
Abstract
Multicystic dysplastic kidney is a congenital anomaly that can affect the kidneys. It is generally unilateral and is characterized by multiple noncommunicating cysts in the renal parenchyma. This disease usually results in an enlarged, nonfunctioning kidney in the neonate. Recent advances in diagnostic medical imaging, especially in sonography, have enabled earlier detection of this disease, created better management and treatment options, and resulted in improved outcomes for patients. This case study demonstrates the use of early detection with sonography and the utilization of it for follow-up care. Sonography is ranked as the imaging modality of choice for patients with a clinical condition of renal failure and has the potential for an improved outcome for patients.
Continued technological improvements in diagnostic imaging have a dramatic impact on the diagnosis, treatment, and management of many diseases. This is especially true in cases of multicystic dysplastic kidney where diagnostic medical sonography can identify the affected kidney(s) prenatally and can be used to track the progress of the disease postnatally. Multicystic dysplastic kidney is present in approximately 1 in 4000 neonates; early detection of the diseased kidney(s) enables planning for appropriate treatment and subsequent follow-up. In the past, management of this disease usually included a nephrectomy due to concerns over complications associated with hypertension and malignancy. However, many physicians are now taking a more conservative approach by leaving the diseased kidney in situ and monitoring with sonography given that most of these cysts eventually shrink.
Case Report
A woman, gravida 3, para 2, presented to the obstetric clinic for a routine 20-week gestation sonogram. Her first two pregnancies were carried to term, delivered vaginally, and were otherwise unremarkable. During the procedure, it was noted that the left kidney of the female fetus contained approximately six large, simple cysts. The left kidney measured 3.47 cm in length, nearly double the size of the right kidney, which measured 1.91 cm in length. The right kidney appeared sonographically to be normal (Figure 1). During the examination, the sonographer witnessed the fetus voiding by noting the bladder shrinking and refilling. The patient’s amniotic fluid index measured within normal limits. All other fetal measurements coincided with the date of the patient’s last menstrual period and the estimated gestational age of the fetus. The patient was then referred to a fetal internal medicine physician for follow-up prenatal care.
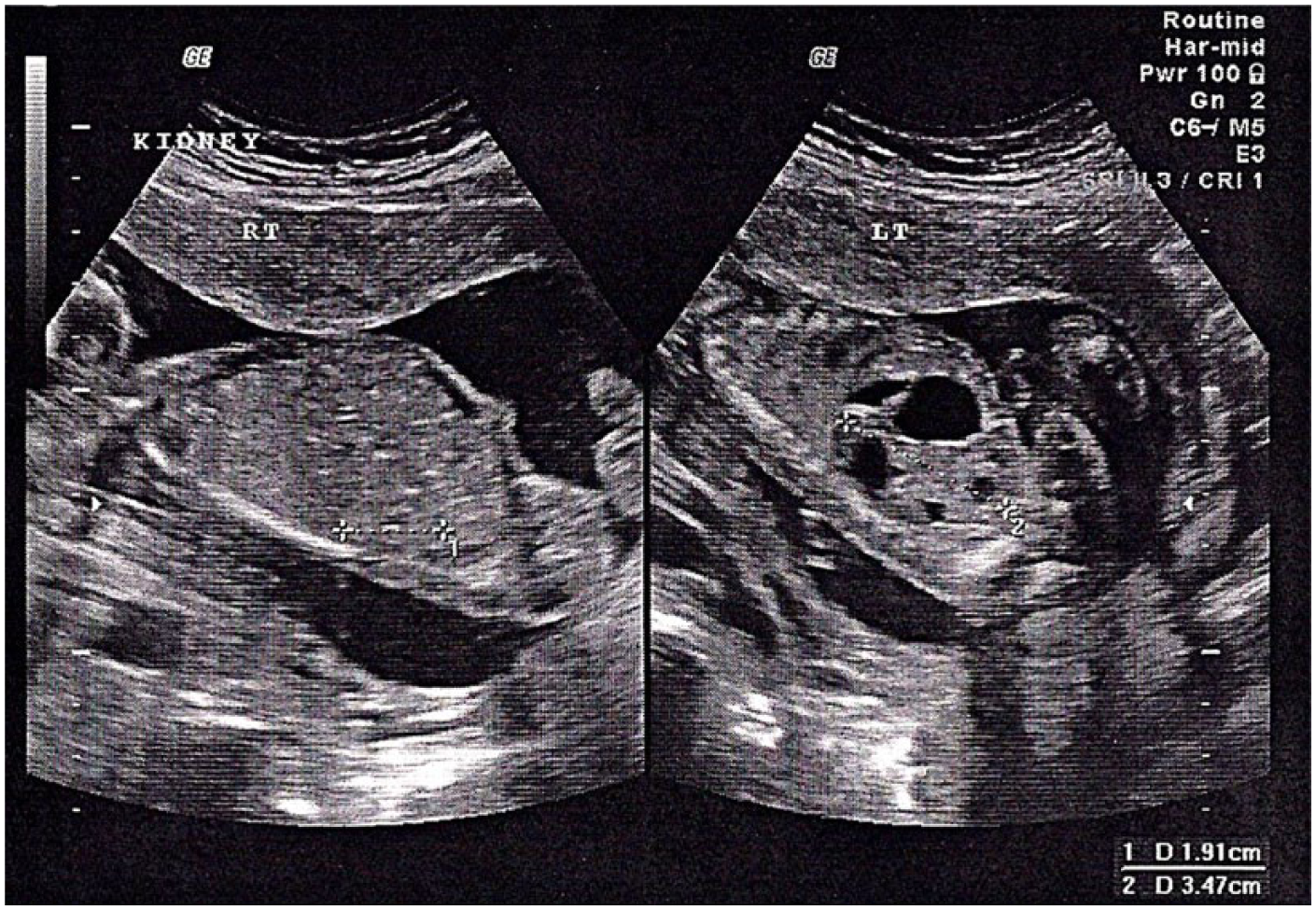
Longitudinal images of the right and left kidneys at 20 weeks’ gestation.
A second sonographic evaluation was performed at 27 weeks’ gestation. At this time, the fetus’ left kidney measured 5.66 cm in length and the right kidney measured 3.84 cm. The cysts were larger in size, with the largest measuring at 3.16 cm in diameter. Color Doppler imaging was used, but it was difficult to detect blood flow to the renal pelvis of the left kidney (Figure 2). In addition, the patient’s amniotic fluid was noted to be at the lower limit of normal.
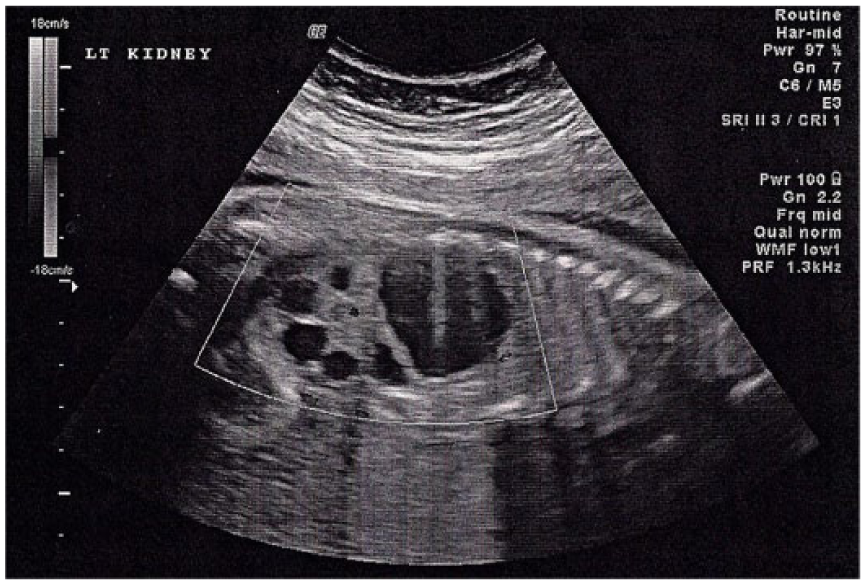
Longitudinal image of the left kidney demonstrating blood flow in the renal pelvis.
The third sonographic examination revealed that the left kidney was continuing to increase in size while the right kidney remained normal. Decreased amniotic fluid was also again documented.
During the fourth sonographic evaluation at 37 weeks’ gestation, the left kidney measured 8.25 cm in length (Figure 3), nearly the size of a normal adult kidney (9.0–12.0 cm). Minimal renal tissue was visible due to the multitude of noncommunicating cysts present; the largest cyst measured 3.88 cm in diameter. Figure 4 demonstrates a transverse view of both kidneys. At the time of this examination, the mother was also diagnosed with oligohydramnios.
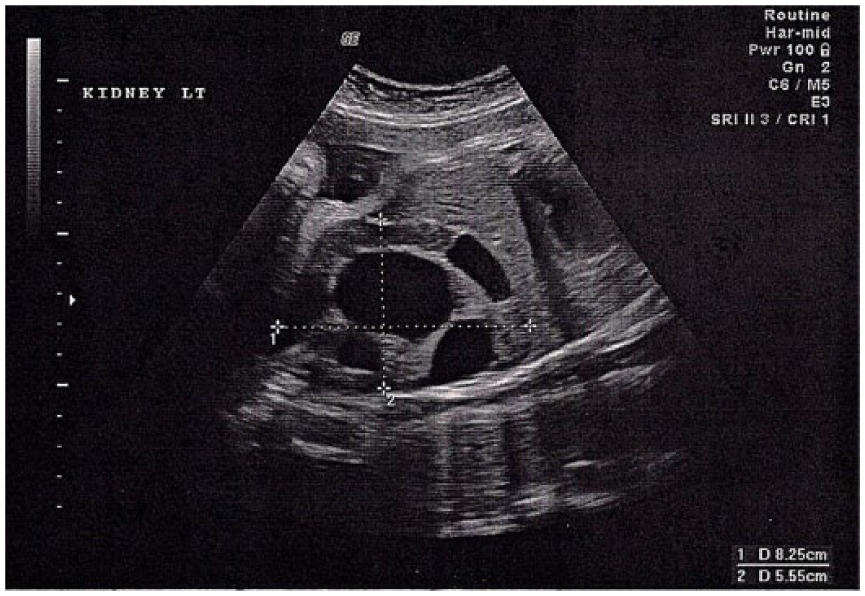
Longitudinal image of the left kidney at 37 weeks’ gestation.
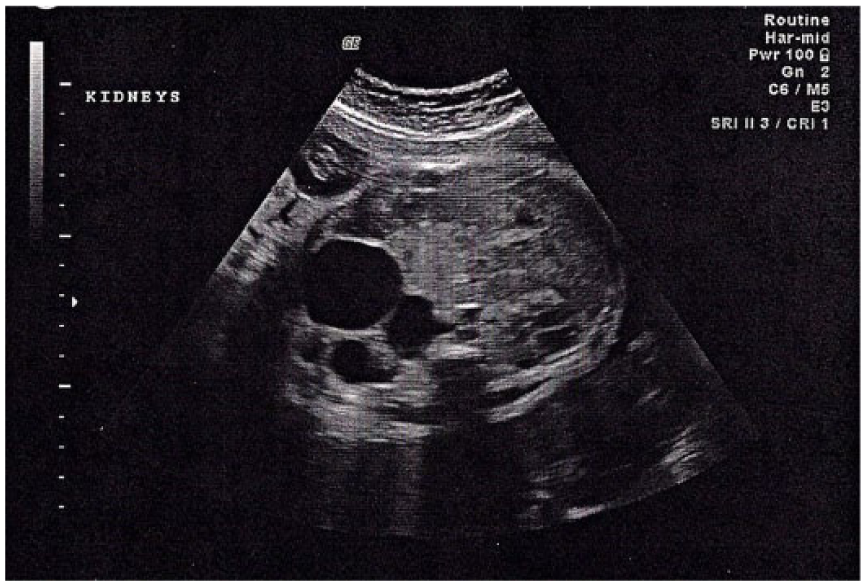
Transverse image of both kidneys at 37 weeks’ gestation.
The fetus was carried to term and delivered vaginally with no major complications; a postnatal physical examination revealed no evident physical masses on the newborn. The neonate’s kidneys were examined sonographically 24 hours after birth, and no obvious changes were noted in the left kidney. In addition, all renal laboratory function test results were within normal ranges.
At two months of age, the infant had another renal sonogram. The left kidney was slightly smaller than its maximum size in utero, and the larger cysts were slightly smaller in diameter. The infant underwent a voiding cystourethrogram (VCUG) procedure, which showed no signs of vesicourinary reflux. There was also no evidence radiographically of hydronephrosis. A targeted renal sonogram was scheduled for the patient at eight months of age, at which time the referring nephrologist anticipated that the left kidney would be smaller and the cysts would have continued to involute.
Discussion
Multicystic dysplastic kidney (MCDK) is a developmental anomaly of the kidney(s) that affects approximately 1 in 4000 live births and is the most frequent type of cystic renal disease in infants.1–4
There are two theories on the etiology of this disease. One hypothesis is that a blockage in the genitourinary tract causes a ballooning effect in the renal parenchyma as it matures and begins to form urine; the pools of fluid form multiple cysts in the kidney and normal, functional renal tissue does not develop. 1 Another hypothesis regarding MCDK is that the mesoderm of the embryo fails to differentiate into nephrogenic epithelium due to a signal processing error in development. 2 Regardless of which theory is more accurate, the multicystic kidney has little to no physiologic function.1,2
Multicystic dysplastic kidney is separate from other cystic renal abnormalities in that it does not seem to be a familial disorder. 5 MCDK is not believed to be caused by any specific type of teratogen, although some of the literature reviewed would suggest otherwise. 6 However, one report does note an increased incidence of MCDK and other fetal anomalies in mothers with preexisting diabetes mellitus. 7 MCDK is thought to be a spontaneous occurrence related to genetic mutations. 6 Most often, the left kidney is affected, and it is more common unilaterally in males.2,3 Bilateral MCDK is not compatible with life.
Prior to recent advancements in sonographic imaging, MCDK generally went undetected unless a palpable mass was noted at birth or was seen as a lump on a small child.1–3 Unilateral MCDK is usually asymptomatic and has been found in older patients secondary to exploratory examinations, for other causes. On occasion, adult patients have undergone an abdominal sonogram and have been found to have unilateral renal agenesis. 4 The possibility exists that the atrophic kidney is the result of MCDK, but little scientific research on this possibility has been completed at this time.
It is important when diagnosing MCDK to determine that the cysts are noncommunicating and that they are located in the renal cortex rather than in the renal pelvis.1,2,4 This helps rule out the possibility of severe hydronephrosis, which is more clinically significant than a nonfunctioning kidney with multiple cysts.5,8 If unilateral multicystic dysplastic kidney is diagnosed in utero, the usual course of action is to follow up with sonography, until the fetus is born. A common occurrence with unilateral MCDK in utero is that the cysts will increase in size until near term and then the cysts will spontaneously involute after birth. 2 The remaining renal tissue will gradually atrophy and may appear as renal agenesis later in life.
In the past, physicians chose to perform an immediate nephrectomy on the multicystic kidney due to concerns related to the development of systemic hypertension or malignancy in the affected kidney.1,3 Today the preferred medical practice is to leave the multicystic kidney in situ as long as it does not cause any major complications to the patient.4,5
Due to the nature of the obstructive process of MCDK, other genitourinary complications may accompany the disorder. Vesicoureteral reflux (VUR) in the contralateral kidney is the most common associated anomaly in patients with MCDK.3,4 Vesicoureteral reflux and the resulting urinary tract infections can cause renal damage and possibly renal failure of the only functional kidney.6,8,9
Although sonography is the preferred imaging modality for MCDK, other types of imaging and physiological testing are usually performed due to other health issues linked to MCDK. The American College of Radiology (ACR) ranks the appropriateness of certain imaging tests for chronic renal failure, and sonography is ranked as the most appropriate. 10
An alternate imaging examination that can be performed on patients with MCDK postnatally is the voiding cystourethrogram, a specialized radiographic procedure that evaluates for VUR.8,9 This test involves placing a catheter into the patient’s bladder and filling the bladder with a contrast medium. The catheter is then removed, and a series of fluoroscopic images are taken of the bladder, kidneys, and ureters as the patient’s bladder is emptied. If any reflux of urine occurs during the examination, then the fluoroscopic images document the areas involved and the severity. Another test that can evaluate possible reflux is performed in the nuclear medicine department. Although typically lower ranked by the ACR, the dimercaptosuccinic acid scan uses radioactive tracers to evaluate the kidneys for size, function, and scarring related to reflux of urine from the bladder.8,9 Magnetic resonance urography can be used to determine the presence of VUR in the presence of MCDK while also evaluating the structure and the function of the unaffected kidney. 9
The prognosis for patients with MCDK is very good since most of the affected kidneys will eventually become smaller as the cysts gradually involute.2,4 Follow-up management for patients with MCDK involves having at least annual renal sonograms (with renal Doppler) of the functioning kidney. In addition, blood pressure and urinary function are also monitored regularly. If hypertension becomes a concern for the patient, then a nephrectomy may be indicated since the multicystic kidney may be the cause. In most cases, the patient’s blood pressure will return to normal levels following the removal of the dysplastic kidney. 11 Segmental resection of the kidney deemed to be multicystic and dysplastic is rarely needed. 12
Summary
It is important to properly diagnose a multicystic dysplastic kidney since early detection of this disorder, along with improved medical management, enables patients with MCDK to have relatively healthy outcomes. Sonography plays a vital role in the diagnosis of MCDK and also provides important diagnostic information for the follow-up care of these patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.