
Abstract
Caudal regression syndrome (CRS), also known as caudal dysplasia syndrome, is a rare malformation that ranges from mild coccygeal to severe forms of lumbosacral and lower thoracic agenesis. Anomalies of other organ systems may also be found simultaneously. Recognition of CRS is important as the extent of abnormality and gestational age could determine the pregnancy’s outcome. Antenatal diagnosis is possible by recognizing the characteristic features on sonography. In this particular case study, a diagnosis of CRS was made during the second trimester with sonography and resulted in an adequate medical management decision. The sonographic features of CRS and its differential diagnoses are discussed in the context of this case study.
Introduction
Caudal regression syndrome (CRS) was first described by Geoffroy Saint-Hilaire and Hohl in 1852. This multiple malformation syndrome is a rare congenital anomaly of unknown etiology with a reported incidence varying from 1 to 2.5 per 100 000 normal pregnancies 1 and has a 200- to 400-fold increased risk in diabetic mothers with reported incidence of up to 1% of pregnancies.1–3 Vascular hypoperfusion and genetic predisposition have been identified as the causative factors besides periconceptional hyperglycemia. The vertebral anomaly may range from simple coccygeal agenesis without any neurological deficit to complete lumbosacral agenesis with severe neurological compromise of the bladder, bowel, and lower extremities. 4 Other anomalies of the musculoskeletal, genitourinary, gastrointestinal, and cardiovascular systems may also be found simultaneously. An interpreting physician’s responsibility is to suspect CRS, document it early in the antenatal period as opposed to similar malformations, and determine its severity and associated anomalies in order to present options for the patient. A case study is presented that demonstrates the detection of CRS on a routine antenatal sonogram, at 19 weeks of gestation. An adequate amount of amniotic fluid permitting optimal evaluation and a systematic scrutiny of the fetus helped in making a confident antenatal diagnosis based on the sonogram. The patient chose to terminate the pregnancy and radiographs confirmed the antenatal findings.
A 24-year-old woman with 19 weeks of amenorrhea visited the hospital for a routine obstetrical checkup. She had one living child and her obstetric history was insignificant, but she was at risk of diabetes. Her routine blood investigation revealed hyperglycemia, with fasting and postprandial sugar levels of 120 mg/dl and 174 mg/dl, respectively. The glycosylated hemoglobin (HbA1c, normal range being less than 6%) levels were 11%, suggesting poor blood glucose control. Sonography revealed a singleton intrauterine live fetus corresponding to 19 weeks. The spine terminated abruptly at the upper lumbar region (Figure 1A). The pelvis revealed fused midline iliac bones (Figure 1B). Both lower limbs demonstrated normal-size femurs and two bones in each leg. However, there was mild thinning of soft tissues of the legs and they were conspicuously immobile (Figure 1C). Bilateral feet showed a clubbed deformity. The fetal cranial, abdominal, and cardiac organ evaluations showed no remarkable findings. The umbilical cord was normal. A confident sonographic diagnosis of CRS was made due to the presence of adequate amniotic fluid. The prognosis of the fetus was explained to the mother and she opted for termination of pregnancy, which was done after control of her high blood sugar levels. Sonographic findings were confirmed on gross clinical (Figure 1D) and radiologic examination of the abortus. The abortus revealed a narrow lower abdominal and pelvic region with a shallow gluteal cleft but a normal anal pit. Due to the presence of soft tissue contractures, the lower limbs were placed in a characteristic fixed position of flexion and abduction at the hip and flexion at the knees. Radiographs of the abortus showed the spine up to mid lumbar (L3) level and absence of distal lumbar, sacrum, and coccyx. Consequently, the iliac blades fused in midline. Thirteen pairs of ribs were radiographically apparent (Figure 1E). Having 13 pairs of ribs is an association with CRS that has not been reported previously.
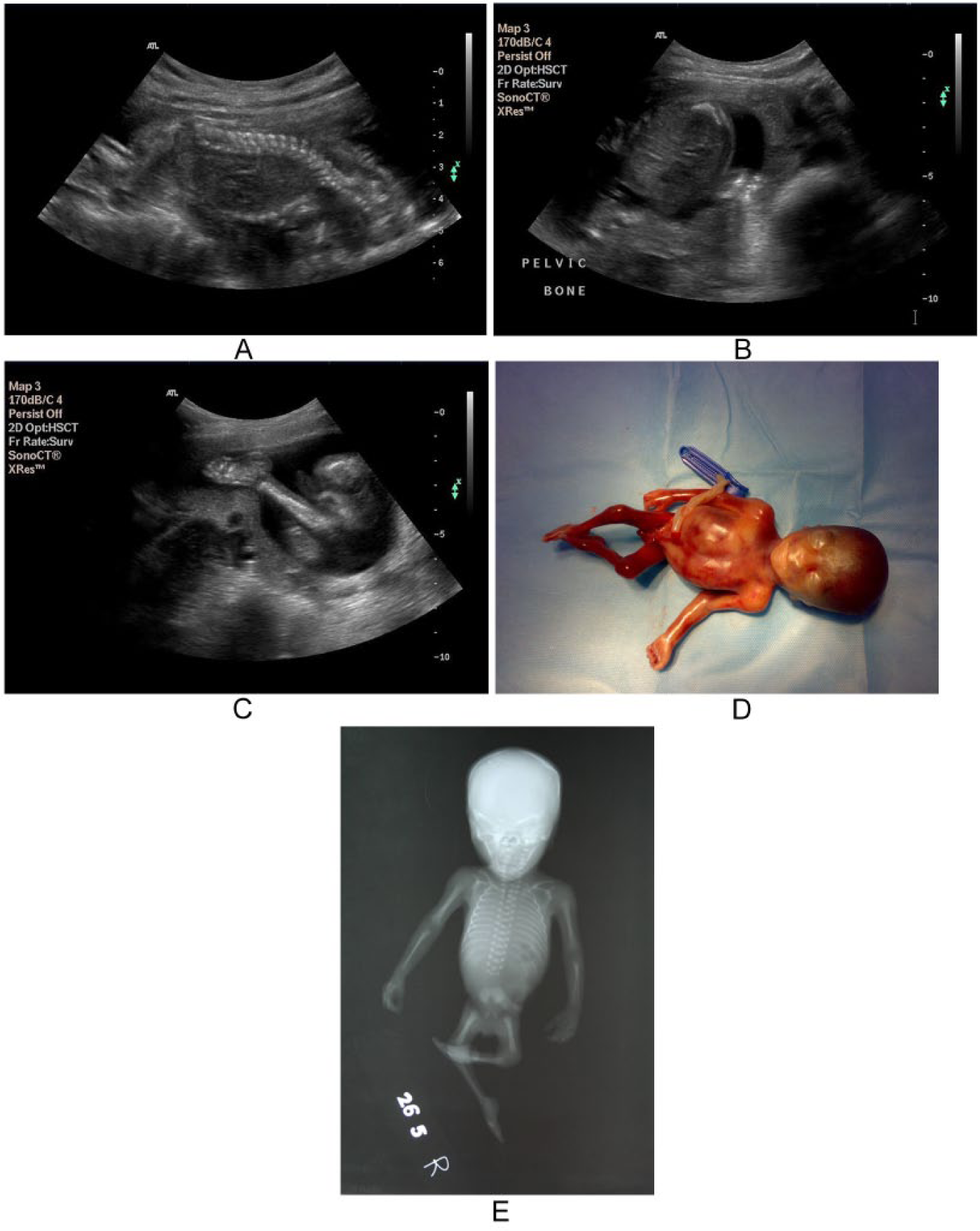
(A) Antenatal sonographic image in sagittal plane shows the spine ending abruptly at the lumbar level (arrow). (B) The iliac bones are hypoplastic and seem to be fused in the midline (arrow). (C) One of the lower limbs shows normally appearing tibia and fibula with thinning of soft tissue (arrow), and club foot is also suspected. (D) Clinical photograph of the abortus. Lower abdomen and pelvic region are hypoplastic (white arrow) and lower limbs (black arrow) are seen in a frog-like position with club feet. (E) Postabortal radiograph showing absence of lower lumbar vertebrae (L4 and L5), sacrum, and coccyx (arrow). The iliac bones are fused. Bilateral lower limbs are hypoplastic and flexed at hip and knee with club feet. Thirteen pairs of ribs are also noted.
Discussion
Caudal regression syndrome results from abnormal fetal development of the lower spine due to defective neuralization of mid posterior axial mesoderm around 4 weeks of fetal development.
Caudal regression syndrome manifests as anomalies of the distal vertebral spine, anorectal, and genitourinary regions and musculoskeletal abnormalities of the lower limbs. 5 However, there is sparing of the brain, spinal cord, and proximal spine, as was also apparent in this case. Antenatal diagnosis of CRS aims at determining the extent and severity of caudal dysgenesis and in detecting the associated abnormalities of other organ systems. A detailed morphologic assessment of the fetus is essential to differentiate CRS from closely mimicking conditions having a more dismal prognosis, to guide appropriate patient management. The diagnosis of CRS is often made late in gestation, usually beyond 20 to 22 weeks. 6
Sonography is adequate for antenatal diagnosis in the presence of a normal amount of amniotic fluid. Associated renal abnormalities may be responsible for a decreased amount of amniotic fluid; however, this could result in the need to inject fluid into the amniotic sac (amnioinfusion) and for magnetic resonance imaging to delineate the fetal anatomy. 7 In this case, adequate amniotic fluid and recognition of the characteristic findings made detection of the abnormality possible at 19 weeks. It also gave the patient an option to elect for a safe termination of the pregnancy. Early detection of CRS, at 11 weeks of gestation, has been previously reported in the literature. 8 In the first trimester, a short crown-rump length is the only finding on transabdominal sonography, which if present warrants a transvaginal approach to reveal the absence of distal spine. Later in the gestation, a complete or partial agenesis of the sacrum and lumbar vertebrae associated with hypoplastic, fused iliac blades in the midline gives a shield-like appearance. Both lower limbs are identified but are often hypoplastic and fixed. Flexion contractures at the hip and knee joints result in a characteristic frog-like appearance of the lower limbs, also referred to as a “Buddha’s pose.” 9 These findings are characteristic of CRS.
Differentiating CRS from other similar types of anomalies with poor prognoses, such as limb body wall complex, neural tube defects, and sirenomelia, is very important. In the first trimester, limb body wall complex with associated caudal deficiency can be identified with the presence of abdominal and/or thoracic wall defects with absent or deformed lower limbs and marked scoliosis. Neural tube defect, also a common occurrence in maternal diabetes, shows vertebral column defects in the form of kyphosis, splaying of the posterior spinal elements with or without a back mass, and associated spinal cord and central nervous system anomalies. A neural tube defect can be excluded by displaying normal subtle curvature of the spine in the longitudinal view, convergence of the vertebral lamina on axial fetal scanning, and presence of a normal cranial sonogram.
Polyhydramnios, seen as an increased amount of fluid in the amniotic sac (Amniotic Fluid Index [AFI] > 18 cm), is a frequent finding with neural tube defects, whereas a normal amount of amniotic fluid can be present in cases of CRS. Sirenomelia, another condition exhibiting severe caudal dysgenesis, is incompatible with life due to accompanying renal agenesis/dysgenesis and associated pulmonary hypoplasia. In sirenomelia, the fetus resembles a mermaid and is diagnosed on the basis of single/fused lower limbs with fewer long bones than normal (three or fewer). A decreased amount of amniotic fluid (AFI < 5 cm) or oligohydramnios is commonly encountered in sirenomelia due to renal agenesis; however, it is considered a rare finding in CRS. Unlike in CRS, a single umbilical artery has been observed in sirenomelia cases. Unlike neural tube defect or sirenomelia, the amount of amniotic fluid is usually normal except when associated with a urinary system abnormality, which may require magnetic resonance imaging due to oligohydramnios. Once the diagnosis of CRS is made and the extent of the abnormality is determined, it is important to determine other associated abnormalities. Caudal regression syndrome may be associated with abnormalities such as pulmonary hypoplasia, congenital cardiovascular anomalies, anal or esophageal atresia, severe orthopedic deformities of the lower limb, and hypoplasia with contractures, which have been noted in severe cases.
Despite an extensive literature search, an association of CRS with 13 pairs of ribs was not located, making this case unique. Another reported case of CRS involving sacrococcygeal segments had a sacral rib. 10 Other musculoskeletal associations described in the literature are kyphoscoliosis, an outward and lateral spinal curvature abnormality, and absent ribs. Various spinal anomalies like longitudinal splitting of the spinal cord, as in diastematomyelia, and posterior vertebral defects with spinal cord containing back mass, as in myelomeningocele, are rare manifestations. Severe defects and multisystem involvement in CRS have a poor prognosis, and early diagnosis in such cases can offer the patient the option for a safe and less traumatic termination of the pregnancy. Antenatal documentation of the extent of CRS can help in counseling the parents regarding termination of pregnancy in severe cases. Surviving infants with a lesser degree of involvement can have normal cognition. However, bladder and bowel dysfunction and disability due to neuromuscular deficits of the lower extremities can lead to significant morbidity. Postnatal interventions can be planned for the associated anomalies in less severe cases. However, such infants require medical assistance in the form of corrective surgical intervention, treatment for urological problems, and supportive orthopedic care throughout life. 11
Conclusion
A well-performed sonographic examination around the mid trimester can define the extent of caudal dysplasia that may exist by demonstrating the vertebral column and lower limbs as well as screening for other associated fetal defects. Sonography may also differentiate CRS from other similar-appearing but more serious conditions like limb body wall complex, neural tube defects, and sirenomelia. Recognition of characteristic findings can provide a confident and early antenatal diagnosis, aiding in appropriate medical management decisions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.