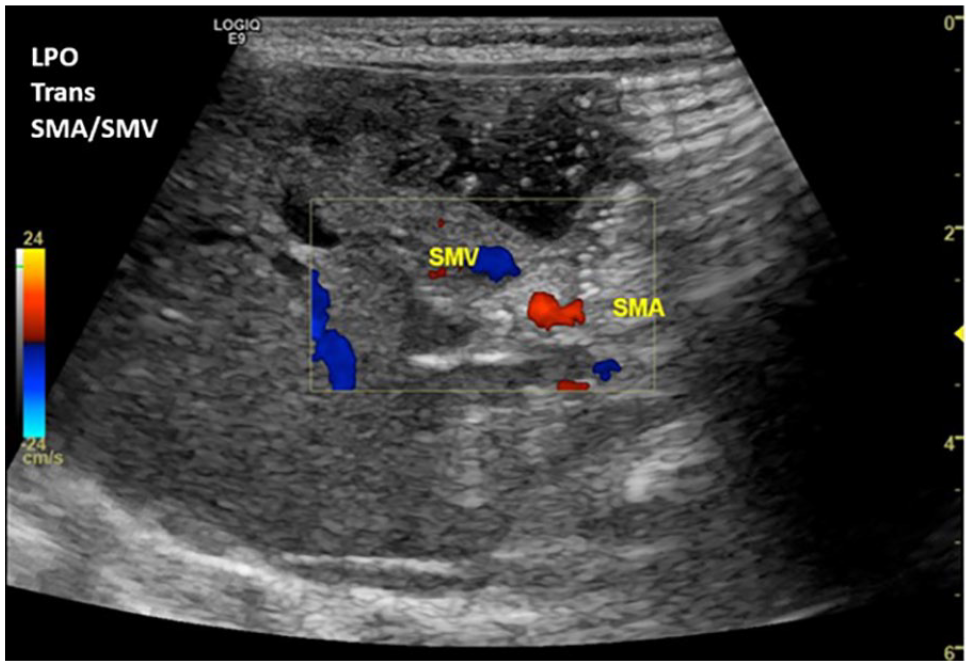
Transverse color Doppler sonographic image of the SMA and SMV demonstrated a normal anatomic relationship while the patient was in the left oblique position. The SMA was visualized posterior and to the left of the SMV. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
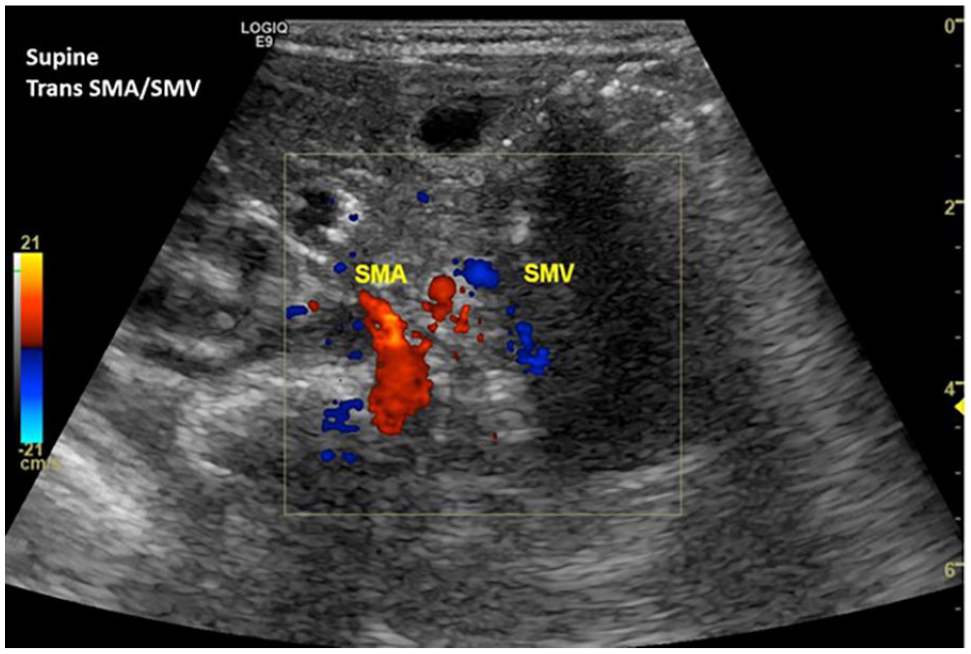
Transverse color Doppler sonographic image of the SMA and SMV confirmed an abnormal anatomic relationship once the patient was repositioned supine. The SMV was visualized anterior and to the left of the SMA. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
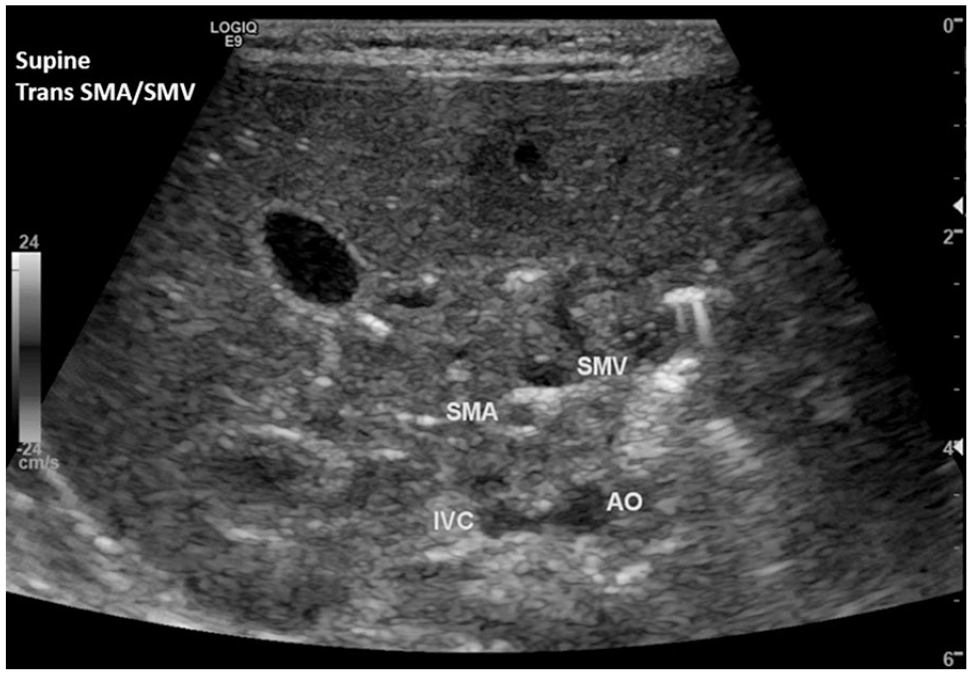
Transverse gray-scale sonographic image of the SMA and SMV confirmed an abnormal anatomic relationship once the patient was repositioned supine. The SMV was visualized anterior and to the left of the SMA. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
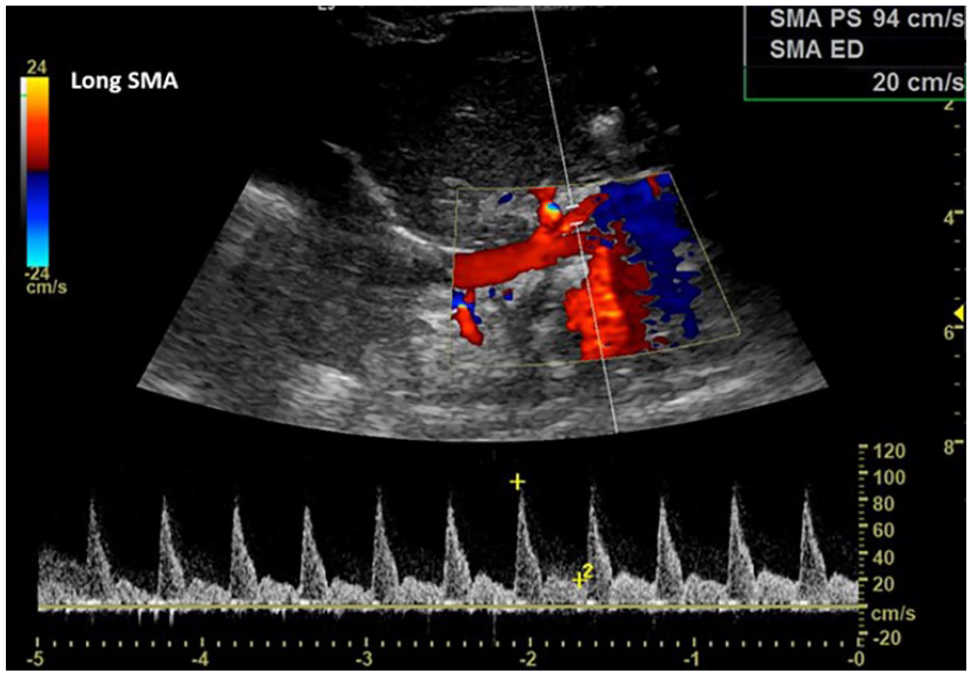
Longitudinal color and spectral Doppler imaging revealed a patent and normal-appearing SMA waveform and velocities. SMA, superior mesenteric artery.
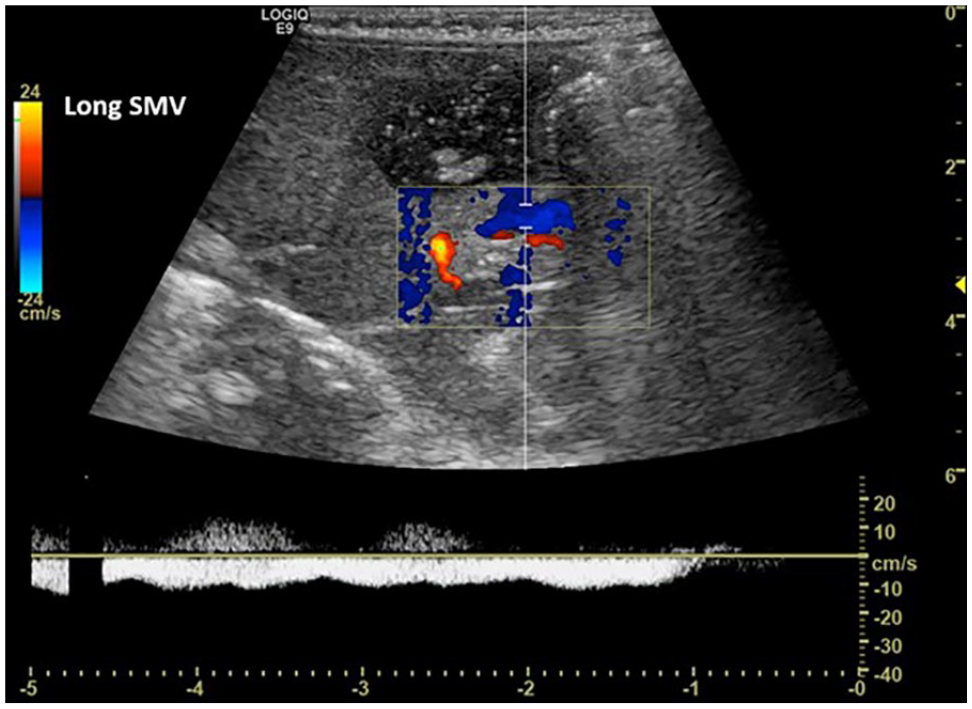
Longitudinal color and spectral Doppler imaging revealed a patent and normal-appearing SMV waveform. SMV, superior mesenteric vein.
The infant was transferred to the NICU that evening and remained clinically stable. A laparoscopic Ladd’s procedure was scheduled for the following morning. Ladd’s bands are thick, fibrous stalks of peritoneal tissue which connect the cecum to the retroperitoneum in the right lower quadrant (RLQ) of the abdomen. When obstructive Ladd’s bands are present, extrinsic compression to the duodenum occurs with the abnormal location of the cecum in the right upper quadrant of the abdomen. The patient was brought into the operating room to explore the abdomen following general anesthesia induction and intubation. Ladd’s bands were noted across the duodenum, with a corkscrew-type appearance, all small bowel on the right and meconium-filled colon on the left. The Ladd’s bands were divided, the duodenum straightened, and the mesentery broadened (Figure 7). The small bowel was reduced into the right side of the abdomen. Due to the appendix in an abnormal position, midline of the left lower quadrant, it was necessary to perform an appendectomy eliminating any future diagnostic dilemma. The case was substantially more difficult than usual due to the patient’s size being less than 4 kg. The patient tolerated the procedure well, was extubated, and then taken to the recovery unit in satisfactory condition. During the sixth month well-child visit, the patient was developing healthy as expected and has not experienced any medical-related complications.
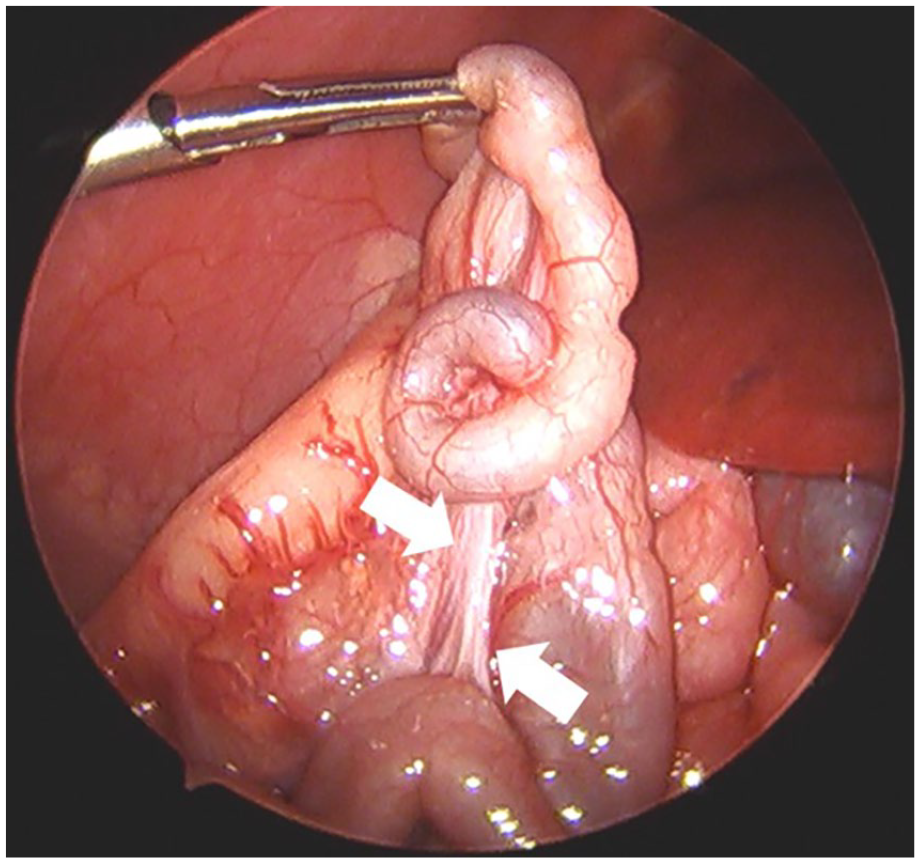
Laparoscopic imaging demonstrated a foreshortened mesenteric pedicle (arrows).
Discussion
Intestinal malrotation is the abnormal rotation of the duodenum and/or cecum around the SMA axis with fixation of the midgut and hindgut to the retroperitoneum.11–14 Normal intestinal rotation can be described as herniation of the bowel into the umbilical cord in the fourth gestational week with a 90° counterclockwise rotation. As the midgut returns to the peritoneal cavity during the 8th-12th week, it further rotates 180°, completing 270° total counterclockwise rotation around the SMA.10,15,16 The small bowel is fixed into place with the duodenum in the retroperitoneum and the jejunum and ileum extending along a broad-based mesentery from the left upper quadrant (LUQ) to the RLQ and the cecum in the right iliac fossa.10,15,17 Failure of the normal 270° rotation during development results in malrotation and a foreshortened mesenteric pedicle. This foreshortening of the pedicle makes the upper small bowel susceptible to a midgut volvulus where the intestines wrap around the SMA/SMV vascular pedicle, obstructing the lymphatic drainage and arterial and venous blood flow, resulting in massive bowel infarction, short bowel syndrome, and potential death11,12,14,16 (Figures 8–10). The mortality rate of midgut volvulus has been reported at 3% 18 with approximately 15% demonstrating bowel strangulation found intraoperatively. 19
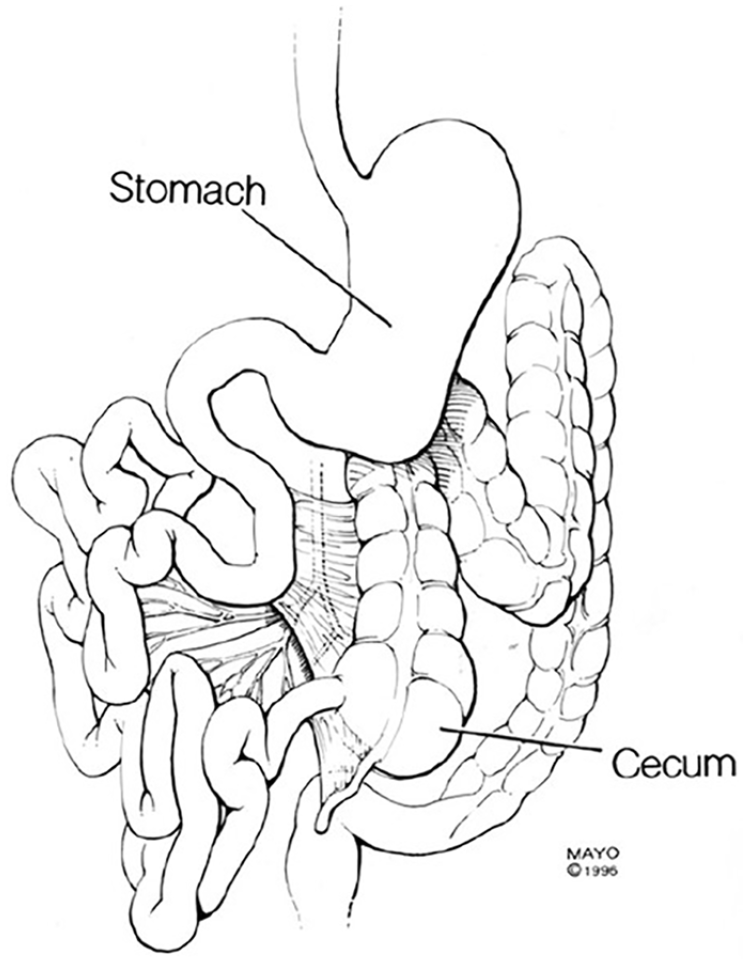
Congenital midgut malrotation.
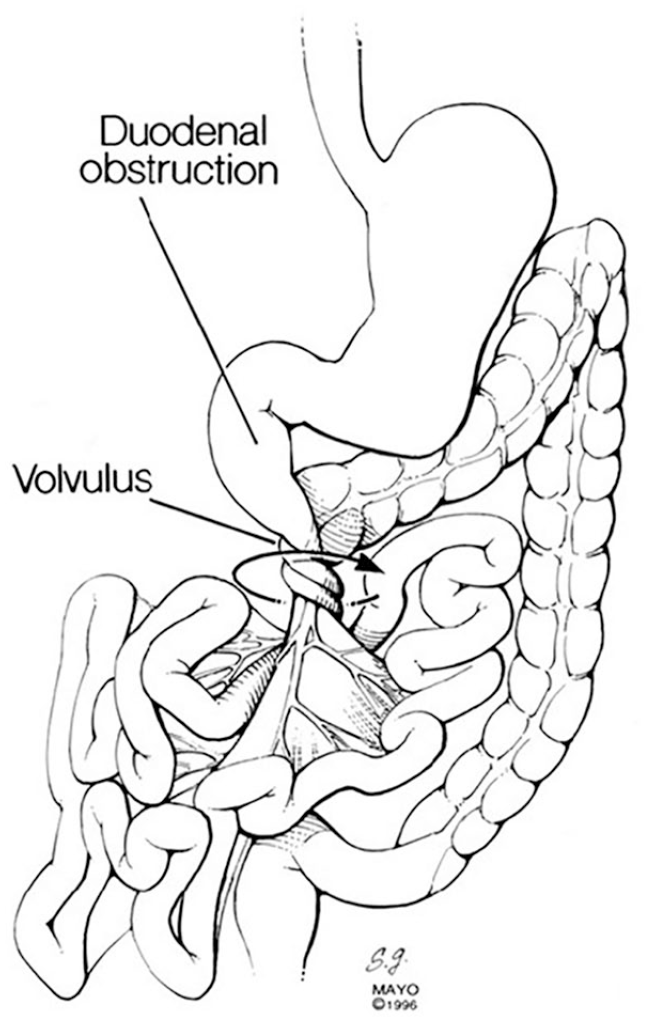
Spontaneous volvulus around the narrow mesenteric root of the SMA and SMV. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
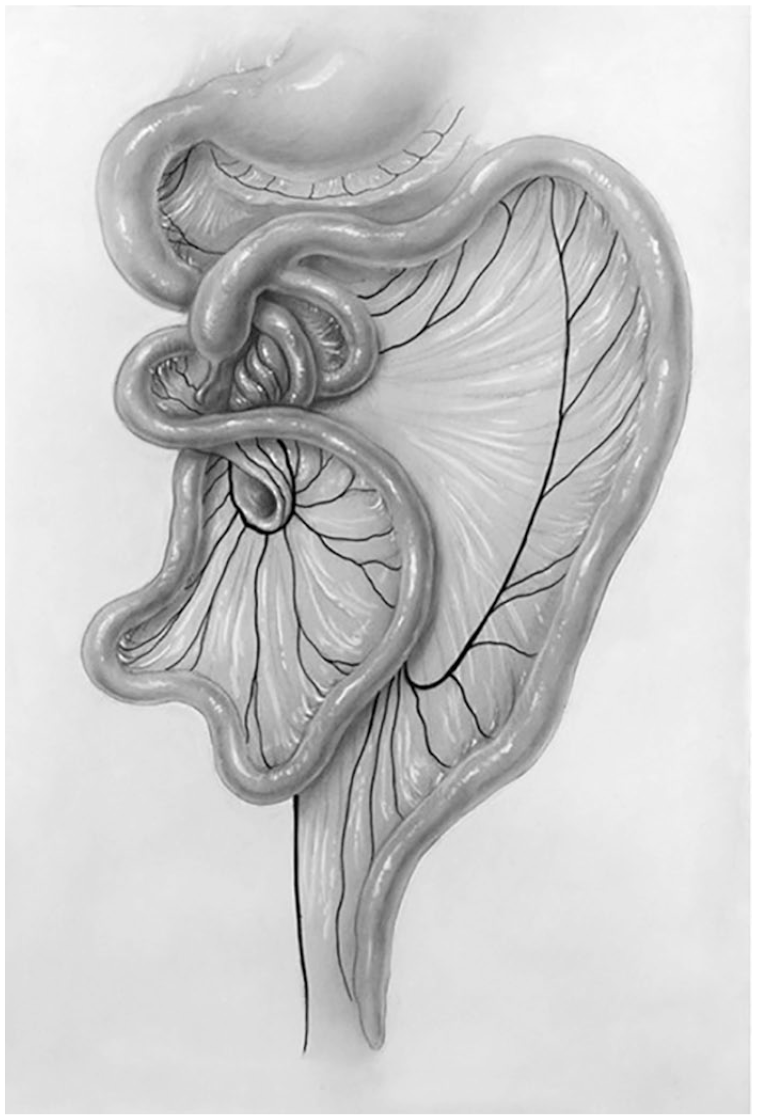
The diagram exemplifies spontaneous volvulus around the narrow mesenteric root of the SMA and SMV. Note the abnormal cecal and appendiceal location in the left upper quadrant. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
The typical presentations of intestinal obstruction are bilious vomiting, constipation, and abdominal distension. 20 In greater than 50% of cases, the most common symptom is bilious emesis during the first month of life, with rectal bleeding and abdominal distension occurring late in the process. 10 In infants, it has been reported that there is a higher incidence of associated anomalies with malrotation. Cardiac anomalies, anorectal malformation, duodenal web, and trisomy 21 have been common associations, as well as type IIIb small bowel atresia that may be secondary to antenatal volvulus. 10
The diagnosis of malrotation is typically confirmed by performing an UGI examination. The positions of the duodenum, jejunum, and small bowel can be established. The key hallmark finding of malrotation on UGI is the lack of retroperitoneal course with abnormal position of the duodenojejunal junction. A complete obstruction may have a bird-beak appearance if volvulus is present at the proximal to mid-duodenum level. 10 The small intestine may be visualized as a corkscrew appearance as it twists around the SMA. 21 Torres and Ziegler 22 described barium UGI contrast examinations as the preferred diagnostic study of choice for malrotation diagnosis, being 95% sensitive and accurate in 86% of cases. Although not widely accepted, sonography has been reported as a useful diagnostic tool and an alternative to UGI examination for malrotation.23,24 Some debate remains regarding the accuracy and appropriateness of color Doppler sonographic imaging when evaluating malrotation and midgut volvulus. The “whirlpool” sign of midgut volvulus was described by Pracros et al, 25 in which the SMV and mesentery wrap around the SMA in a clockwise fashion and it can be demonstrated using color Doppler.26,27 This “whirlpool” sign can be visualized with a reported 97% positive predictive value. 28 The abnormal relationship between the SMA and SMV can be indicative of malrotation when evaluating these mesenteric vessels using color Doppler. In normal anatomy, the SMA lies posterior and to the left of the SMV. 18 Reversal of the SMA and SMV position is most predictive of malrotation, with the SMV to the left of the SMA. 27 However, as this case demonstrates, the normal or abnormal relationship of the SMA to the SMV is positionally dependent. Thus, when evaluating this relationship, the patient should be evaluated in a variety of positions, as in this case left oblique and supine.
Immediate surgical treatment is required for malrotation diagnosis with or without a midgut volvulus in a patient with bilious emesis. 16 The bowel is detorsed in a counterclockwise fashion immediately when a volvulus is present, and any non-viable intestine is resected. William Ladd described the Ladd’s procedure in 1936, which is widely used today. 29 The Ladd’s bands are separated, the base of the mesentery is broadened, and to minimize the risk of recurrent volvulus, the small intestine is placed in the right side of the abdomen and the colon in the left. The cecum is positioned in the LUQ of the abdomen and an appendectomy is performed to reduce any future diagnostic confusion.10,15,16,30,31 The typical practice is to perform surgical management via laparotomy, but several studies have shown to have successful outcomes using laparoscopic technique.32–34 An elective Ladd’s procedure is widely performed in patients without any comorbidity.35–38 Complications of Ladd’s surgical procedure include small bowel obstruction, incisional hernia, perforated viscus, and recurrent volvulus. 10 The most common surgical complication is small bowel obstruction, which occurs in 7%–24% of open laparotomy procedures and 0%–5% of those performed laparoscopically.39–43 Overall mortality is roughly 3% depending on the presence of bowel ischemia. 44
Conclusion
Sonography remains a cost-effective, accessible, non-nephrotoxic, and non-ionizing tool for diagnosis in the pediatric population and is the initial imaging modality of choice for many disease processes. Diagnosing congenital intestinal malrotation is an emergent finding especially when midgut volvulus is suspected. An UGI radiographic examination is considered the diagnostic gold standard. However, some institutions perform sonography primarily for malrotation. Furthermore, color Doppler can be used as a problem-solving tool when the UGI is equivocal, with assessment of the orientation of the SMA and SMV helping to aid in diagnosis. The key finding is the reversal of the mesenteric vessels with the SMV to the left of the SMA. However, as this case shows, the relationship should be scrutinized in a variety of positions.
Footnotes
Authors’ Note
The patient’s family gave permission for the use of medical history and imaging for research purposes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.