
Abstract
Baker cysts are common pathological findings during sonography of the popliteal fossa. Although they can present as a typical, mild variant or have an atypical sonographic appearance, a common feature of them is that their expansion is usually limited in the intermuscular planes or spaces between muscles and knee capsule. Baker cysts extending into muscles are rare. Two cases of a Baker cyst with extension into the medial head of the gastrocnemius (MHG) are reported with sonographic findings. Both of the cases were discovered in females, who had anterior or bilateral knee pain and radiographic features of osteoarthritis. Knee effusion was identified sonographically in both of the patient cases. In the popliteal fossa, Baker cysts were found in both patients with intramuscular extension into the MHG. In the first case, a cystic penetration was noted into the MHG, near the neck of the cyst, having a cone shape and oriented toward the inferior aspect of the muscle. The second case had a cystic penetration into the MHG near the base of the cyst with a tube shape, along its long axis. The possible pathogenesis is discussed.
A Baker cyst is an abnormal fluid distention in the gastrocnemius-semimembranosus (G-S) bursa. G-S bursa is found in the medial aspect of the popliteal fossa, at the intersection between the semimembranosus tendon (SMT) and the tendon of the medial head of the gastrocnemius (MHG).1,2 It is a common pathological finding during sonography of the popliteal fossa. 3 Sonography is becoming more widely recognized as a valuable imaging tool for the diagnosis of Baker cysts.4,5 A common feature of Baker cysts is that they tend to expand in the intermuscular planes or spaces between the muscle and knee capsule.6,7 However, four cases of Baker cysts with extension into nearby muscles have been reported with MRI in the literature.7,8 Among these cases are examples of extension into the vastus medialis muscle and with extension into the MHG muscle. These types of pathological presentations represent uncommon presentations of Baker cysts. In this article, two cases of Baker cyst with intramuscular extension into the MHG are reported with associated sonographic findings.
Case Report
Case 1
A 68-year-old woman with left knee pain was referred for sonography. She had a history of osteoarthritis (OA) of the left knee for five years, but shortly before she visited her physician, the knee pain had increased while walking. The pain was mainly on the medial and lateral sides of the left knee. Physical examination revealed no swelling of the anterior knee but mild swelling in the medial aspect of the popliteal fossa. No tenderness upon palpation was identified. Radiographs demonstrated mild OA change in the medial compartment.
A systematic sonogram of the left knee was performed with a linear high-frequency transducer (8–17 MHz). The suprapatellar recess displayed mild effusion (Figure 1). No other abnormality was identified in the anterior and bilateral sides of the knee. In the medial aspect of the popliteal fossa, a transverse section at the top demonstrated a typical Baker cyst with a superficial body, a deep small base, and a neck between them (Figure 2A). When moving the transducer inferiorly, a small cystic lesion appeared in the MHG near the neck of the Baker cyst (Figure 2B); then the connection of the cystic lesion with the Baker cyst appeared (Figure 2C), and gradually the cystic lesion became much larger (Figure 2D). A sagittal section of the MHG displayed a cone-shaped cystic lesion in the muscle oriented toward the inferior of the muscle (Figure 2E). The largest diameter of the cyst was 1.5 cm, and the length was 2.6 cm. After this examination, the patient was advised by her physician to have a regular follow-up medical appointment to monitor the cyst; no treatment was recommended.
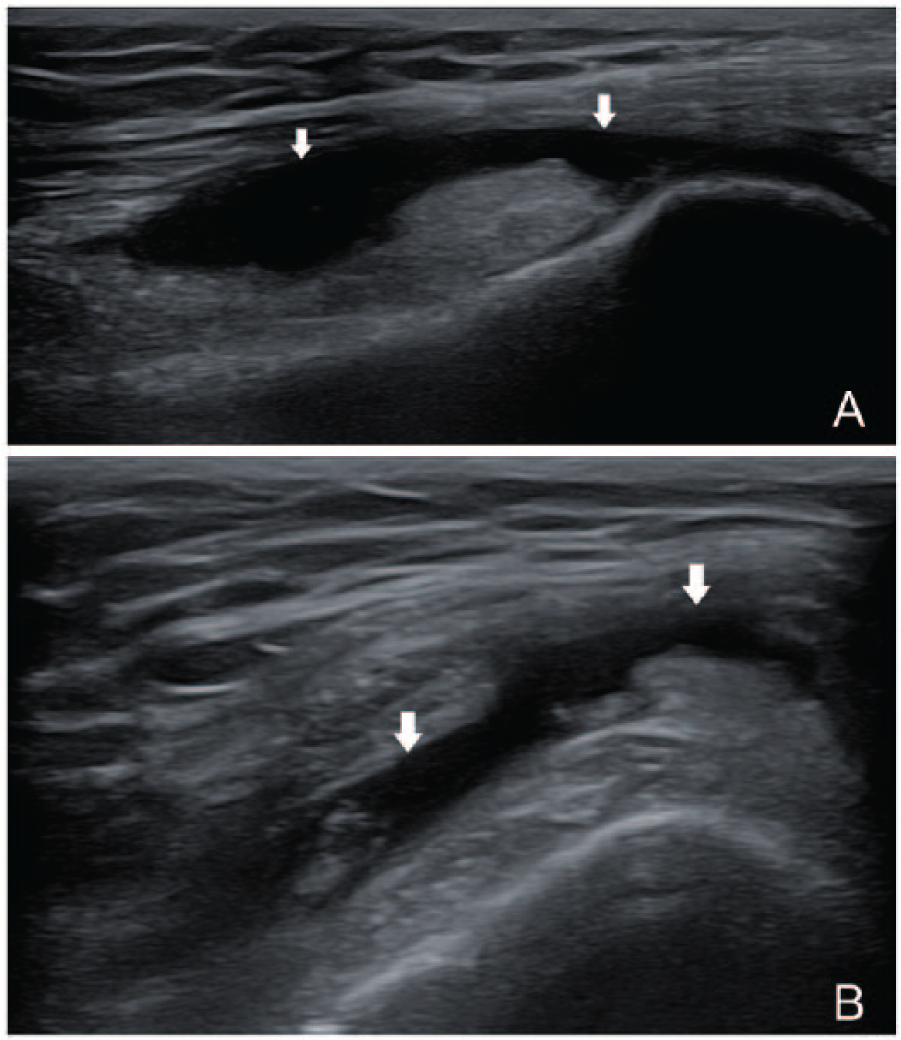
Case 1 knee effusion. Longitudinal (A) and transverse (B) view of the effusion (arrow) in suprapatellar recess.
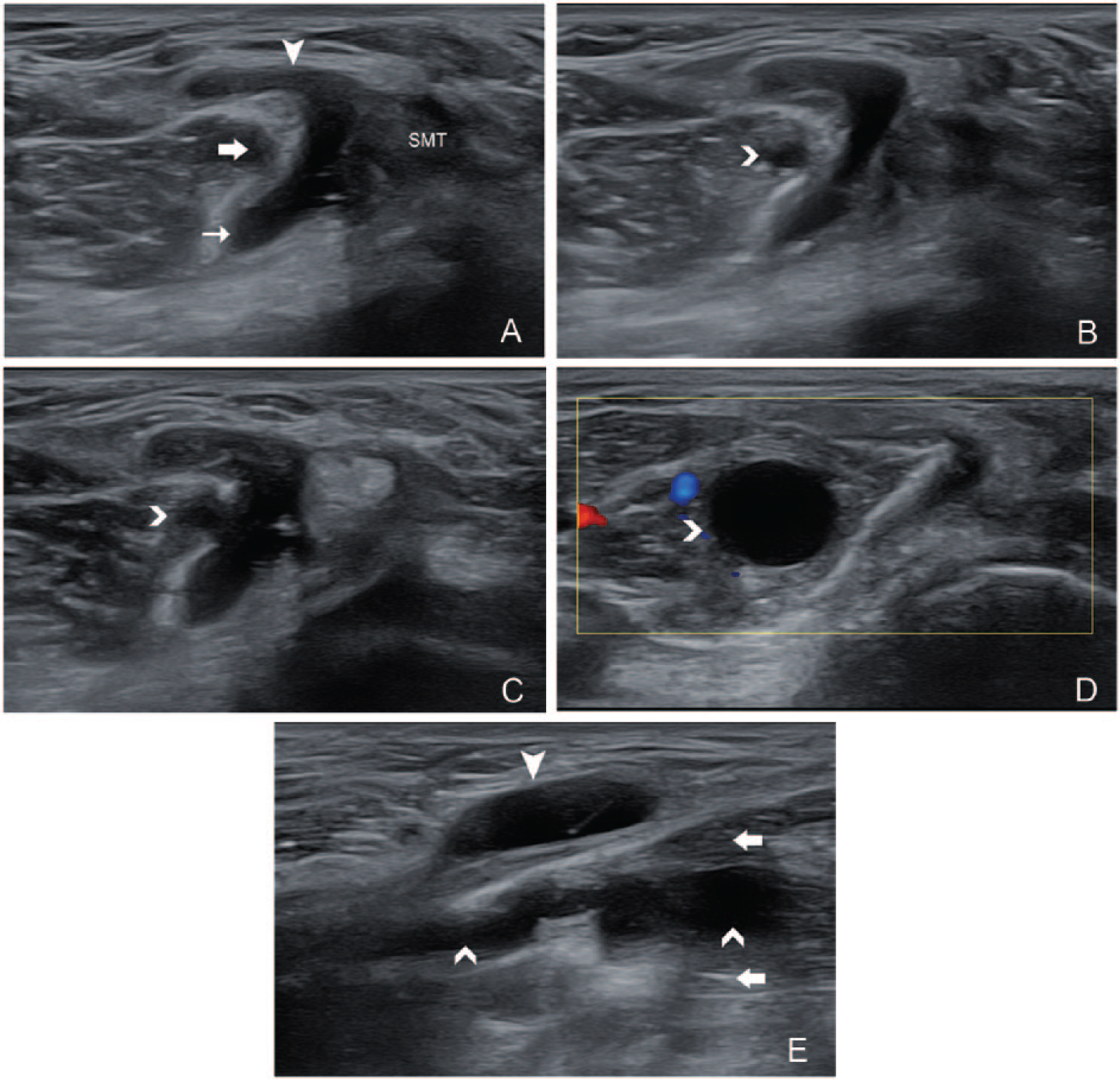
Baker cyst extends into the medial head of the gastrocnemius (MHG) near the neck of the cyst. (A) Transverse view at the top of the medial popliteal fossa: a typical Baker cyst with body (arrowhead), base (thin arrow), and the neck between the MHG (arrow) and semimembranosus tendon. (B) At a lower level than A, a cystic lesion (right-pointed arrow) appeared in the MHG. (C) At a lower level than B, a connection between the cystic lesion and the Baker cyst could be seen. (D) At a lower level than C, the cystic lesion became larger. (E) Longitudinal view of MHG, a cone-shaped cystic lesion in the muscle with its bottom toward the inferior aspect of the MHG.
Case 2
A 58-year-old woman with left anterior knee pain was referred for sonography. She had suffered with pain around the patella for three months. Physical examination revealed no swelling or point tenderness in the anterior or posterior knee. Radiographs demonstrated early OA changes within the left patellofemoral joint.
A systematic sonogram of the left knee was performed with a linear high-frequency transducer (8–17 MHz). The suprapatellar recess showed mild effusion (Figure 3). No other abnormality was identified in the anterior or bilateral sides of the knee. In the medial aspect of the popliteal fossa, a transverse section at the top showed an X-shaped atypical Baker cyst with the deep medial part deep to the SMT (Figure 4A). When moving the transducer inferiorly, a small cystic lesion appeared in the MHG near the base of the Baker cyst (Figure 4B); then the connection of the cystic lesion with the Baker cyst appeared (Figure 4C), and gradually the cystic lesion became smaller (Figure 4D). A sagittal section of the MHG displayed a tube-shaped cystic lesion in the muscle (Figure 4E). The largest diameter of the cyst was 0.7 cm and the length was 3.1 cm. After this sonogram, a follow-up medical appointment was recommended by the physician to monitor the cyst without medical intervention.

Case 2 knee effusion. Longitudinal (A) and transverse (B) view of the effusion (arrow) in suprapatellar recess.
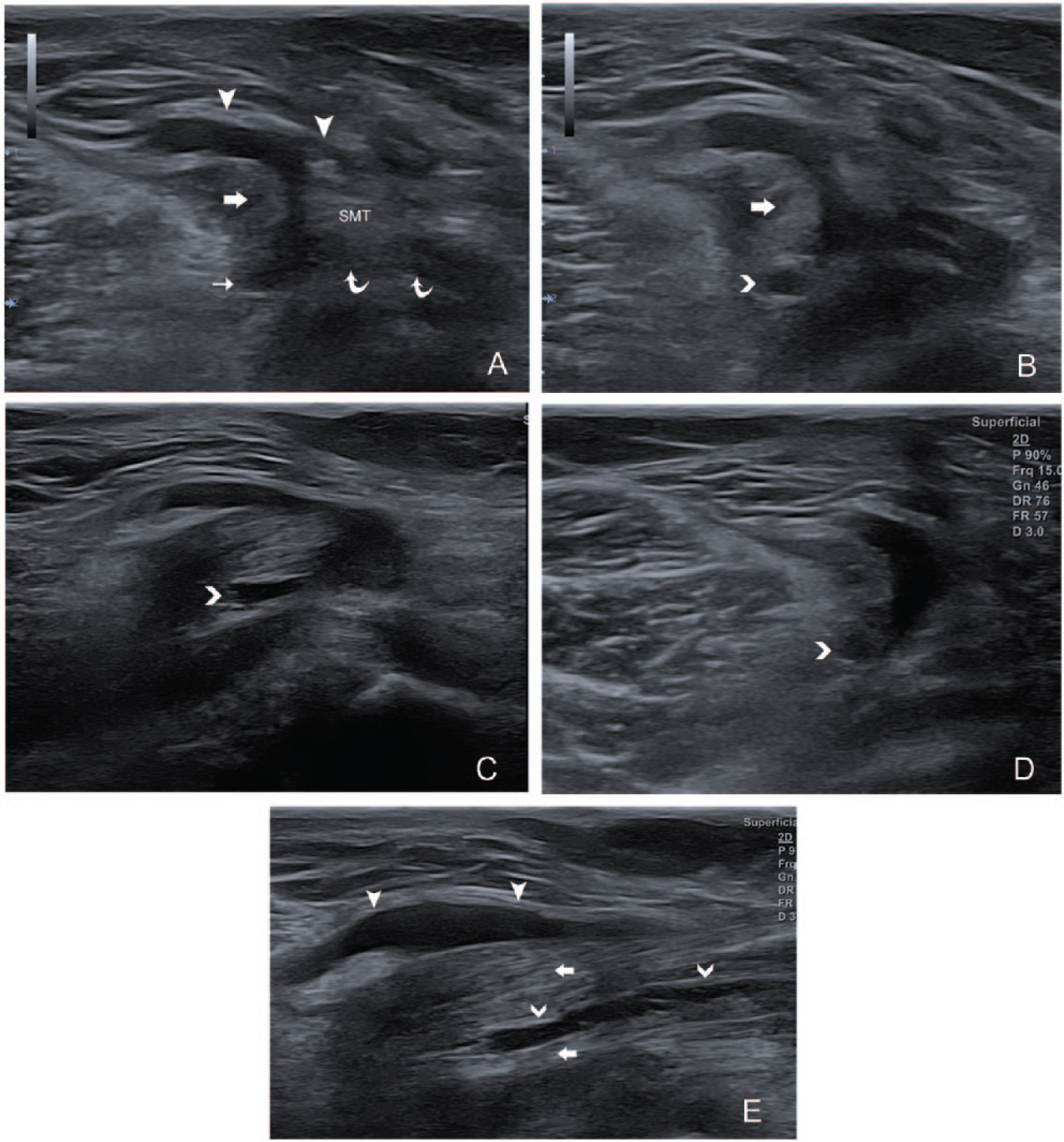
Baker cyst extends into the medial head of the gastrocnemius (MHG) at the base of the cyst. (A) Transverse view at the top of the medial popliteal fossa: an X-shaped Baker cyst with body (arrowheads), base (thin arrow), the neck between the MHG (arrow) and semimembranosus tendon (SMT), and the deep medial part (curved arrows) deep to the SMT. (B) At a lower level than A, a cystic lesion (right-pointed arrow) appeared in the MHG. (C) At a lower level than B, a connection between the cystic lesion and the Baker cyst could be seen. (D) At a lower level than C, the cystic lesion became smaller. (E) Longitudinal view of the MHG, a tube-shaped cystic lesion in the muscle with its narrow end toward the inferior aspect of the MHG.
Discussion
According to the anatomy of the G-S bursa, its proximal portion consists of deep and superficial segments. The superficial segment is located superficial to the MHG, while the deep segment lies close to the SMT and the tendinous surface of the MHG. The two segments of the bursa are connected between the outer border of the SMT and the inner border of the tendon of the MHG. 4 This is the anatomical basis of the X-shaped atypical Baker cyst on the transverse sonographic view. The second patient case represents this type of Baker cyst. However, it is frequently seen that a septa separates the segment of the bursa, deep to the SMT from the rest of the bursa. 4 The effusion in this separated bursa without the deep medial part presents a typical Baker cyst, such as in the first patient case. For a typical Baker cyst, there are three distinct aspects on the transverse sonographic view: the body, the neck, and the base.1–3 The base is the deep part lying deep to the tendon of the MHG but superficial to the posterior capsule of the joint, which has an opening connecting the joint with the base in more than half of adults.4,9 The body is the superficial part of the bursa, while the neck is the connection between the base and the body.
In most adult Baker cysts, the fluid may originate from the knee joint through the capsular opening to the part of the bursa deep to the MHG.4,5,9 The current two cases both have knee effusion, indicating the possible communication between the joint and the Baker cyst. During knee bending with weight bearing, the pressure is high in the joint, which squeezes fluid in the knee joint into the low-pressured bursa through the capsular opening. During extension of the knee, the capsular opening is closed because of the deep segments of the bursa being firmly compressed by the cross-action of the overlying tendons of the MHG, semimembranosus and semitendinosus. 9 Therefore, it entraps the fluid in the deep segment of the bursa, which causes higher intrabursal pressures. This one-way fluid transmission is called functional valve mechanism. 7 The high pressure in the deep segment of the bursa will push the fluid to other parts of the bursa. The result is the decline of pressure in the deep segment of the bursa. When the knee flexes again, the above cycle repeats.9,10 Therefore, the Baker cyst expands and becomes enlarged.
It is presumed that if the surrounding tissue of the G-S bursa is weak and cannot sustain the intrabursa pressure, the bursa may extend into the weak area and expand inside. Since the superficial segment of the bursa is in the subcutaneous tissue and usually sustains lowest pressure compared with other parts of the bursa, mostly the expansion happens in the superficial segment. This could explain the phenomenon that the body of a Baker cyst is usually larger than the base. However, intermuscular planes and the space between the muscles and the posterior capsule of the knee joint all provide space for expansion, depending on the local pressure. Conversely, the cyst can also expand into the nearby muscles.7,8 The current two patient cases both demonstrated the cyst extending into the MHG. The proposed pathogenesis is that weakened muscle fascia or a constitutional focal defect of the muscle fascia may allow for penetration of an expanding cyst under pressure.7,8 For the current two patient cases, no history or clinical findings could provide a clue of focal fascia defect or weak. However, the fact that the G-S bursa functions to reduce the friction between the SMT and MHG could imply possible focal chronic micro-injury and resulting fascia weakness or defect, which renders susceptibility to a high-pressured cyst to dissect into that space. The Baker cysts reported in these two cases expanded into the MHG mainly along the long axis and downward. This could have occurred due to possible weak intramuscular planes between the bundles of muscle fibers in the MHG and the effect of static pressure.
Most of the Baker cysts are asymptomatic for patients. The symptoms of Baker cysts include posterior knee pain, a sense of fullness or a mass in the posterior knee, and reduced knee range of motion.1,11 Although the current two patient cases both had knee pain, the locations of the pain were likely caused by developing OA, as indicated by the radiographs. Therefore, they had no direct symptoms related to Baker cysts and can be classified as having asymptomatic Baker cysts. It is also important to carefully evaluate a meniscal cyst that is located medially as this indicates the potential for a developing Baker cyst in the posterior knee. 12
For asymptomatic Baker cysts, no treatment is required except for the treatment of the underlying cause of the intra-articular knee disease,10,11 which was attributed to OA. For symptomatic Baker cysts, available treatment includes cyst aspiration, corticosteroid injection, or surgical remove of the cyst, depending on patients’ situations.10,11
Conclusion
A Baker cyst with intramuscular extension is uncommon. The patient cases presented demonstrated Baker cysts with intramuscular extension into the MGH, with associated sonographic findings. The postulated pathogenesis of this presentation may be due to focal chronic micro-injury of the fascia of the MHG leading to fascia weakness or defect, which renders susceptibility to dissection under pressure.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.