
Abstract
Takayasu arteritis is a chronic, large vessel vasculitis that typically affects the aorta and its main branches. We present a case of a 33-year-old male patient who was diagnosed with Takayasu arteritis after being admitted for acute cardiogenic shock requiring inotropes. Initial transthoracic echocardiography demonstrated severe biventricular dysfunction. Computed tomography imaging of his chest showed pulmonary infarcts. Patient subsequently developed sudden lower extremity weakness and bowel incontinence, and urgent magnetic resonance imaging of his spine demonstrated thoracolumbar vascular myelopathy. Transesophageal echocardiography revealed diffuse symmetrical thickening of the walls of the aorta; findings suggestive of aortitis. Patient was initiated on intravenous corticosteroid and systemic anticoagulation. Subsequent computed tomography angiography demonstrated irregular luminal contour of the aortic arch, and complete occlusion of the left subclavian artery, abdominal aorta, superior mesenteric artery, and left renal artery. He underwent an emergent aortoiliac thrombectomy. He was transitioned to oral prednisone, tocilizumab, and azathioprine with excellent recovery.
Introduction
Takayasu arteritis (TAK) is a rare form of vasculitis that primarily involves the large arterial vasculature by causing inflammation in the vessel wall. Historically, this disease affects females over males in nine out of ten cases. 1 While TAK primarily affects the large vessels, it was initially discovered by a Japanese ophthalmologist in 1905 who noted abnormal retinal vessel changes associated with abnormality of the aortic arch. 2 In the following case report, we present a case of a male patient who was diagnosed with TAK after presenting with cardiogenic shock and multiorgan dysfunction, notably highlighting the atypical and severe presentation of the patient.
Case presentation
A 33-year-old male of Indian descent, with a past medical history significant for malaria and typhoid fever, presented with an 8-month history of slowly progressive right-sided lower back pain. The patient underwent a course of oral steroids and physical therapy with notable relief under the presumed diagnosis of sciatica by outpatient providers. Approximately 5 months later, he began experiencing similar symptoms in his left lower back, accompanied by paresthesia in the lateral pedal region. A few days prior to his presentation, he developed new-onset dyspnea on exertion, cough, and bilateral lower extremity swelling, which prompted his visit to the emergency department.
Vital signs demonstrated a blood pressure of 150/100 mmHg, a heart rate of 120 s/min, and a temperature of 36.3°C. He was tachypneic with a respiratory rate of 22 breaths/min but was saturating well on room air. Labs were notable for hemoglobin of 9.1 g/dL, white blood cell count of 29.2 × 109/L with neutrophilic predominance, creatinine 3.52 mg/dL, and mildly elevated transaminases. NT-proBNP was elevated to 30,000 pg/mL. C-reactive protein was 175.4 mg/L (normal ⩽8 mg/L). Transthoracic echocardiography (TTE) showed severe generalized left ventricular hypokinesis with an ejection fraction of 17% and moderate-to-severely reduced right ventricular systolic function with right ventricular systolic pressure of 70 mmHg. Bilateral lower extremity ultrasounds were negative for deep vein thrombosis. Computed tomography (CT) angiogram of the chest demonstrated small pulmonary infarcts. He was initiated on inotropic support with milrinone for cardiogenic shock. Left and right heart catheterization revealed no significant coronary artery disease, with pressure parameters suggestive of compensated cardiogenic shock while on inotropic support. During the procedure, concerns were raised about a possible thromboembolic event when the patient suddenly experienced a loss of sensation and motor strength in the lower extremities. Urgent magnetic resonance imaging of the spine revealed findings suggestive of thoracolumbar spine infarction, secondary to thoracolumbar vascular myelopathy.
Post-procedure, the patient was transferred to the intensive care unit (ICU) for further management. He was started on norepinephrine to augment spinal cord perfusion, along with heparinization for suspected spinal cord infarction. His urine output started to decrease with a worsening creatinine of 3.9 mg/dL, which necessitated the initiation of continuous renal replacement therapy. The patient was noted to have a discrepancy in blood pressure in the bilateral upper extremities, with the right side being ~40 mmHg higher than the left.
To exclude a cardioembolic source of stroke, a transesophageal echocardiography (TEE) was performed, which revealed diffuse symmetrical thickening of the walls of the aorta, findings suggestive of aortitis (Figure 1). Prior to the TEE, there were no changes in the vascular wall that were detected on other imaging modalities. Patient was also confirmed to have a moderately to severely enlarged left ventricular chamber with an estimated ejection fraction of 20%, severe generalized left ventricular hypokinesis with normalized right ventricular function.
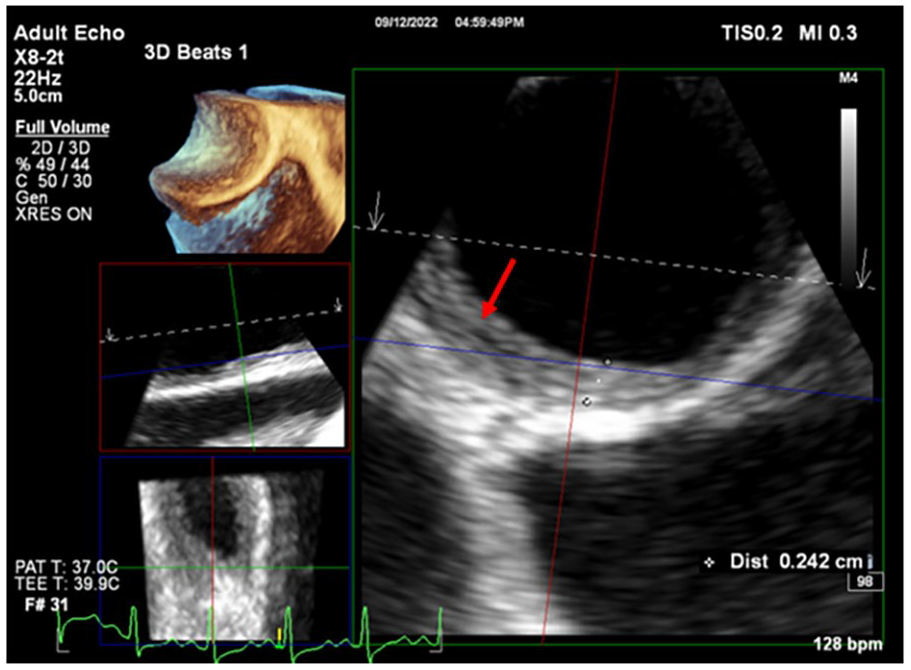
Transthoracic echocardiography images revealing diffuse symmetrical thickening of the walls of the aorta (red arrow).
Intravenous methylprednisolone 1 g/day was initiated, and anticoagulation was continued. Subsequently, the patient was started on tocilizumab and azathioprine, due to the severity of the disease, significantly elevated inflammatory markers, and multiorgan dysfunction. Methotrexate was avoided in the setting of acute renal failure.
Emergent CT angiogram of the chest, abdomen, and pelvis revealed an acute complete occlusion of the abdominal aorta at the level below the celiac artery, extending to the bilateral common iliac arteries, along with a left renal infarct (Figure 2). In addition, a complete occlusion of the left subclavian artery was noted, which likely caused a decreased flow to the left upper extremity. Given these findings, vascular surgery was consulted, and the patient was emergently taken to the operating room for aortoiliac thromboembolectomy. The surgery successfully debulked the clot burden, and the blood flow was restored in the superior mesenteric and iliac arteries. While his other rheumatological workup remained negative, the patient’s inflammatory markers were elevated. The diagnosis of TAK was established. Given that the patient had involved the entire aorta and its branches (including the ascending aorta, aortic arch, descending thoracic aorta, abdominal aorta, and renal arteries), he was classified as Type V. His Indian Takayasu’s Arteritis Activity Score 2010 was 17 points, indicating active TAK. 3

CT angiogram of the chest abdomen pelvis revealing an acute complete occlusion of the abdominal aorta at the level below the celiac artery (red arrow), extending to the bilateral common iliac arteries.
The patient demonstrated continued post-operative improvement, allowing for the transition from continuous renal replacement therapy to intermittent hemodialysis as his hemodynamic status stabilized. He was transferred out of the ICU shortly thereafter. Oral prednisone with a taper plan was continued along with azathioprine as a maintenance regimen and anticoagulation for arterial thrombosis. Tocilizumab was also added to his regimen instead of infliximab due to his lower ejection fraction, and infliximab was added 2 weeks later once his ejection fraction improved to 40% (instead of tocilizumab). He has since continued on azathioprine. Guideline-directed medical therapy for heart failure was initiated with dapagliflozin and carvedilol. His inflammatory markers normalized in subsequent follow-ups. Repeat TTE 18 months later showed a recovery in his ejection fraction to 54%.
Discussion
TAK is a form of large vessel vasculitis characterized by granulomatous inflammation of the involved territory, with major vessels such as the aorta and its branches, the pulmonary, and even the coronary arteries implicated. 4 The estimated prevalence of TAK in the United States is 8.4/million. 5 Young females of Asian descent make up the majority of patients affected by this disease. The exact pathophysiology of this condition remains unknown; however, pan-arteritis which is characterized by intimal hyperplasia, medial and adventitial thickening, and infiltration by mononuclear and giant cells, is thought to play a role in the development of the disease. 6
Presentation of TAK is variable and depends on the location of vessel involvement. Constitutional symptoms are typically present, such as fevers, fatigue, and weight loss. They can later progress to claudication of the extremities, weakness, hypertension, retinopathy, valvular dysfunction, or other neurological manifestations such as syncope or seizures. 6 Our male patient had presented with atypical symptoms that started with nonspecific back pains followed by a 1-day history of dyspnea on exertion and lower extremity swelling, leading to a diagnosis of heart failure. He lacked the typical constitutional symptoms highlighted above. Although the presentation of acute heart failure related to TAK is rare, it has previously been described in the literature. 7 Other differentials for acute cardiomyopathy should be explored, including viral myocarditis, cardiomyopathy related to substance use, genetic cardiomyopathy, or ischemic heart disease.
The American College of Rheumatology has established classification criteria for TAK. 4 These criteria are listed in Table 1. Three out of six criteria are required for diagnosis, and the presence of any three or more criteria yields a sensitivity of 90.5% and a specificity of 97.8% for diagnosis of TAK. Our patient met the criteria based on age, claudication of the extremities, systolic blood pressure difference in his arms, and arteriographic narrowing/occlusion of major vessels.
Diagnosis of Takayasu arteritis using the American College of Rheumatology 1990 criteria a .

The presence of three or more criteria is consistent with a diagnosis of Takayasu arteritis with sensitivity of 90.5% and specificity of 97.8%.
Once a diagnosis of TAK is made, treatment is initiated with high-dose glucocorticoids, typically 1mg/kg. Further immunosuppression with a steroid-sparing agent is often incorporated into the treatment regimen. 1 The American College of Rheumatology’s guidelines from 2021 recommend initial treatment at disease presentation with high-dose glucocorticoids and the addition of either methotrexate or azathioprine. 4 In more severe cases, or if patients are refractory to this regimen, a TNF inhibitor is recommended, with tocilizumab as an alternative in cases where TNF inhibitors are contraindicated. Due to his congestive heart failure, a TNF inhibitor was not utilized in our patient. If irreversible arterial stenosis develops, as in our case, surgical intervention may be warranted. Depending on the vessels involved and the patient’s anatomy, either endovascular or open-surgical approaches may be employed. The choice of approach is ultimately influenced by the surgeon’s expertise. Surgical options include angioplasties, grafting, and stent insertions. Major complications of surgical intervention in TAK are relatively rare, yet active disease at the time of surgery represents a major risk factor. Patients with active disease requiring surgery are more likely to require graft revision or develop progressive symptomatic disease at another site. 8
Immunosuppression should be slowly weaned over time with close surveillance and follow-up, as up to 50% of cases experience disease relapse, including acute aortic syndromes such as aortic dissection. Surveillance should be done with inflammatory biomarkers such as C-reactive protein and erythrocyte sedimentation rate and regularly scheduled advanced imaging with MR or CT angiography or positron emission tomography. 9
The majority of patients with TAK experience relapsing and remitting arteritis and require long-term immunosuppressive therapies. Vascular involvement tends to be progressive, although the short-term prognosis is favorable. In literature, a 5-year survival of 80%–90% has been reported. 8 Fields et al. 10 evaluated the outcomes of 42 patients with TAK who underwent surgical intervention. They discovered that only 43% of those who had active disease on steroids at the time of surgery were free from graft revision or disease progression at the 5- and 10-year follow-up. In contrast, 90% of those with inactive disease who were on steroids at the time of surgery were free from such complications.
In our patient, the extensive vascular involvement leading to lower extremity paralysis secondary to thoracolumbar vascular myelopathy necessitated emergent surgical intervention. While this may have increased the risk of disease relapse or progression, he is being closely monitored by multidisciplinary teams with appropriate imaging and laboratory evaluations.
Our case presented unique challenges in the diagnosis and surgical and medical management of TAK presenting with atypical and life-threatening features. The patient was successfully treated with high doses of glucocorticoids, azathioprine, and surgical intervention. He was ultimately maintained on infliximab and a gradual prednisone taper, yet remains at higher risk of relapse or progression of the disease. This distinctive presentation of TAK enhances our understanding of the diverse phenotypes of this condition and offers valuable insights for managing similar patients in the future.
Conclusion
TAK is a chronic form of large vessel vasculitis that primarily affects the aorta and its major branches. Our patient was diagnosed with TAK after being admitted due to acute cardiogenic shock. He was successfully transitioned to a treatment regimen consisting of oral prednisone, tocilizumab, and azathioprine, leading to an excellent recovery.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author contributions
Eiad Habib: conceptualization, writing – original draft; Laura MacPhee: conceptualization, writing – original draft; Fawad Aslam: methodology, supervision, writing – review and editing; Bhavesh Patel: methodology, supervision, writing – review and editing; Ayan Sen: supervision, writing – review and editing; Lisa LeMond: supervision, writing – review and editing; Ina Soh: writing – review and editing; Chelsea Marshall: writing – review and editing; Marie Grill: writing – review and editing; Kartik Mangipudi: writing – review and editing; Nolan McBride: writing – review and editing; Hiroshi Sekiguchi: methodology, supervision, writing – review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.