
Abstract
This methodological approach to assessing obesity is based on the prepilot work conducted on a small sample of men and women (25-58 years of age) in a laboratory setting. The use of skinfold calipers, body mass index, and sonographic imaging of adipose and visceral fat were obtained. In this pre-experimental work, the rigorous use of sonographic measures of visceral fat demonstrated better trend results than the other measurement tools. The sonographic methods employed were modeled after the work published by Hamagawa et al. All measurements were taken five times, and only the middle three were retained for mean data points. The data are compared and contrasted with a paucity of international studies using sonography to measure visceral adiposity. It is important to determine whether sonography could serve as a non-ionizing imaging technique for the assessment of body composition and a screening technique for cardiovascular disease prediction.
Keywords
Introduction
Obesity remains a significant public health issue that is associated with a reduced quality of life, multiple comorbidities, and multicausal mortality.1–3 In the United States, more than one-third of adults and children are overweight or obese.4,5 The most widely cited assessment scheme for obesity is based on the World Health Organization’s international classification, which relies on body mass index (BMI). 6 Although BMI is moderately correlated with more direct measures of body composition,7–9 it fails to differentiate between the layers of body tissues. The prevalence of normal weight obesity, a condition of having normal body weight with an excessive amount of body fat, has been associated with significant cardiometabolic dysregulation, metabolic syndrome, and cardiovascular risk, which casts doubt on studies relying solely on BMI as a measure of obesity. 10 Epidemiological studies have also used waist circumference, waist to-hip ratio, and sagittal diameter to estimate abdominal fat, yet these measures fail to differentiate between visceral and abdominal subcutaneous fat. 11 Clinicians are encouraged to use BMI and waist circumference as screening tools for determining obesity in adults and children.11,12
The visceral fat layer extends from the anterior surface of the liver to the linea alba, while the subcutaneous fat extends from the skin to the linea alba. Discerning between specific tissue deposits and phenotypes is critical given the evidence supporting the metabolic consequences that are dependent on the location of the fat deposit. Metabolic syndrome is a term used to connote the risk factors that can raise a person’s risk for cardiovascular disease and stroke. 10 Abdominal visceral fat deposits can initiate the pathogenesis of metabolic syndrome, which can also be a contributing factor for the development of type 2 diabetes and cardiovascular disease. 13 The gold standard for quantitative assessments of intra-abdominal adiposity is computed tomography (CT) and magnetic resonance imaging (MRI), but widespread utilization remains limited secondary to accessibility and cost. 14
Researchers have attempted to use diagnostic medical sonography (DMS) to measure visceral fat layers; however, most have documented limitations that were related to low-frequency transducers and inconsistent scanning protocols.15–17 A promising study, conducted by Bazzocchi et al., 17 compared DMS measures to CT at similar anatomical slices. If DMS were to be used to measure intra-abdominal adiposity, the next step would be to compare results with dual energy x-ray absorptiometry (DXA). A DXA is a low-dose ionizing radiation diagnostic scan that can be used as a measurement tool for body fat.14,15 Comparing DXA to DMS for measuring intra-abdominal adiposity would provide additional validation as to the proper diagnostic tool that should be used. The added value of using a non-ionizing technique to screen for intra-abdominal adiposity and associated cardiovascular disease risk could be important in translating this diagnostic technique for patient assessment.
The American College of Radiology’s (ACR’s) Appropriateness Criteria is an evidence-based tool that is widely used to guide physicians and practitioners in making appropriate recommendations for diagnostic testing. The ACR recommendation for assessing risk in an asymptomatic patient, at low risk for cardiovascular disease, is CT calcium scoring; however, the rating is usually not appropriate. 18 With a patient of intermediate risk, the rating for CT increases to a rating of usually appropriate. 18 The risk for progressive metabolic disease is categorized differently, and the ACR recommends a screening cardiac MRI with stress and intravenous contrast. 18 It would appear that less invasive and reduced levels of ionizing radiation could be used to screen patients at risk for progressive metabolic and cardiovascular disease. The significance of providing a nonionizing imaging technique for measuring abdominal visceral fat has the potential to assist physicians and patients in making proactive treatment decisions.
The utilization of DMS to measure abdominal visceral fat would require more scientific evidence to raise the ranking of this nonionizing technique and accelerate its recommendation for screening high-risk patients. Given the increasing rate of childhood obesity, it would also seem important to promote a nonionizing imaging technique for pediatric patients at risk for early development of cardiovascular disease.
Literature Review
A Brazilian study was conducted with a cohort of 100 women who consented to an anthropometric evaluation including bioelectrical impedance, DXA, DMS, and a CT scan. 19 In this research, the technique, descripted by Bazzocchi et al., 17 was used to take abdominal visceral fat measurements with modern DMS equipment. Multiple measurements were taken, and an average was retained across the data set. The CT evaluation of abdominal visceral fat was selected as the gold standard, and all measurements were compared for a possible non-ionizing match. This study found that waist circumference, waist-to-hip ratio, and DMS measures of visceral fat were the best correlated matches with values of visceral fat detected by CT. 19 In fact, a value of 6.90 cm of visceral fat measured from a DMS image was deemed as an indicator of visceral obesity and had a specificity of 82.8%, a sensitivity of 69.2%, and correlated with CT at 74%. 21 Given that this study was conducted on adult women with a mean age of 50 years and limited range of obesity, a larger group of subjects would provide more robust evidence.
In previous studies, the same group of researchers recruited a sample of 101 women who consented to DMS for the purpose of assessing their abdominal visceral fat and also with a CT scan. 20 In this sample, clinical blood biomarkers of cardiovascular risk were also obtained. Again, the DMS image measurements of abdominal visceral fat matched the CT images; however, they also were moderately correlated with fasting insulin (r = 50.29 and r = 50.27, P < .01) and plasma glucose 2 hours after oral glucose load (r = 50.22 and r = 50.34, P < .05). 18 The fasting insulin was a clinical tool used to identify patients with prediabetes. This study underscored the ability of DMS image measurements to approach not only CT measurements of abdominal visceral fat but also the predictive ability that these measures could have compared to CVD-specific biomarkers. Of note, one limitation was the lack of specificity as to the DMS measure site. The authors only described taking the measures “above the umbilical knot.” For reproducibility, the measurements taken from all imaging studies need specific landmarks. Like the other study, this group of women had a mean age of 50 years and were relatively homogeneous in terms of anthropometry. 18
In a large Chinese study, 4301 hypertensive inpatients were recruited for a study using mixed assessments to detect cardiovascular disease and visceral fat measures. 21 The results documented that waist circumference was the best predictor of a diagnosis of cardiovascular disease followed by BMI, waist-to-hip ratio, bioelectrical impedance, then intra-abdominal fat distance measured from DMS, compared with CT. 21 Because this study was published in Chinese, the precise methods were difficult to discern. Of interest is the cutoff values that they published for both men and women based on their work. Since this study was likely based on data from a convenient sample of patients, it hampers the generalizability of the findings.
To detect visceral adiposity and early stages of metabolic and possible cardiovascular disease, a pilot study was designed to determine whether the scanning and sonographic measures stratifying subcutaneous and visceral fat is relatively low cost, nonionizing, and replicable.
Materials and Methods
A pilot study was completed in 2016 with a group of five volunteers of mixed gender, age, weight, and adiposity. For this study, a convenience sample of participants was recruited from a university setting, via email. Prior to participation, a short orientation was given to provide information about the testing procedures and to obtain a verbal consent. Data collected included a DMS scan, abdominal skinfold, body weight, and height measurements.
Sonography
DMS uses high-frequency sound waves that penetrate the skin surface and travel into body tissues, recording the reflected signal. 22 The GE Healthcare Logiq i (Milwaukee, WI) ultrasound was used for this pilot. The transducer selected as a 12-MHz linear that was upshifted to 16.0 MHz and adjusted to an output power of 100% (MI: 0.13). Acoustic gel was applied to the transducer, to reduce the loss of acoustic power at the air-tissue interface. The transducer was then placed perpendicular to the tissue interfaces. 22
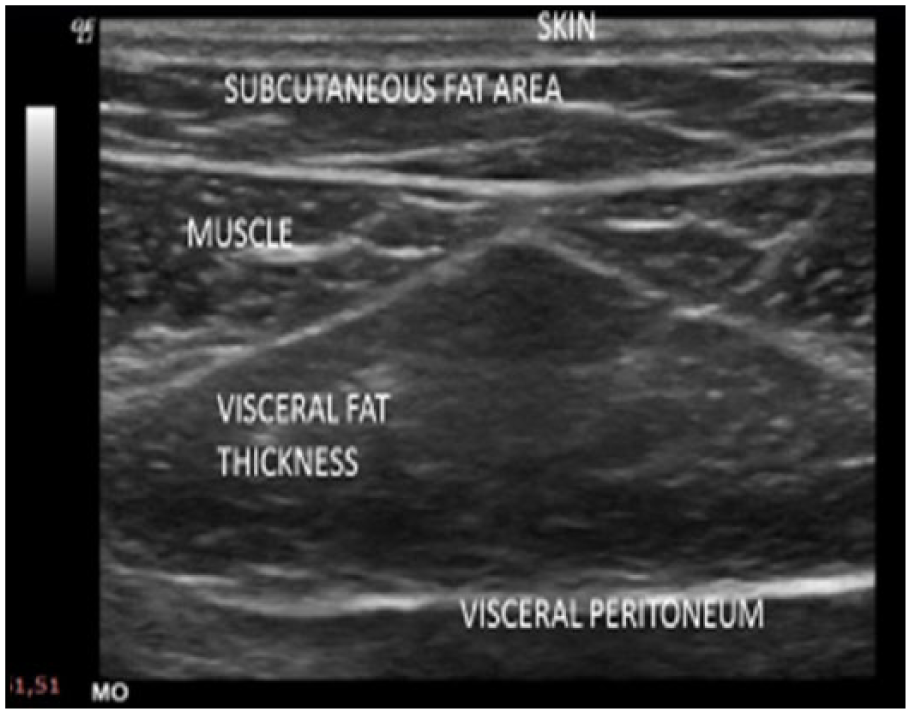
Participants were scanned using the protocol, described by Hamagawa el al. 23 ; however, this technique was enhanced by using a cine loop of the sagittal area, obtained from the xiphoid process to the umbilicus. Using a cine loop, a scan in the sagittal plane facilitated the measurement to be taken using the “run-stop” function, retrospectively. An electronic caliper was used to measure the subcutaneous fat thickness from skin (cutaneous boundary) to the linea alba, and the visceral fat thickness was measured from the peritoneum boundary to the linea alba (Figure 1). Measurements were recorded and coded as S min, referring to the subcutaneous fat measurement taken at the narrowest point. V max was used to indicate the visceral fat measured at two locations, close to the xiphoid, and visceral fat was measured at the widest point (Figure 2). The Hamagawa technique was used as a guide in scanning, measuring, and recording data from the sonographic images (Figure 1).
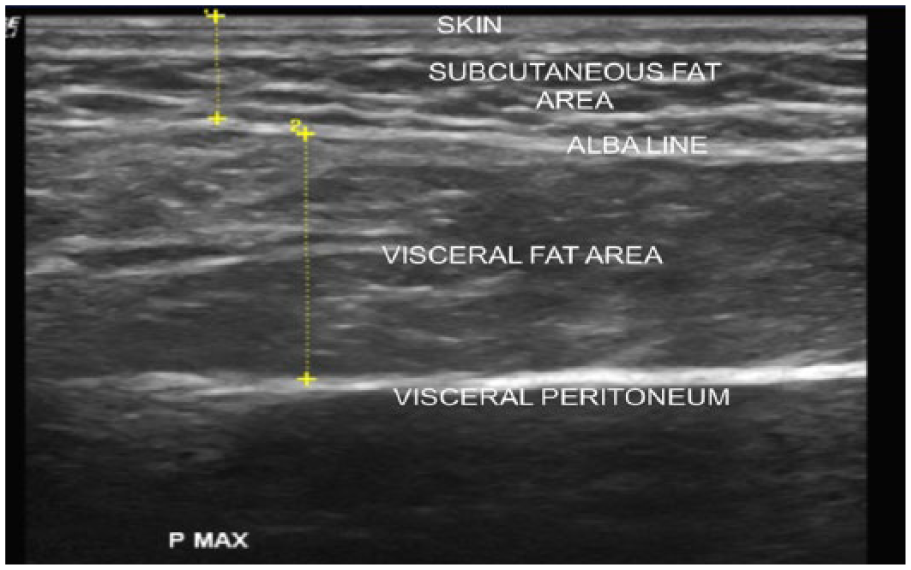
The sonographic image documents the amount of abdominal adipose tissue. Sonographic measurements of thickened visceral fat are compared with subcutaneous fat.
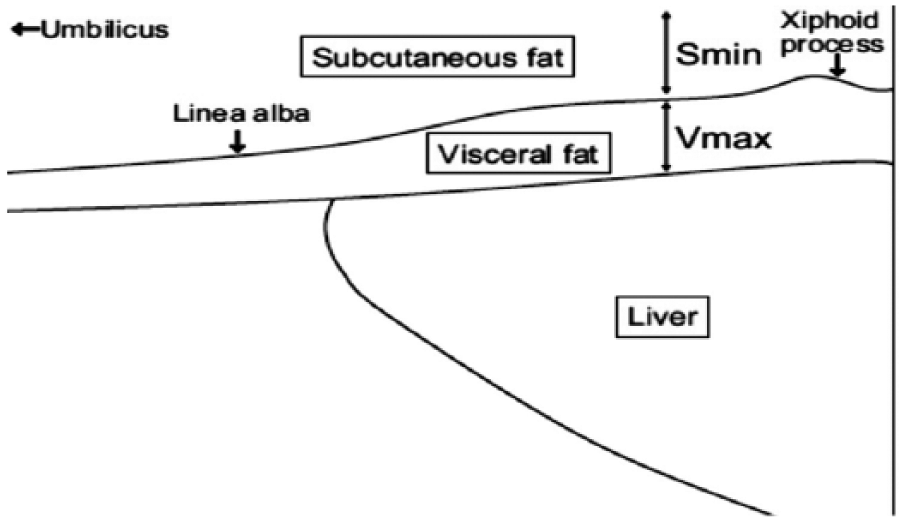
The methodology of Hamagawa et al. 23 for capturing the sonographic image longitudinally and also the anatomical landmarks for making the measurements. Reproduced with permission from the author.
Abdominal Skinfold Measurement
Abdominal skinfold caliper measurements were taken on the right side of the abdomen by a trained interventionist using calibrated Lange calipers, about 1-inch lateral from and 0.5 inches below the umbilicus. Each measurement was taken five times, with the recorded score being the median value of the five scores. 24
BMI
A calibrated scale and a wall-mounted stadiometer were used to take measurements of weight and height, respectively. Weight (in pounds) was divided by height (in inches) squared and multiplied by 703: BMI = (weight/height)²) × 703.
Results
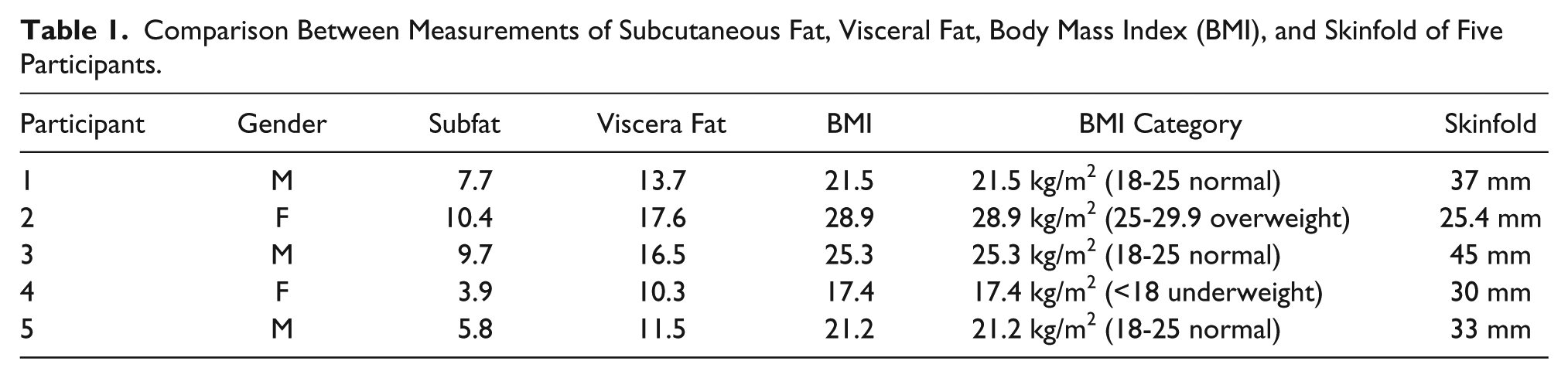
DMS, BMI, and skinfold caliper measures of fat adipose tissue were compared across the convenient sample of three men and two women, ages 25 to 58 years. The data collected were plotted such that the DMS measurement of visceral body fat was compared with the other variables. DMS measures of visceral fat and BMI tended to trend more comparably than the skinfold measurements (Table 1). DMS images are provided from the selected subjects to demonstrate the data collected (Figures 1, 3, and 4).
Comparison Between Measurements of Subcutaneous Fat, Visceral Fat, Body Mass Index (BMI), and Skinfold of Five Participants.
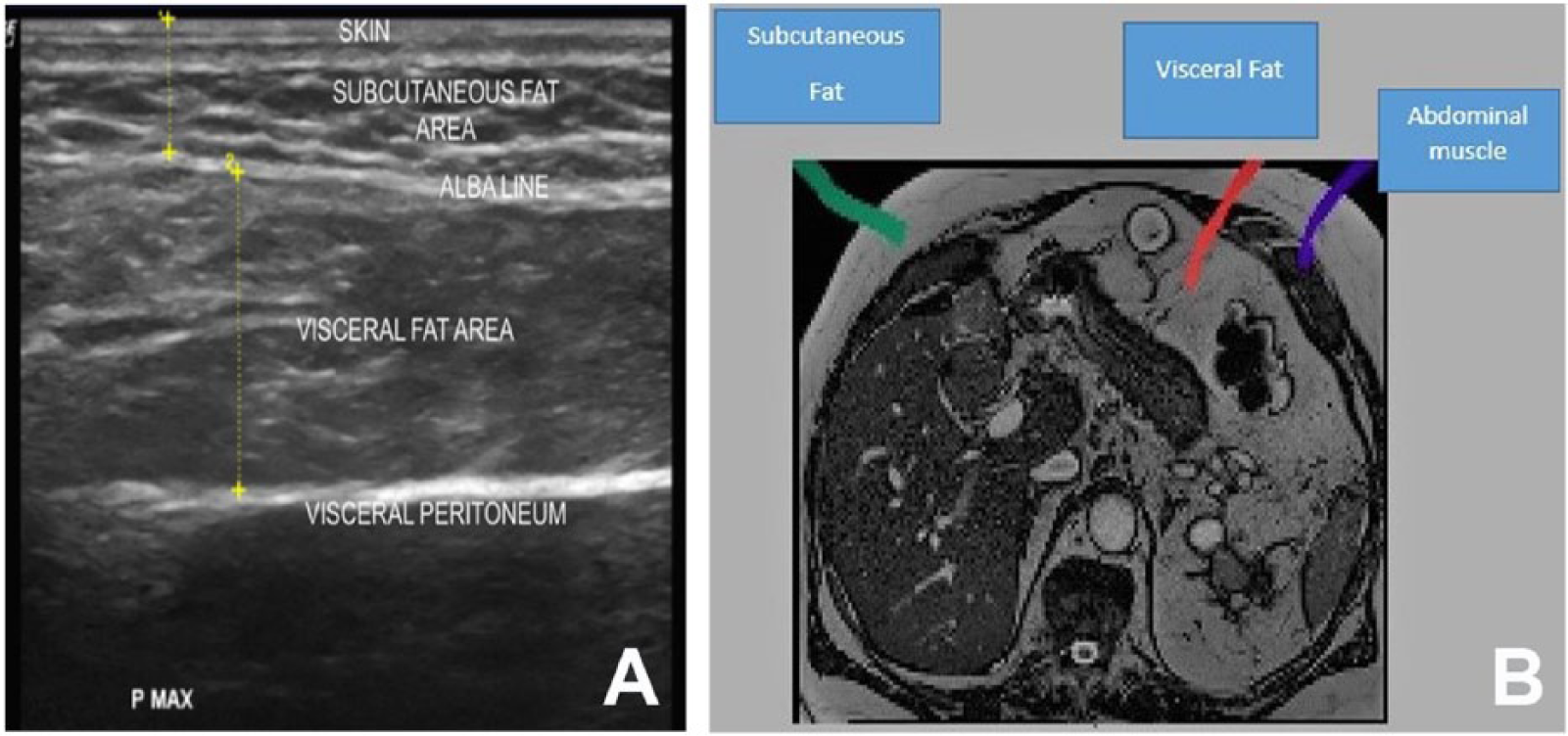
Abdominal adipose tissue is imaged with both diagnostic medical sonography (DMS) (A) and computed tomography (CT) (B). Measurement of DMS and CT adipose layers were imaged at comparable anatomical locations. Measurements were taken at approximately the same level.
Transverse sonographic view of the upper abdominal wall and the linea alba line, which compares subcutaneous and visceral fat layers.
Graph 1 depicts the trending of the data as a result of the data points collected.
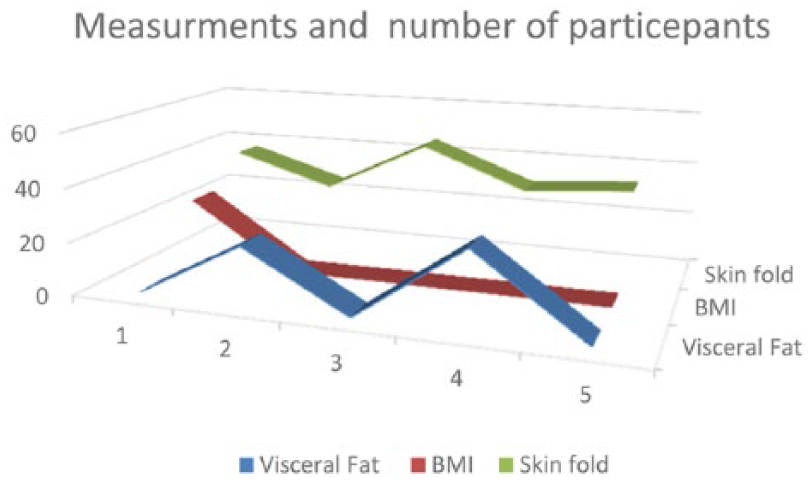
The trend graph demonstrates comparisons between diagnostic medical sonography measurements of visceral fat, body mass index, and skinfold measures.
Discussion
Because of increasing obesity and risk for cardiovascular disease, this pilot points to the feasibility of DMS to measure abdominal fat in a laboratory setting. Given that the volunteers were a mix of men and women of varied age, a study of a similar age range could help to fill in the trend graph. Berker et al. 25 recruited 104 participants, 19 to 58 years of age (men and women) as part of their study. All subjects consented to anthropometric evaluation, bioelectrical impedance analysis, DMS, and CT on the same day. In this much larger study, they determined that the most effective method for matching visceral fat on CT was the visceral thickness measured with DMS, among the male participants. 25 In contrast, the best match for measurements of visceral fat in women was a combination of measures with DMS, BMI, and waist circumference. 22 This would suggest that DMS could be used as a nonionizing imaging technique for detecting visceral fat, but due to the variety of anthropometrics among women, it might be important to use mixed measurements.
The prevalence of childhood obesity is increasing at an alarming rate. More than one-third of children are overweight or obese.4,5 To provide screening of children with a propensity for obesity and early cardiovascular disease, a nonionizing imaging technique would be important. It would also allow for quantifying visceral obesity in pediatric patients given that BMI and skinfold measurements are unreliable and CT imparts radiation exposure. In a study of 73 pediatric patients, ages 7 to 13 years, biomarkers and visceral fat measurements were obtained. Results of this study demonstrated a strong positive correlation between DMS measures of visceral fat and categories of obesity. DMS measures of visceral fat were moderately correlated with a homeostasis model assessment for insulin resistance score (r = 0.403, P < .001). 26
This pilot is innovative as it applied high-frequency transducers to obtain the highest level of resolution and additionally demonstrates feasibility that this measurement technique can be further tested for both accuracy and reliability. As mentioned earlier, clinicians are encouraged to use BMI and waist circumference for assessing obesity in adults and children.11,12 This pilot study would suggest that DMS measures could be a possible tool that would provide more global data to that assessment.
In addition, as a nonionizing imaging technique, this is a tool that could be expanded to address the United States Department of Agriculture’s childhood obesity prevention strategies as a safe and accessible tool for quantifying visceral adiposity and predicting risk of obesity-related disease. 27 Sonographic techniques have tremendous potential as a screening tool; however, prospective studies that adopt this sonographic technique should adhere to the current evidence promoting inclusion of a battery of biomarkers to ensure maximum effectiveness. In summary, these early findings support the feasibility of DMS to measure abdominal fat in a clinical or community setting, particularly in pediatric populations.
Footnotes
Acknowledgements
The research team would like to thank The Ohio State University’s Clinical Research Center staff. The dedicated staff and graduate students make this ongoing research possible as well as provide valuable assistance to these patients.
A supplemental video is available online with this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.