
Abstract
The accumulation of abdominal adiposity has been associated with many risk factors in adults and children. Currently, body mass index (BMI) percentiles, computed tomography (CT), and dual X-ray absorptiometry (DXA) are widely used to evaluate body fat but are not widely acceptable for measuring visceral and subcutaneous adiposity. The aim of this study was to evaluate abdominal adiposity in children by the use of diagnostic medical sonography (DMS). Fifty-eight third graders were recruited for a 10-week interventional study. This cohort received baseline body composition and anthropometric measures, including height, weight, calculated BMI percentiles, blood pressure, bioelectric impedance, and DMS. The resulting data analysis provided a set of descriptive statistics. DMS may be a reliable, practical, and cost-effective method for measuring visceral and subcutaneous adiposity across varied body compositions of children.
According to the Centers for Disease Control and Prevention (CDC), the percentage of obesity in children and adolescents has more than tripled since the 1970s. 1 The prevalence of obesity among children in the United States has reached rates of 13.9%, 18.4%, and 20.6% in children ages 2 to 5 years, 6 to 11 years, and 12 to 18 years, respectively. 2 The prevalence of overweight obese adults and children has become a national public health crisis, affecting over 13 million children and adolescents across the United States. 2 The increased rates of childhood obesity have put these individuals at risk for chronic health conditions, diseases, and pathologies. 1 The increasing rate of childhood obesity will also increase the likelihood of adult obesity and associated comorbidities, including but not limited to type 2 diabetes, fatty liver, glucose intolerance, and increased incidence of metabolic conditions in youth. 3 Obesity is a major determinant for cardiovascular disease and a risk factor for type 2 diabetes. The progression of type 2 diabetes typically begins with the accumulation of abdominal adiposity or abdominal obesity. 4 In addition, childhood obesity is associated with increased risk for atherosclerosis and mortality due to adult cardiovascular disease, regardless of an adult’s weight. 5
To define obesity in children, the CDC uses age- and sex-specific body mass index (BMI) percentiles. Size and growth patterns of children and adolescents are used to categorize BMI percentiles (Table 1). 2 These BMI percentiles are referenced versus the standard adult calculations, and this is mainly due to the varied body compositions of male and female children at different ages. 6 BMI percentiles have become the standard for determining overweight and obese children, although BMI is an incomplete assessment due to the complex behaviors of obesity. 7
Body Mass Index for Weight Status Categories With Corresponding Percentiles.

The rising trend in childhood obesity would suggest a need to advocate for screening and early diagnosis of disease and metabolic conditions in children and adolecents. 4 Screening children and adolescents for an earlier diagnosis could promote preventative measures and early treatment. It may also help to lower the risk for future chronic disease implications in adulthood. An accumulation of abdominal adiposity in adolescents has been shown to be associated with disorders such as cardiovascular disease and metabolic syndrome. 6 An accurate and reliable tool that measures visceral adiposity to screen children and adolescents for disease risk should be readily available. BMI, waist circumference (WC), and waist-to-hip ratio have shown to be better correlated with total body fat distribution when compared to direct measures of visceral fat. 6 The use of computed tomography (CT) and magnetic resonance imaging (MRI) is often not readily available and is an expensive screening tool. Previous research has used dual X-ray absorptiometry (DXA) to estimate visceral fat accumulation. Lee et al. 6 used an algorithm that estimates the mass and volume of visceral fat in the android region to both evaluate and estimate visceral fat in girls aged 9 to 13 years. 6 Lee et al. 6 suggested that DXA estimated visceral fat measures almost as well as MRI in this particular cohort of participants. DXA (android percent body fat, subscore) in addition to WC improved the estimate of the visceral fat measurements. 6
Although DXA could be used as an alternative to MRI or CT, it still does not have the capability of definitively differentiating visceral and subcutaneous fat layers within the abdomen. In addition, DXA is not readily available and requires low doses of ionizing radiation to make an indirect quantitative assessment. DMS has been shown to accurately measure visceral adiposity compared to CT. 8 Previously, DMS has been a screening tool researched to measure subcutaneous and visceral fat in adults.9,10 The use of DMS to measure abdominal adiposity in children has not been extensively researched previously. The gap in the literature points to the need for a safe and accurate screening tool for assessment of abdominal adiposity. The use of DMS has safety benefits due to the use of nonionizing radiation compared to the ionizing radiation methods of DXA and/or CT. Therefore, the objective for this study was to pilot the use of DMS as an accurate and reproducible tool to measure visceral fat in children and adolescents.
Subject Population and Methods
Fifty-eight third-grade children aged 8 to 10 years were recruited for a 10-week study (31 males and 27 females). This study, data collection, and intervention materials were approved through the sponsoring university’s internal review board and elementary school system. Participants were asked to attend a day of data collection at a research center prior to the study intervention. Prior to data collection, a verbal and written consent process was conducted for participants and their parents/guardians. During their initial visit, these participants underwent multiple anthropometric measures and imaging as part of the data collection. These specific measures recorded were height, weight, bioelectrical impedance, blood pressure, skin carotenoids, and DMS measures.
Anthropometric Measures
Height and weight were measured to calculate participants’ BMI percentiles. Percentiles were calculated using the CDC growth charts. 1 A registered dietitian performed bioelectrical impedance and blood pressure measures. Body fat percentages were generated using bioelectric impedance. DMS measures were conducted on a GE Logiq i (Milwaukee, WI) ultrasound machine with a 9.0 (6–8 MHz) linear transducer. An optimized protocol referenced by Woldemariam et al. 11 and Stigall et al. 9 was used to measure the visceral and subcutaneous adiposity of each participant. Trained and credentialed sonographers performed all the imaging and data analysis. Cine clips and static images were taken from the xiphoid down to the umbilicus in the sagittal plane. An additional transverse image was taken at the middle of both iliac crests (the level at which waist circumference measures are performed). These images were then analyzed by a trained sonographer, and measurements of visceral fat (minimum and maximum), subcutaneous fat (minimum and maximum), and mesenteric fat thickness were measured at the appropriate levels (Figures 1–3). Differences of anthropometric and imaging measures significance between males and females were determined by a sample t test. The a priori value, set at P < .05, was considered statistically significant.
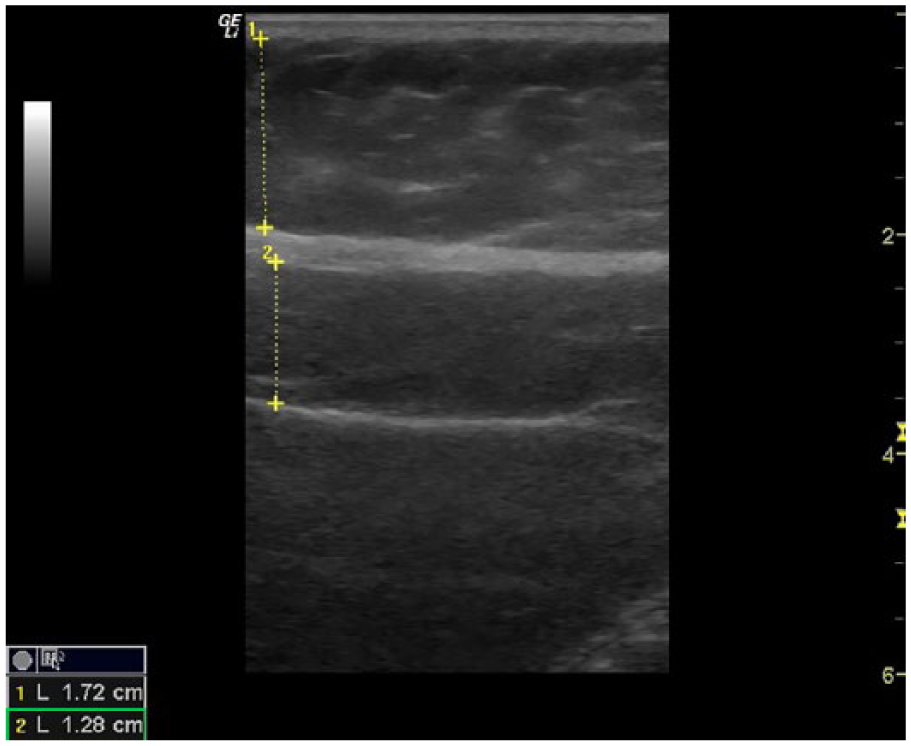
Sagittal image taken at the level of the xiphoid. Subcutaneous minimum measurement (1), visceral maximum measurement (2).
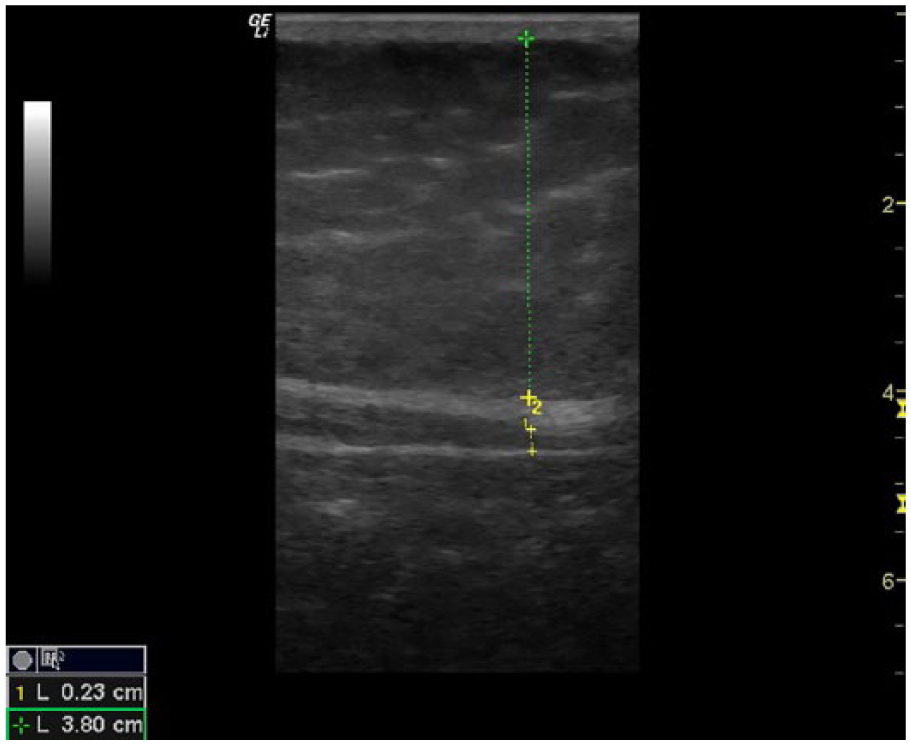
Sagittal image taken at the umbilicus. Subcutaneous maximum measurement (green dotted line), visceral minimum measurement (yellow dotted line).

Transverse image taken at level of iliac crests. Mesenteric fat thickness measurement (green dotted line).
Results
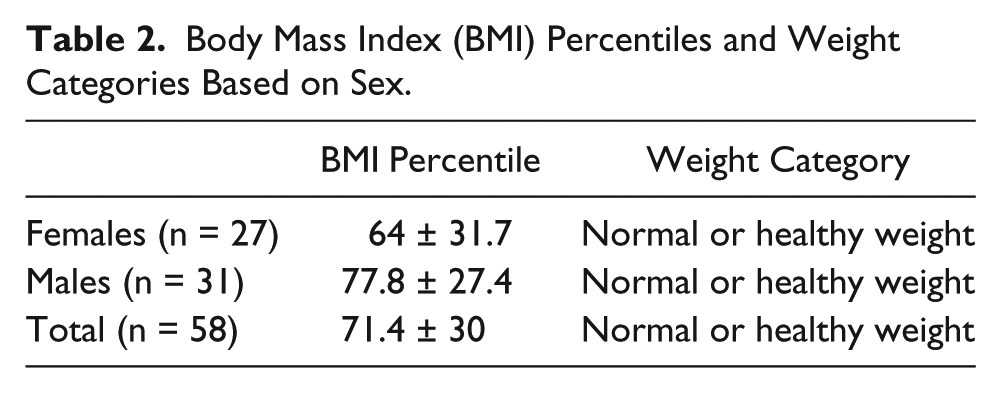
This was a convenience sampling of children recruited for this study. The cohort was fairly balanced for sex and also for age, with the minimum age being 8 and the maximum being 10 years old. The mean (SD) BMI percentile was 71.40 (30). As a group, these participants were classified at the upper limits of the normal or healthy weight category. The breakdown of BMI percentiles is shown in Table 2. In addition, clinical data are summarized in Table 3. Included are age, weight, height, BMI, BMI percentiles, percent body fat, and all sonographic measures. Adiposity measurements of the participants prior to intervention were acquired from the sonographic images taken as previously described. The mean BMI percentile for males was 77.80, whereas the mean BMI percentile for females was 64.00. Height, weight, and sonographic measures did not differ substantially. Overall, there were minimal differences in anthropometric measures and DMS measures regardless of sex. The sample t test is shown in Table 3. The closest measure to significance was the BMI percentiles at 0.08.
Body Mass Index (BMI) Percentiles and Weight Categories Based on Sex.
Participant Characteristics and t Test Showing Difference Between Males and Females.
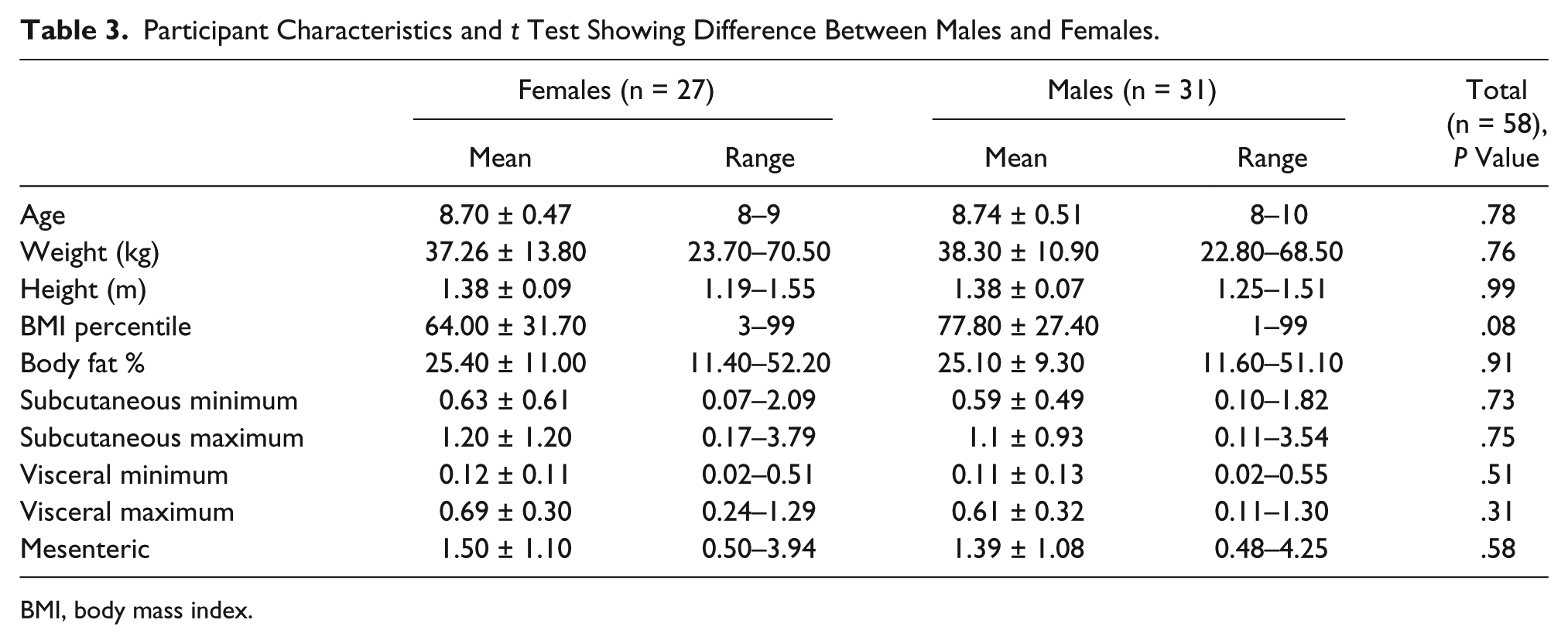
BMI, body mass index.
Discussion
The descriptive results of this convenience sample of 8- to 10-year-olds depicts them as on the upper limits of the normal or healthy weight category. This is very comparable to a convenience sample of 6- to 8-year-old children who underwent a similar baseline set of measurements. 12 In the Liem et al. 12 study, DMS was used as well as DXA, CT, and skinfold thickness. In that study, they determined that mesenteric fat could be adequately measured but the subcutaneous fat could not. In the current study, obtaining a high-quality subcutaneous minimum measurement was challenging due to the thin layer of skin and fat. Unlike the Liem et al. 12 study that found that skinfold thickness was the best gauge for overall pediatric adiposity, this study worked to solve the imaging challenges and confidently record the subcutaneous fat layer. In the present study, the thinner participants were imaged with a stand-off pad to increase the resolution of the subcutaneous fat layer and corresponding measurements. The difference in results between the Liem et al. 12 study and the present study is most likely due to higher quality transducer technology, the use of a linear broad bandwidth transducer, and the use of a stand-off pad and gel.
In a study by Semiz and Sabir, 13 male and female participants aged 11 to 12 years were similarly assessed for abdominal adiposity. In this study, DMS, skin calipers, and anthropomorphic techniques were used to measure the depth of subcutaneous, visceral, and abdominal fat. 13 These researchers concluded, after collecting DMS images with the same protocol as the present study, that BMI was a better classification of obesity than DMS or skin calipers. In contrast to Semiz and Sabir, 13 the use of a curvilinear 3.5-MHz transducer for imaging the subcutaneous, visceral, and abdominal fat had to be a limiting factor. Skinfold calipers were also likely to be less tolerated by children approaching their teens. Therefore, the present study does advocate that using DMS for assessing abdominal adiposity is challenging with children but needs to leverage the use of image optimization to provide the highest quality images for measurement.
Measuring visceral adiposity can be less challenging with DMS and therefore has been used to compare with cardiovascular biomarkers. Adult studies have attempted to correlate visceral adiposity with high-density lipoprotein (HDL) cholesterol, triacylglycerol, high-sensitivity C-reaction protein concentrations, and the intima thickness at the common carotid artery. 14 The relationship between these variables has been explored by several researchers.9,11,15 Kim et al. 14 conducted a study containing 240 men and 106 diabetic patients who had DMS measurements of visceral fat taken and compared to the prevalence of cardiovascular disease, dyslipidemia, and metabolic syndrome. Men whose visceral fat measured in the middle to high quartile were found to have greater a prevalence of cardiovascular disease, hypertriacylglycerolemia, low-HDL cholesterolemia, and metabolic syndrome than those in a lower quartile. 14 In addition, women were shown to have a prevalence of metabolic syndrome and dyslipidemia in the middle to higher quartile. 15 Regardless of sex, visceral adiposity accumulation relates to increased risk for chronic conditions and severe illnesses. In a pediatric study, Silveira et al. 16 evaluated the correlation of body fat composition and components of metabolic syndrome across a cohort of adolescents. In that study, 182 obese pediatric subjects, aged 6 to 16 years, had body composition and trunk fat measures obtained with DXA. 16 Participants with higher intra-abdominal adipose tissues were positively associated with increased dyslipidemia, nonalcoholic fatty liver disease, and components of metabolic syndrome. 16 All of these components in the pediatric population could lead to chronic conditions into adulthood.
In a study by Gishti et al., 17 a large group of children was studied to determine if specific abdominal fat measures might be more strongly associated with risk factors in childhood than standard BMI percentiles. 17 They examined abdominal fat distributions associated with cardiovascular disease in 6523 children. 17 Participants received a series of measures that included BMI, DXA, and DMS measures. Gishti et al. 17 suggested that higher fat distribution measures were correlated with increased risk of hypertension, hypercholesterolemia, and clustering of cardiovascular risk factors. In addition, higher abdominal fat mass was associated with increased risk of cardiovascular disease factors independent of BMI. 17 In the current study, there was a difference in BMI percentiles between males and females. This is most likely due to BMI using a holistic approach of looking at the overall body fat distribution, whereas there were minimal differences in sonographic measures of abdominal adiposity. This suggests that DMS has the potential of detecting differential measures of subcutaneous and visceral fat in children aged 8 to 10 years. Although BMI is a traditional method for determining disease risk in children, it does not adequately characterize the risks caused from abdominal adiposity accumulation. The close association of visceral adiposity accumulation and metabolic conditions as well as other disease risk underscores the importance of a DMS screening tool that is reliable, reproducible, and safe for children and adolescents.
In a similar study, cross-sectional images were collected on a convenience sample of 122 African American adolescents and 129 Caucasian adolescents, ages 8 to 19 years, to analyze metabolic syndrome and its relationship to abdominal adipose tissue. 18 Researchers concluded that an increased prevalence of metabolic syndrome was seen in overweight versus nonoverweight youth as predicted by previous studies. In addition, the participants with a higher prevalence of metabolic syndrome had higher visceral fat measurements. 18
Philipsen 19 explored the reproducibility of DMS assessment of abdominal fat distribution in 86 participants. Visceral and subcutaneous fat were estimated with adequate intra- and interobserver reproducibility. 19 They concluded that DMS could be used as a feasible method for determining subcutaneous and visceral fat measures. 19 Mook-Kanamori et al. 20 investigated whether visceral fat measures in children could be determined by DMS compared to CT. DMS measures of abdominal fat correlated with CT measurements ranging from 0.75 to 0.97 (all P < .001). 20 DMS of abdominal adiposity in children highly correlated with CT measures of abdominal adiposity in children. It is suggested that sonographic measures of abdominal fat in children are a valid method for epidemiological and clinical studies. 20
Conclusion
Although the use of DMS as tool for measuring pediatric abdominal adiposity has not been widely studied, previous research and the present study would suggest that with an optimized protocol, DMS could be a reliable tool to evaluate visceral and subcutaneous fat in children and adolescents. Due to the challenges of imaging abdominal adiposity in children, the present study advocates for image optimization and the use of higher quality transducer technology for assessing abdominal adiposity in children. The difference in BMI percentiles between males and females in this study suggests that the use of BMI percentiles may fall short in assessing children’s risk for disease due to the inability of BMI to differentiate fat distribution. BMI uses the evaluation of overall body fat distribution, whereas the minimal differences noted in visceral and subcutaneous fat measures could represent the potential of DMS detecting minimal differences in abdominal adiposity and, therefore, detecting changes sooner and more accurately in abdominal adiposity over time. Based on this descriptive study conducted with an optimized DMS scanning protocol, it is possible to use DMS as a reliable, noninvasive, and easily accessible means of screening children for metabolic conditions, cardiovascular disease risk, and other risk factors. Using this imaging protocol and staging a longitudinal study of children at risk would be highly encouraged to determine if the previous study results could be dismissed.
Limitations
This was a convenience sample of children who volunteered for an interventional study. These baseline measures cannot be generalized as the research design is preexperimental and hampered by threats to internal and external validity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.