
Abstract
Multicystic dysplastic kidney (MCDK) is a common nonhereditary cystic dysplasia that can be detected antenatally. This disorder commonly manifests in utero and presents unilaterally; however, this patient’s case demonstrates bilateral MCDKs. The use of sonography is essential in diagnosing this disorder both antenatally and following birth. Bilateral MCDKs present as large anechoic cysts overtaking renal parenchyma and halting all normal renal physiologic functions. This case study demonstrates the importance of early detection, the progression of this disorder, as well as the large part sonographic imaging plays in visualizing the MCDK.
The most common cystic dysplasia diagnosed antenatally is the multicystic dysplastic kidney (MCDK). There are dysplastic changes that begin within the affected kidney, ultimately ending normal and essential renal functions. While MCDK can present as unilateral or bilateral, the bilateral presentation happens in less than 1 in 10 000. 1 Whether unilateral or bilateral, recognizing this pathology is essential to the diagnosis and identification of associated anomalies. Early detection can assist in intervention procedures such as termination of the pregnancy with bilateral MCDK, due to the disorder, being incompatible with life.
Case Report
A 24-year-old pregnant female received prenatal care, beginning at 28 weeks gestation. Sonography showed a series of anomalies within the male fetus, including bilateral MCDKs, abdominal ascites, anhydramnios, pulmonary hypoplasia, small thorax, and the absence of kidney function. The patient was admitted to the hospital for a needle aspiration of fetal ascites during which they removed 300 cc of fetal fluid. Following the aspiration, the umbilical cord drug screen tested positive for morphine, likely due to narcotic exposure, during the procedure. Approximately 5 hours following the procedure, the infant was born via vaginal delivery at 31 weeks and 6 days gestational age.
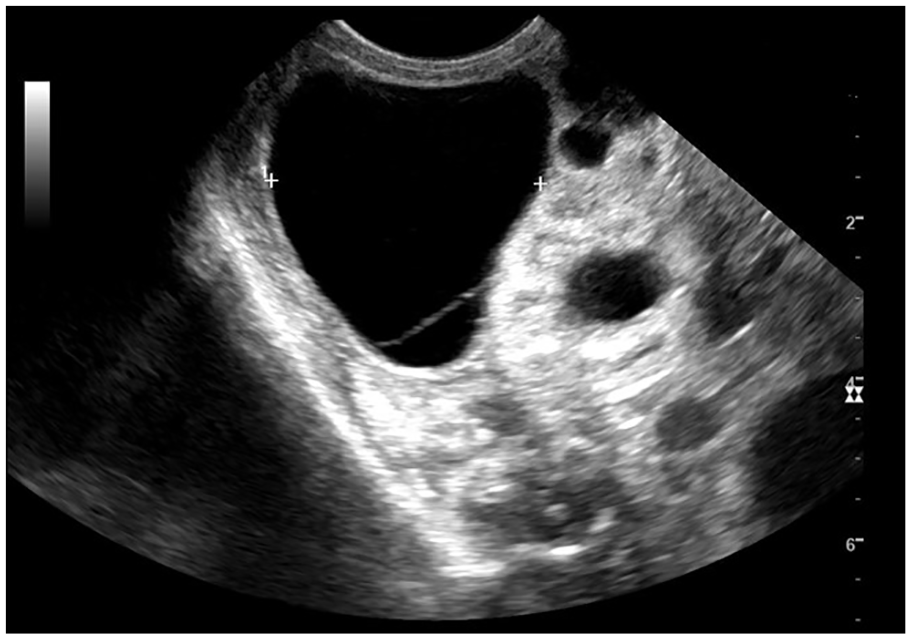
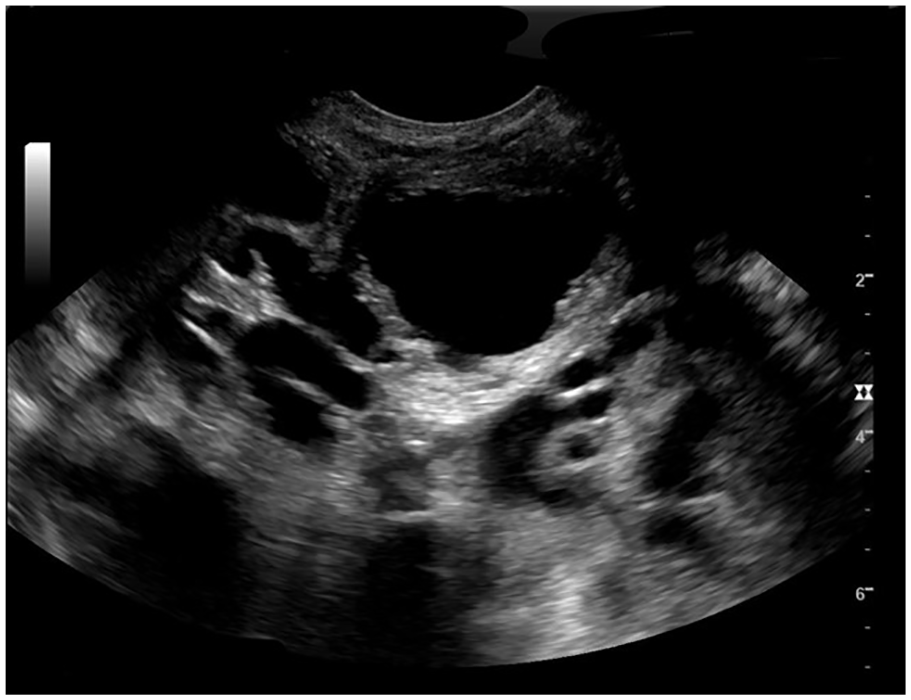
The infant was admitted to the neonatal intensive care unit (NICU), presenting with a severely distended abdomen due to bilateral MCDKs and ascites. The sonographic findings showed large anechoic cysts overtaking the renal parenchyma (see Figures 1 and 2). The renal cysts were bilateral, round, and anechoic. The cysts ranged in size, the largest bilateral cysts presented with septations within them, and it was difficult to visualize the connecting points of the large cysts (see Figure 3). The sonogram was unable to demonstrate whether the cysts were part of the kidney or stemming from surrounding organs. The sonogram did indicate signs of hydronephrosis and caliectasis, through the abnormal fluid collections, within the kidneys. In addition, a pair of tortuous ureters was seen posterior to the bladder (see Figure 4).

Longitudinal gray-scale sonogram of the right kidney showing multiple cystic regions overcoming the normal renal parenchyma.

Longitudinal gray-scale sonogram of the left kidney showing multiple smaller cystic regions within the renal parenchyma. The caliper placement measured a renal length of 5.36 cm.
Transverse gray-scale sonogram of the right upper quadrant demonstrating a large fluid collection with internal septations. The caliper placement measured a fluid collection at 3.34 cm.
Transverse gray-scale sonogram of the bladder demonstrating bilateral tortuous ureters inferior to the bladder.
Another sonogram was conducted to assess the fluid collections, within the four abdominal quadrants. Large collections of ascites were present in all four quadrants (see Figure 5A and B). Following the abdominal sonogram, physicians opted to remove 20 mL of serosanguineous fluid, consisting of both blood and fluid, from the abdominal quadrants. On a follow-up sonogram, ascites appeared to be lessened yet still present alongside a distended abdomen. A series of chest radiographs were conducted, which allowed for visualization of an enlarged heart, small bilateral pleural fluid, and pulmonary edema. Accompanying these findings, the infant initially presented with a right-sided pneumothorax, which was treated with a needle aspiration and catheter placement. Throughout the following days of the infant’s NICU stay, there were recurring right pneumothorax and left pneumothorax, which were treated with the placement of a chest tube.
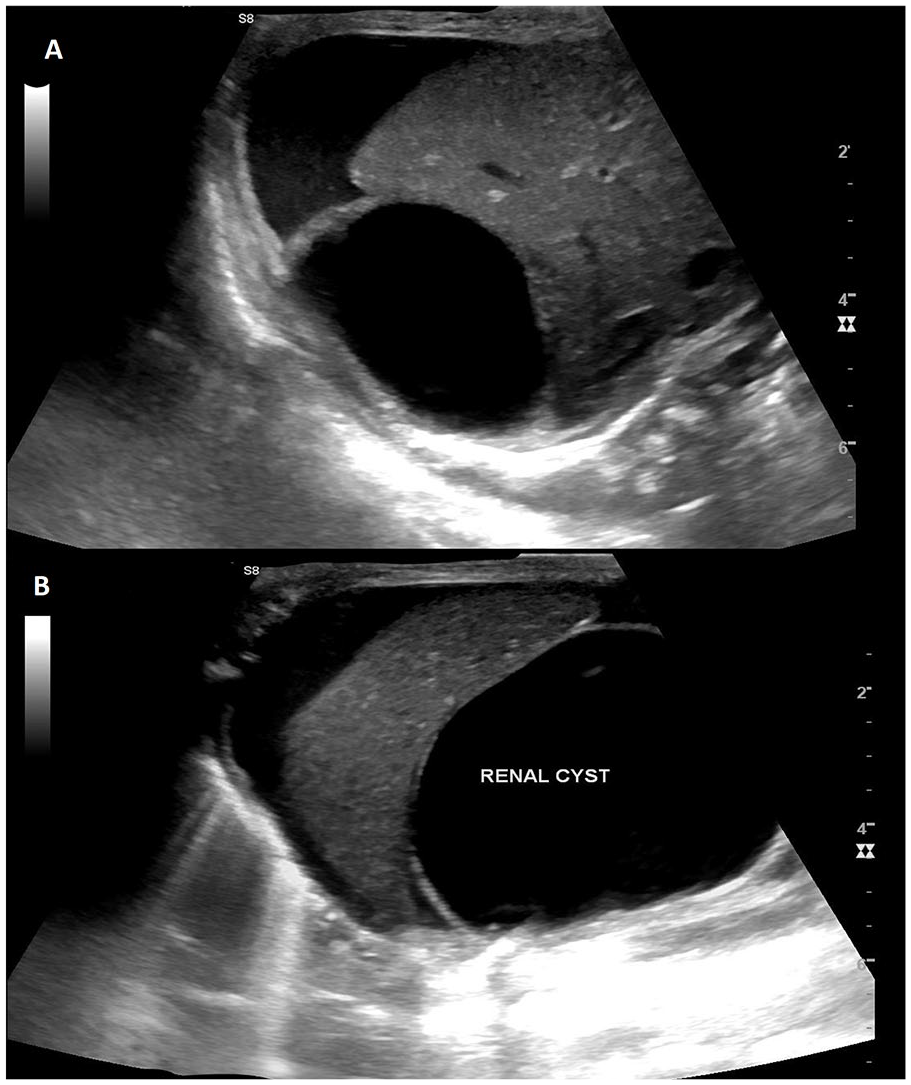
(A) Transverse sonogram of the right upper quadrant fluid collection surrounding the superior aspect of the liver and renal cyst sitting inferior to the liver, and (B) longitudinal sonogram of the right upper quadrant with ascites surrounding the liver and a large anechoic renal cyst, located just inferior to the liver.
After the radiographs were completed, an echocardiogram was used to assess the infant’s cardiac structure and function. Often times, MCDKs are associated with extrarenal anomalies, including a wide variety of cardiac anomalies. 2 Prenatal and postnatal echocardiograms can be useful with an infant presenting with MCDKs, which allows for a proper assessment of cardiac function and possible anomalies. In the present case, the echocardiogram revealed the infant had severely depressed right ventricular systolic function, pulmonary regurgitation, small right to left atrial shunt, moderate tricuspid regurgitation, and a flattened interventricular septum. Following both the echocardiogram and radiographs, the infant was deemed unfit to be put on dialysis due to poor heart function and respiratory failure. At 11 days, the infant died due to cardiopulmonary failure, as a result of a pulmonary hypoplasia, stemming from the MCDKs.
The infant’s autopsy report confirmed the diagnosis of severe bilateral MCDKs. Contributing factors to the infant’s death include prematurity, bladder outlet obstruction, and pulmonary hypoplasia, further complicated by pulmonary hypertension. It was also discovered that the infant had posterior urethral valves ultimately causing severe hydronephrosis, dilated ureters, and bladder outlet obstruction. Genetic testing was completed following the death of the infant, which showed no evidence of genetic abnormalities. There can be an increased incidence of accompanying chromosomal abnormalities with the bilateral MCDK as opposed to unilateral MCDK. 2
Discussion
A functioning renal system is essential to maintain homeostasis via filtration of blood, removal of metabolic waste products, and the production and excretion of urine. 3 The developing kidney goes through three developmental stages ending in the permanent kidney. The urinary system in a fetus develops from the mesodermal tissue and by the third month of gestation will begin to function through excretion of urine into the amniotic fluid. 3 Instead of the smooth hypoechoic renal parenchyma, this infant presented with echogenic, irregular renal tissue. Unlike a normal renal system, the case study infant did not demonstrate hypoechoic renal pyramids, due to multiple noncommunicating cysts overtaking normal renal parenchyma. 4 Antenatally, MCDK is thought to occur due to abnormal interactions or development of the ureteric bud and the metanephros. 5
MCDK is characterized as multiple noncommunicating cysts, which are separated by nonidentifiable and dysplastic renal parenchyma. 4 Unilateral dysplastic kidney occurs in around 1 in 3000 to 5000 fetuses, whereas bilateral occurs in 1 in 10 000 fetuses. 1 Bilateral MCDKs is the less common form of the disease, it is considered incompatible with life due to the lack of functioning renal tissue and associated anomalies with the disease. This disorder can be visualized antenatally via sonography, and it is often the first diagnostic method when evaluating MCDKs. In some cases, magnetic resonance imaging (MRI) can add additional information regarding associated anomalies, including oligohydramnios, unusual location and appearance of cysts, or malformations of other organs. 5
Prenatal sonography can detect MCDKs; however, it can be easily mistaken for multiple other renal anomalies. The differential diagnoses include hydronephrosis, obstructive renal dysplasia, urinary tract obstruction, or other variations of renal cystic disease. 6 Misdiagnosis of MCDKs is most commonly a result of the similar sonographic appearance of hydronephrosis. Sonographically, MCDKs can be described as varying degrees of cysts, throughout the kidney, without normal renal shape or internal structures. Hydronephrosis will appear differently; often there will be a dilated renal pelvis and collecting system. Likewise, a hydronephrotic kidney can oftentimes lose visualization of renal parenchyma. As hydronephrosis progresses and becomes more severe, distinguishing these two anomalies will become increasingly similar as fluid begins to overtake the entire kidney. 7 It is essential to distinguish these renal anomalies from each other due to the differing nature of treatment and follow-up procedures. MCDKs will take on a more conservative approach to treatment options as surgical intervention is not often recommended, whereas hydronephrosis will need operative treatments to correct for obstructions. 7
Progression of the disease advances as the cysts enlarge and more cysts develop within the hilum. Prognosis almost depends solely on the advancement of the disease, bilateral or unilateral, and other anomalies. Bilateral MCDK disease is incompatible with life; typically the mother will elect to terminate the pregnancy. This decision is usually based on the lethal nature of the anomaly or the fetus will die shortly after birth. 4 Infant survival is extremely uncommon as a result of the multiple complications that stem from this disorder, such as pulmonary hypoplasia resulting from lack of amniotic fluid. A case study has been reported of an infant presenting with bilateral MCDKs and survived the prenatal period. 8 Unfortunately, upon birth the infant was immediately placed on dialysis and remained on dialysis until a renal transplant and bilateral nephrectomy was performed. 8
Sonographically, the kidneys will appear with multiple cysts of differentiating sizes; the patient will most likely present with enlarged kidneys and abdominal circumference. It is difficult to define renal borders due to the parenchyma being taken over by cysts. The cysts appear as multiple large anechoic cysts, all of differing sizes. The parenchyma will have an increased echogenicity as a result of connective tissue proliferation. 9 If the disease is unilateral, the contralateral kidney will present enlarged and there will be no oligohydramnios allowing for proper lung development. With bilateral presentation, the fetus will present with oligohydramnios or anhydramnios and pulmonary hypoplasia, which occurs as a result of low levels of amniotic fluid. Sonography is the most reliable way to diagnose MCDKs, and MRI can become an asset when determining more specific aspects of the disorder and accompanying anomalies. 10
Conclusion
When sonography is utilized in prenatal care, sonographers may visualize enlarged and cyst filled kidneys around 18 to 20 weeks gestational age. Sonography is often the first method in diagnosing MCDKs; it allows for a deeper understanding of how the disorder affects other systems. In this case, prenatal sonographic screening allowed for visualization of the multiple life-threatening anomalies the fetus suffered from, allowing for interventional procedures to occur in an attempt to improve chances of survival. Despite the inability of the fetus to survive the countless medical blockages, sonography was able to provide medical professionals with a deeper knowledge of the events leading up to death.
Footnotes
Acknowledgements
The authors thank Heidi Heser, RDMS; Tracy Heinz, RDMS; and Hailey Bertani, RDMS, RVT for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.