
Abstract
Granulomatous mastitis (GM) is a rare and benign condition of the breast. The condition most commonly affects women of childbearing age and is commonly associated with pregnancy, breastfeeding, and oral contraceptive use. The symptoms and imaging characteristics of GM often mimic those of breast carcinomas. Imaging findings tend to be less pronounced by mammography, and GM can be mammographically occult, making sonography important in identifying the condition. Proper identification of this entity is important to prevent misdiagnosis and/or delayed treatment. The diagnosis is commonly made by tissue sampling under ultrasound guidance.
Granulomatous mastitis (GM; also known as granulomatous lobular mastitis or granulomatous lobulitis) is a rare and benign condition of the breast. GM was initially described by Kessler and Wolloch 1 in 1972 as a condition unassociated with trauma or infection. The etiology of GM is unknown, although an autoimmune component is suspected.2,3 It typically affects women of childbearing age and is commonly associated with pregnancy, breastfeeding, and oral contraceptive use. 4 The symptoms of GM tend to overlap with more malicious entities, particularly breast carcinoma. However, it may also be asymptomatic. The imaging characteristics of GM are variable and likewise tend to overlap with those of breast carcinoma. GM can be occult by mammography, but the entity is rarely occult as detected on sonography. 5 The sonographic findings are varied but can be suggestive of the entity. GM is commonly diagnosed by tissue sampling under ultrasound guidance. Proper identification and diagnosis of GM is important to prevent misdiagnosis and/or delayed treatment. Treatment protocols and treatment efficacies vary, and the condition is often chronic.
Case Report
A 35-year-old woman presented to her primary care physician reporting an area of palpable concern, pain, and redness of the skin in the upper inner right breast adjacent to the areola. The patient reported first noting the area of concern 15 days prior with gradual worsening of the symptoms. The patient denied other breast concerns, including nipple discharge. The patient reported no systemic symptoms, including fevers, fatigue, and cough. The patient had no significant personal breast health history and no significant family history of breast cancer. The patient was otherwise healthy without any significant current health conditions and did not take any prescription medications, including oral contraceptives. The patient was tested the year prior for HIV-1/HIV-2 and was negative. The patient has had two pregnancies, with one full-term delivery via spontaneous vaginal delivery six years prior. She had an intrauterine device placed shortly after the delivery. A urine pregnancy test was administered upon her presentation and was negative for pregnancy. At presentation, the patient’s vital signs were normal, including a temperature of 99.2°F. Physical examination was significant for a 4-cm palpable mass in the right breast at 2 o’clock adjacent to the areola with overlying skin erythema. No dermal pustules or drainage were noted.
A presumptive diagnosis of acute mastitis was made. The patient was prescribed a course of oral antibiotics. A diagnostic mammogram and breast sonogram were ordered and scheduled for two weeks from the date of presentation.
The patient reported to the breast imaging clinic two weeks later. She reported completing the course of antibiotics without improvement of her symptoms. Physical examination findings were unchanged. A bilateral diagnostic mammogram was performed using both 2D and 3D (tomosynthesis) imaging (Figure 1). Mammography demonstrated a 5-cm focal asymmetry in the right breast centered at 2 o’clock middle depth, corresponding with the area of concern. There was associated mild overlying skin thickening and nipple-areolar retraction. In addition, there was subtle right axillary lymphadenopathy as demonstrated by the presence of lymph nodes with the loss of the normal fatty hila and reniform shapes. The left breast and axilla were unremarkable.
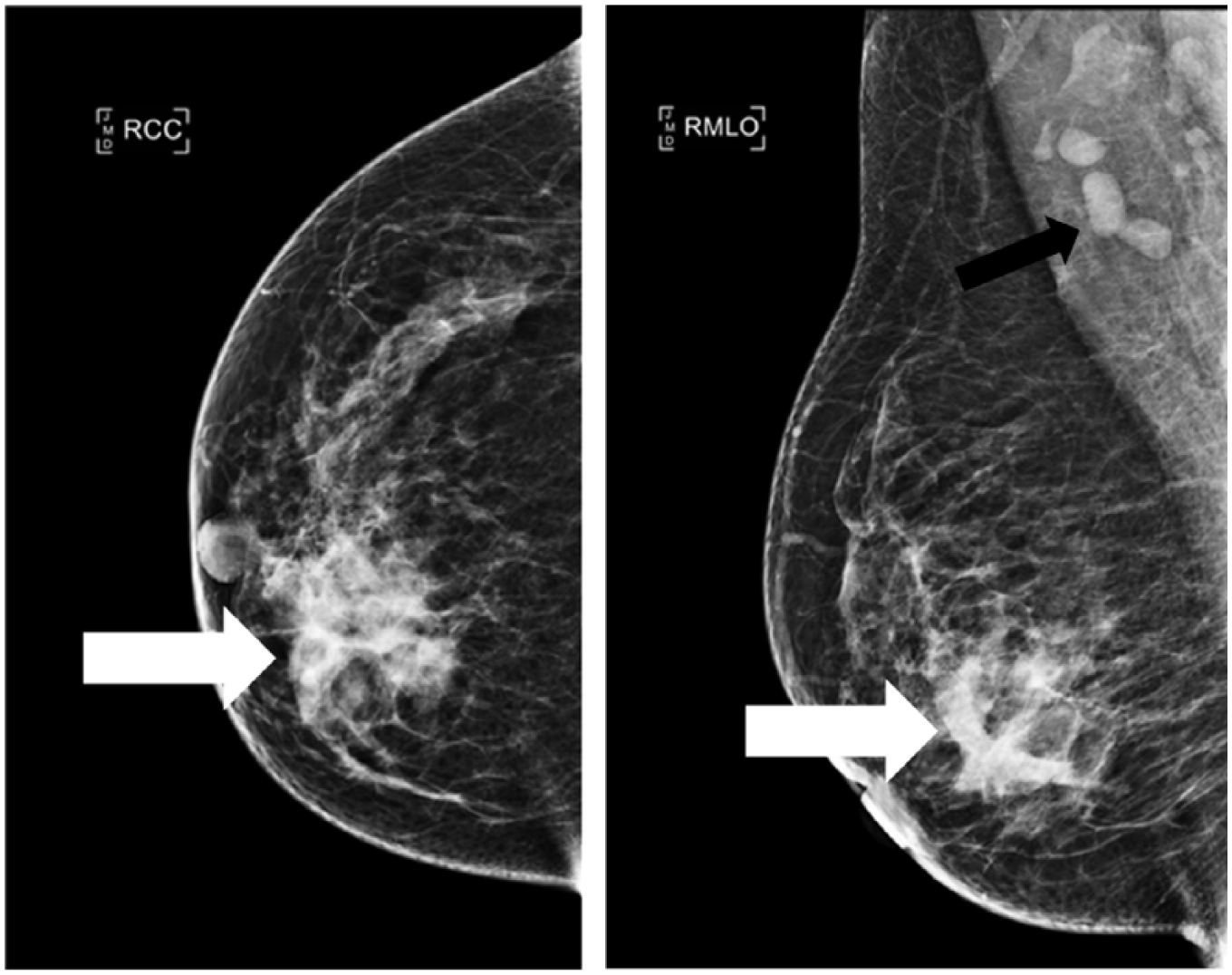
Craniocaudal and mediolateral oblique 2D mammography views of the right breast show a 5-cm focal asymmetry in the right breast centered at 2 o’clock middle depth (white arrows). Right axillary lymphadenopathy is also noted (black arrow). There is mild skin thickening and nipple-areolar retraction.
The mammogram was immediately followed by a focused sonogram of the area of concern in the right breast and axilla (Figure 2). Sonography demonstrated a 6.8-cm × 2.6-cm × 5.3-cm heterogeneously echogenic irregular-shaped mass in the right breast centered at 2 o’clock 5 cm from the nipple. The margins were predominately indistinct. Areas of tubular echogenicity extended to the superficial breast, and there was mild overlying skin thickening. Color Doppler sonography demonstrated predominately perilesional hypervascularity with less prominent intralesional hypervascularity. Sonographic evaluation of the right axilla demonstrated multiple lymph nodes with mild cortical thickening measuring up to 0.5 cm. There was partial effacement of the fatty hila. No cortical hypervascularity was noted by color Doppler imaging. Mammography and sonographic findings correlated with the area of concern in the right breast.
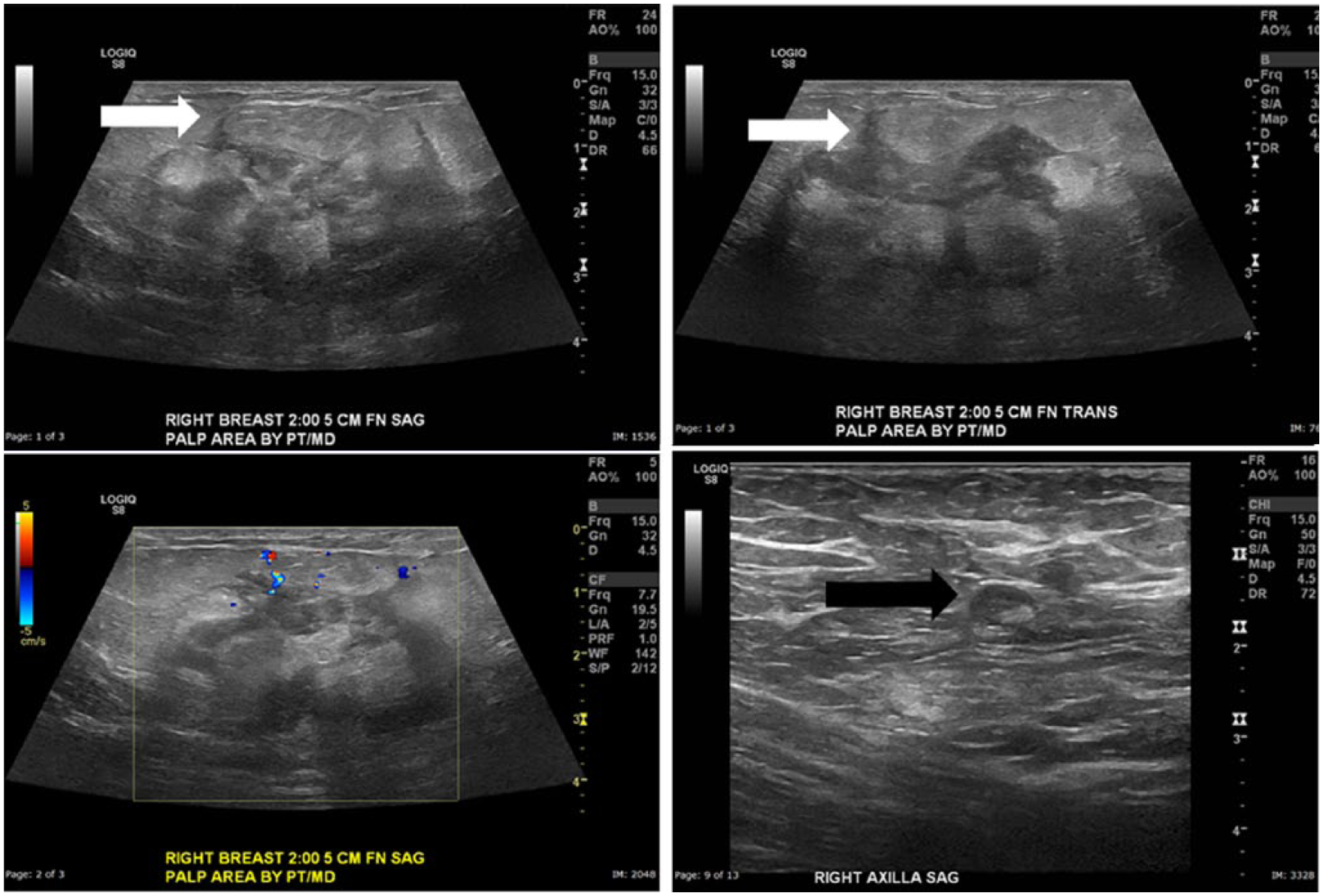
Grayscale sonography of the right breast at 2 o’clock 5 cm from the nipple shows a 6.8-cm × 2.6-cm × 5.3-cm heterogeneously echogenic irregular-shaped mass with predominately indistinct margins. Areas of tubular hypoechogenicity extend to the superficial breast (white arrows), and there is mild overlying skin thickening. Color Doppler imaging demonstrates predominately perilesional hypervascularity with less prominent intralesional hypervascularity. Grayscale evaluation of the right axilla demonstrates a lymph node with mild cortical thickening measuring up to 0.5 cm with partial effacement of the fatty hilum (black arrow).
Given the clinical presentation and imaging findings, GM was suspected. However, given the overlap of symptoms and imaging findings with breast carcinoma and the need for pathologic confirmation of the suspected etiology, an ultrasound-guided core needle biopsy of the mass was recommended for tissue diagnosis.
The ultrasound-guided core needle biopsy was performed four days later (Figure 3). Using a 14-gauge core biopsy needle device under ultrasound guidance, four specimens were taken of various areas of the lesion. A ribbon-shaped biopsy marker was deployed. Postprocedure mammogram demonstrated the biopsy marker within the lesion. The specimens were sent for histopathologic evaluation.
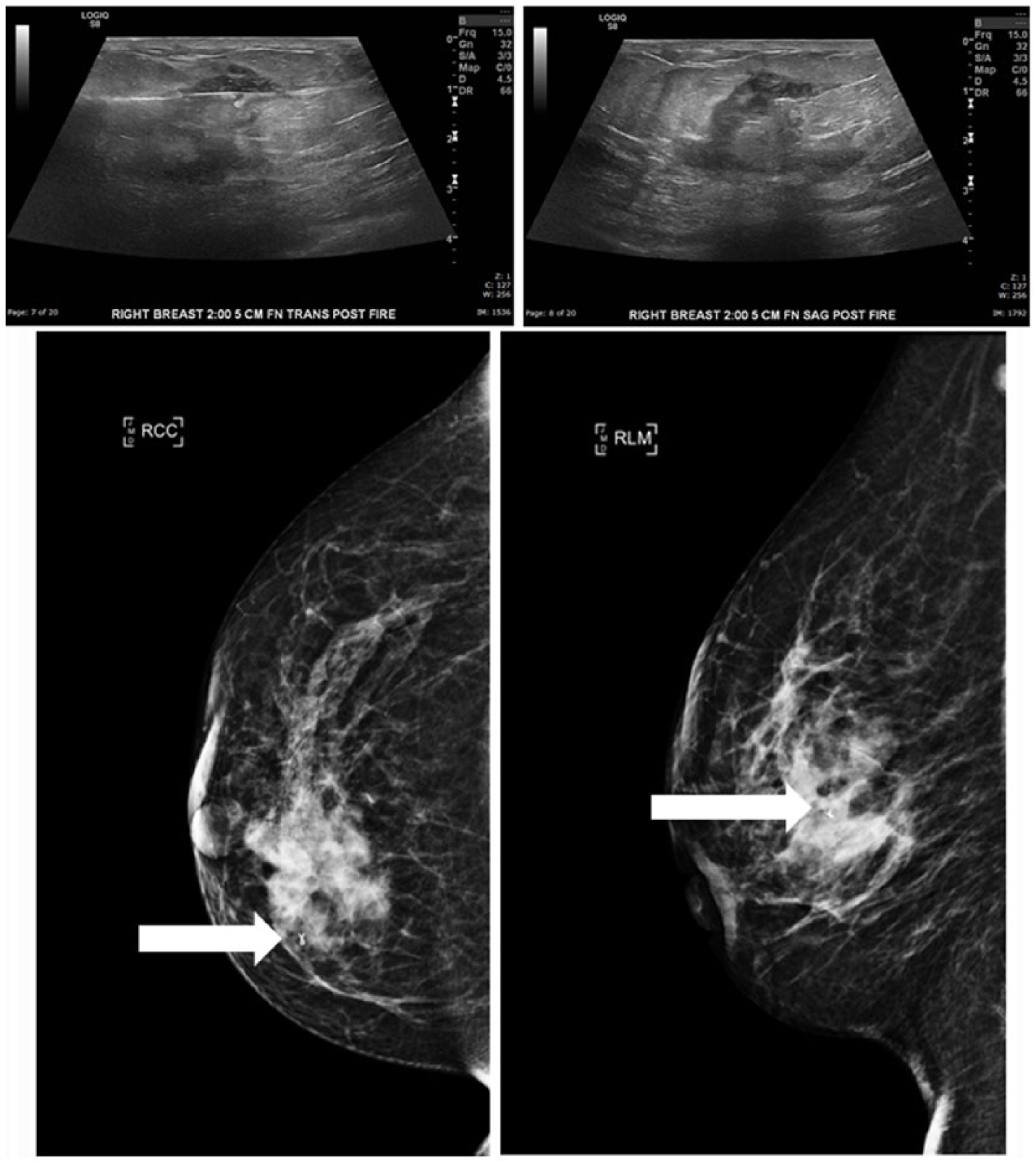
Grayscale sonographic images of the ultrasound-guided core needle biopsy demonstrate the biopsy needle well within the mass and confirmed in the tangential plane. Craniocaudal and lateromedial mammography views performed immediately following the procedure demonstrate the ribbon-shaped biopsy marker to be within the targeted lesion (arrows).
Histopathologic evaluation demonstrated dense chronic inflammatory cell infiltrate surrounding breast lobules and several granulomas with focal central necrosis and acute inflammation (Figure 4). Acid-fast bacilli (AFB) and Grocott-Gomori methenamine silver (GMS) special stains were negative for acid-fast bacilli and fungal organisms. No malignancy was identified. The pathologic diagnosis was granulomatous mastitis.
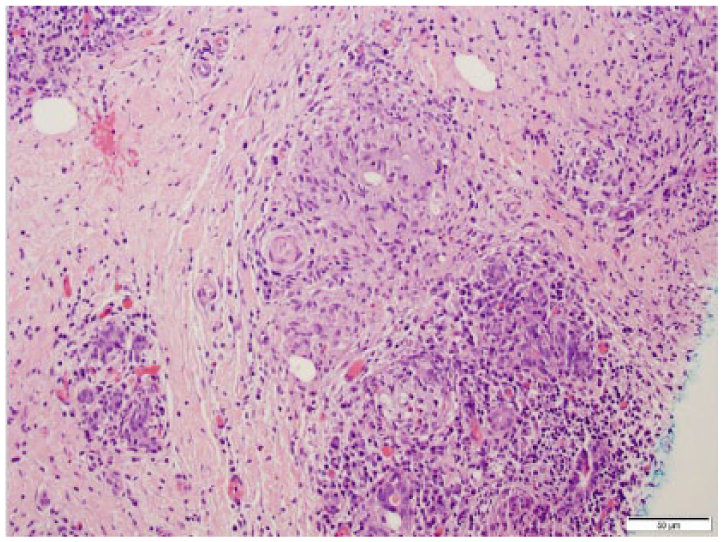
Hematoxylin and eosin stain shows dense chronic inflammatory cell infiltrate surrounding breast lobules and several granulomas with focal central necrosis and acute inflammation. (Image provided by Dr. Sagar Dhamne, Department of Pathology, Baylor College of Medicine)
Given the diagnosis, the patient was placed on a 30-day regimen of oral prednisone (corticosteroid). Subsequent clinical follow-up over two months has demonstrated near-complete resolution of the symptoms and physical examination findings. No repeat imaging has been performed. Of note, the Quantiferon Gold test was performed and was negative. The patient also had a negative two-view chest radiograph. There were no laboratory or clinical findings to suggest tuberculosis or sarcoidosis as the underlying cause.
Discussion
The normal breast is primarily composed of glandular tissue and fat (Figure 5). The amount of glandular tissue within the breast varies and is analogous to breast density noted by mammography. Fibroglandular tissues are more prominent in the upper outer quadrant and less prominent in the lower inner quadrant. Therefore, both malignancy and benign breast pathologies are more commonly located in the upper outer quadrant.
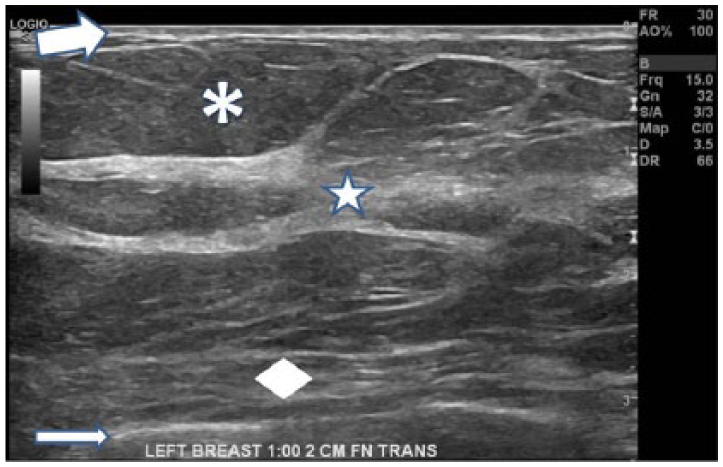
Grayscale sonographic image of a normal breast. Normal gray appearance of the subdermal fat (asterisk). Hyperechoic, white appearance of fibroglandular tissue (star). Thin hyperechoic dermis (thick arrow). The pectoralis muscle (diamond) and an underlying rib are identified (thin arrow). Note the image label including laterality, clock face position, and distance from the nipple in centimeters.
Breast sonography requires the use of a high-frequency linear transducer (8–15 MHz). However, lower frequency transducers may be needed for larger breasts or highly attenuating lesions. The patient is placed in the supine position with the ipsilateral arm raised over her head. Sonographic settings should be optimized so that the subcutaneous fat appears gray in comparison to the echogenic fibroglandular tissue, which appears white. The proper-appearing subcutaneous fat is used as a reference for echogenicity within the breast, with lesions of similar echogenicity being described as isoechoic.
Breast abnormalities are imaged in tangential planes, either radial and antiradial or transverse and sagittal. Imaging should include the size of the abnormality in three dimensions via grayscale imaging and document vascularity via color Doppler imaging. The images should be labeled with which breast laterality, clock-face location, and distance from the nipple in centimeters. 6
The histology of GM demonstrates noncaseating granulomas mixed with epithelioid histiocytes and multinucleated giant cells of the foreign body and of the Langerhans types confined to breast lobules. 2 GM has a mean age of presentation of 33 to 38 years and represents 1.8% of benign breast diseases.2–5 The condition is rare with an unknown, albeit very low, prevalence. The cause is unknown, although an autoimmune etiology is favored. Association with pregnancy, breastfeeding, and oral contraceptive use is noted. GM typically develops within six years following pregnancy.2–5 There is a higher predilection for women of Latin and Asian races. 7 The condition is exceedingly rare in men. 8
Granulomatous mastitis has similar clinical signs and symptoms to breast carcinoma. GM commonly presents as an area of palpable concern in 78% to 89% of cases. Pain and tenderness are reported in 11% to 41% of cases. Erythema, skin thickening, dermal sinus formation, and/or axillary lymphadenopathy are less common presentations.2–5,8,9 Systemic symptoms such as fever, chills, and fatigue are unusual. GM typically is unilateral without side or location predilection, but the subareolar breast tends to be spared.2–5,7 GM is often a diagnosis of exclusion, with associated laboratory tests performed to rule out other causalities. Biopsy specimens will commonly be subjected to AFB and GMS stains to evaluate for tuberculosis (TB) or fungal infections. The patient will also commonly undergo chest radiograph and a Quantiferon Gold test to further evaluate for TB. The chest radiograph will also be used to evaluate for potential sarcoidosis, and further autoimmune serum tests may be performed if indicated.
Treatment of GM varies without an optimal management regimen firmly established. Given that the symptoms can overlap those of infectious mastitis, patients are often empirically treated with antibiotics, although the efficacy rate may be as low as 5%.10–12 Commonly, GM will be treated with corticosteroids, although there is no consensus regarding the dose and duration of treatment. Surgical excision, often with wide surgical margins, is also commonly used, particularly for refractory or severe cases.10–13 Refractory cases may also be treated with other medications such as methotrexate, azathioprine, and/or hydroxychloroquine. 14 Despite the varied treatment options, GM can often be refractory or recurrent. For instance, recurrence rates for surgical excision have been reported to range from 8% to 50%.10–13 There is no defined disease progression or staging, with significant varied treatments and outcomes. GM is typically managed clinically following diagnosis based on symptoms and clinical findings. Sonography can be used to serially gauge for size changes of the lesion, although no study has been performed to determine the efficacy of using sonography to follow the disease.
Mammography imaging findings of granulomatous mastitis are variable and nonspecific. An asymmetry is the most common finding noted in 44% of cases. Irregular mass(es) are present in 16% to 34% of cases. Axillary lymphadenopathy and skin thickening are less common findings (18% and 7%, respectively). Calcifications are rare.2–5 GM can be occult by mammography.
By sonography, the imaging findings are also variable and nonspecific. Hovanessian Larsen et al. 2 found the most common sonographic finding to be a large, irregular hypoechoic mass with multiple tubular extensions, which was seen in 59% of cases. Skin thickening was noted in 52% of cases. GM presented with a lobulated or irregular hypoechoic mass in 33% of cases. Axillary lymphadenopathy was noted in 28% of cases. When presenting as a mass, the mean diameter ranged from 0.8 to 6 cm. Other studies have also described perilesional echogenicity as well as intralesional and perilesional hypervascularity. Another study described dermal fistulae in as many as 50% of patients.2–5
The primary differential diagnosis for GM is invasive breast carcinoma (IBC). Breast carcinoma is the most common cancer in women in the United States and the second leading cause of cancer-related deaths. The appearance of IBC by sonography varies, but the most common appearance is an irregular hypoechoic mass—similar to GM. The tubular extensions described with GM are much less common with IBC but are nonspecific to both entities. Given the overlap of symptoms and appearance on clinical imaging, tissue sampling is used to histopathologically confirm the diagnosis. Image-guided core biopsy is diagnostic for GM in 96% of women. Fine-needle aspiration is only diagnostic in 21% of cases. 8 There are no studies describing the validity or reliability of sonography in diagnosing GM or in differentiating it from IBC, although anecdotally both would be low.
Conclusion
Granulomatous mastitis is a rare and benign breast disease commonly affecting women of childbearing age. The symptoms and imaging characteristics are commonly similar to invasive breast carcinoma. Image-guided tissue sampling is typically needed to differentiate the entities. Granulomatous mastitis is often a chronic condition either being refractory to treatment or recurrent.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.