
Abstract
Sirenomelia is an uncommon complex congenital anomaly associated with fusion of the lower limbs and abnormalities of the urinary and gastrointestinal tract. Most cases of sirenomelia are not diagnosed in utero due to the complexity of the anomalies coupled with anhydramnios. With a male predominance of approximately 3:1, amniocentesis or noninvasive prenatal screening is the only way to confirm the chromosomes and gender of fetuses diagnosed with sirenomelia in utero. Few cases have been reported surviving past the neonatal period and a majority die in utero.
Introduction
Sirenomelia, or “mermaid syndrome,” is a multifaceted and rare anomaly usually diagnosed after birth. It can be difficult to diagnose prenatally, but any time severe oligohydramnios or anhydramnios is identified, especially with renal anomalies or renal agenesis, and there is an inability to distinguish distinct lower extremities, sirenomelia should be considered. Historically, sirenomelia was considered to be the most severe form of caudal regression syndrome, although recent research has shown differences between the two disorders. These subtle differences have encouraged some researchers to discuss the possibility of sirenomelia and caudal regression syndrome being two separate anomalies with overlapping characteristics. The use of sonography and magnetic resonance imaging (MRI) can aid in the diagnosis prenatally and assist in the postnatal treatment and care of the affected fetus.
Case Study
A young female, gravida 1 para 0, was referred to a high-risk pregnancy center for a detailed anatomic survey at 23 weeks of gestation due to the concern for multiple congenital anomalies. Outside pregnancy records mention an early sonogram suggesting a twin gestation, and two subsequent sonograms demonstrated a singleton pregnancy as well as concern for the threat of abortion. The outside 19-week sonogram identified bilateral hydrocephalus, an abnormal cerebellum with lemon-shaped head causing concern for Chiari II malformation, bilateral multicystic dysplastic kidneys, and pericardial effusion. The sonography report noted that the fetal stomach was identified, but they were unable to visualize a urinary bladder. Cord vessels were noted to be difficult to completely image. The combination of breech presentation and anhydramnios restricted the evaluation of anatomy. The patient had not initiated prenatal care until 16 weeks, so genetic screening had not been requested at that time.
The examination was performed on a GE Voluson E8 using a C1-5-D curvilinear transducer and RM6C 3D transducer. Sonographic findings included dolichocephaly with bilateral ventriculomegaly (Figure 1) and a hypoplastic cerebellum, single umbilical artery (Figure 2), multiple cysts on both kidneys (Figure 3), short upper extremities, and a single femur bone (Figure 4). Hands and feet were not visualized. The fetal stomach and bladder were not identified. Lower spine was not well visualized due to breech presentation. The examination was limited by anhydramnios and breech presentation. The patient was counseled regarding the poor prognosis and declined the option for termination.
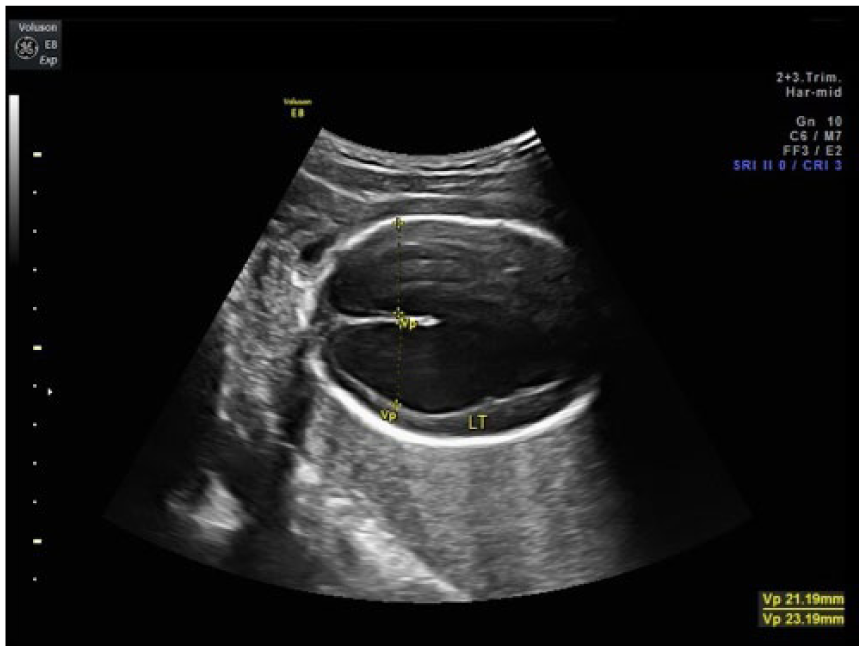
Bilateral ventriculomegaly at 23 weeks gestation.
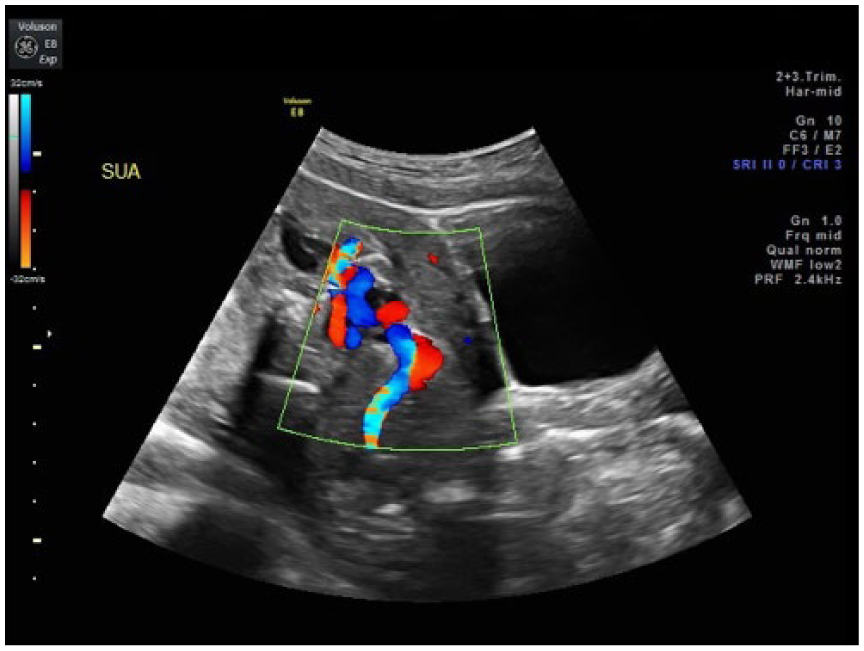
Color Doppler demonstrating a single umbilical artery at 23 weeks gestation. Maternal bladder is seen to the right of the image.
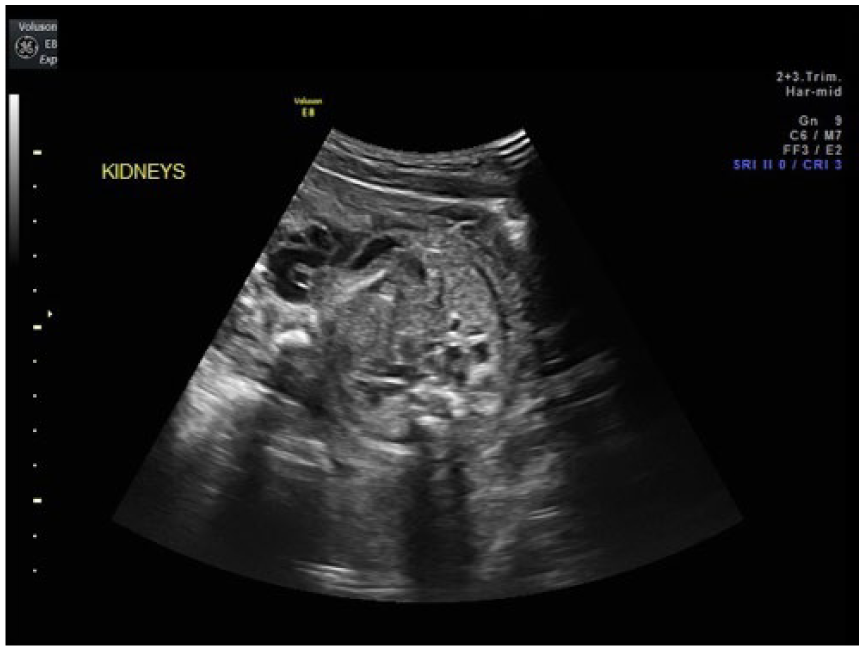
Limited assessment of multicystic kidneys at 26 weeks gestation. The lack of amniotic fluid volume limited evaluation of renal tissue.
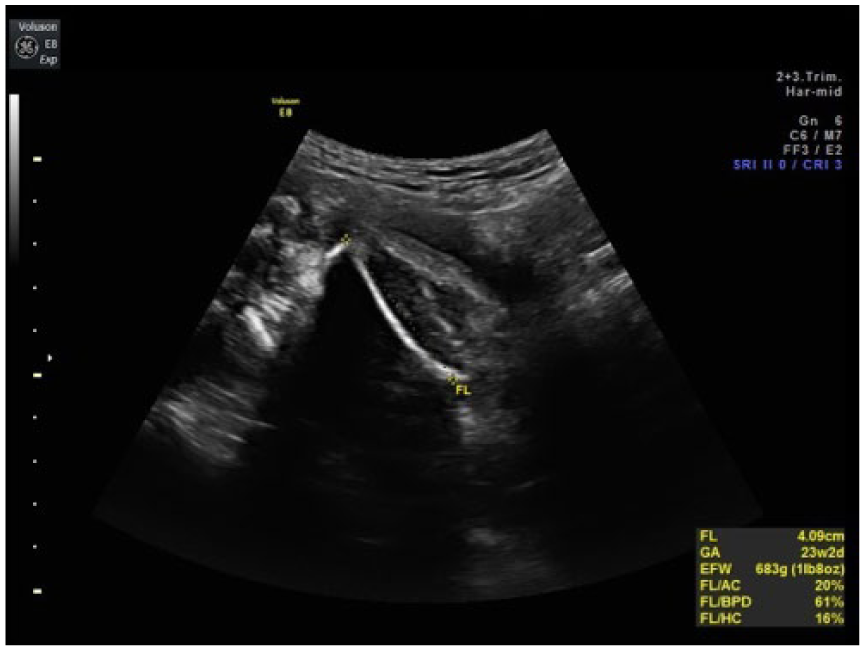
A single femur bone at 26 weeks gestation.
A fetal echocardiogram showed mild right ventricular hypertrophy with normal left ventricle size, an abnormal cardiac axis of 11 degrees and a cardiothoracic ratio of 0.6, a small perimembranous ventricular septal defect, and a small amount of pericardial effusion. No direct evidence of congenital heart disease was noted, so the abnormal axis and cardiomegaly were thought to be due to lung hypoplasia.
A repeat anatomic sonographic assessment 3 weeks later revealed a single femur bone and a lower leg bone that appeared bowed and fractured (Figure 5) as well as confirmed the previous sonographic findings. Maternal blood was drawn for noninvasive prenatal screening to evaluate for fetal chromosomes, including sex chromosomes, and microdeletions.
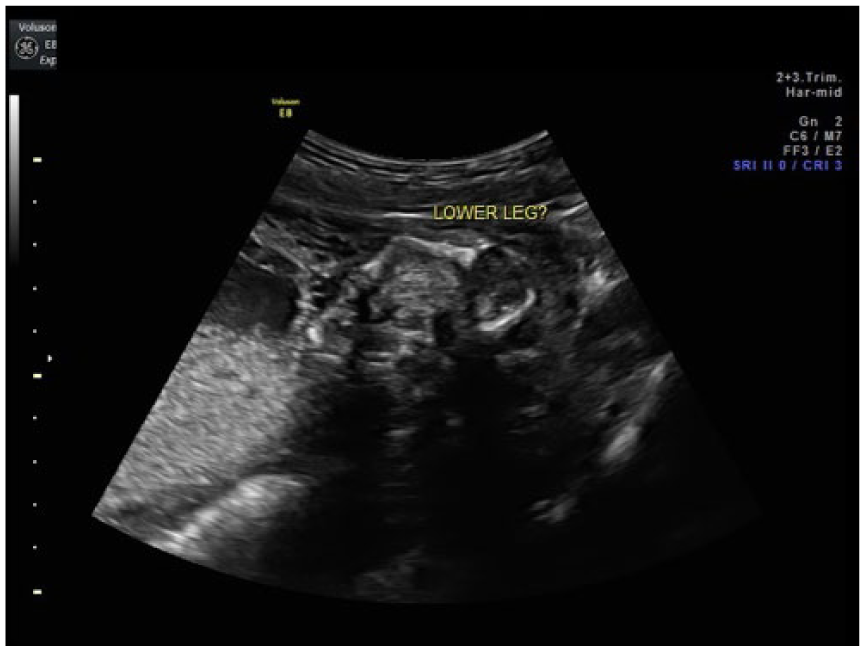
A single fractured lower leg bone at 26 weeks gestation.
The patient presented to the labor and delivery unit at 29 weeks, and the stillborn fetus was delivered vaginally. Weighing 1.3 kg (2.86 lb), the delivery was complicated by a footling breech presentation and prolapsed cord. Postnatal findings included a missing left thumb, fused lower extremities with the appearance of three to four fused feet (Figure 6), penis-like appendage located on the lower fused limbs, imperforate anus, skin tag distal to imperforate anus (Figure 7), and three-vessel cord. Although prenatal imaging demonstrated a single umbilical artery, no follow-up was performed after delivery to determine the discrepancy between prenatal and postnatal findings. The patient declined any further testing, including autopsy and karyotyping.

Postmortem image at 29 weeks gestation, showing the absence of the thumb on the left hand.

Postmortem image at 29 weeks gestation, demonstrating the phallus-like appendage near the sacrum.
Noninvasive prenatal screening results returned shortly after delivery, negative for trisomies 13, 18, and 21, with sex chromosomes indicating a female fetus. Microdeletions for 22q11.2, 4p- (Wolf-Hirschhorn), 15p11.2, 5p- (Cri du Chat), and 1p36 were also tested and not detected in the sample.
Discussion
Sirenomelia was first discussed in the literature in 1542 by Rocheus 1 and is characterized by a single lower extremity with the presence of severe skeletal, urogenital, and gastrointestinal anomalies.1,10 Some research states that sirenomelia is a severe form of caudal regression, whereas other research states that it is a separate anomaly. Sirenomelia, although incredibly rare, should be considered as a differential diagnosis any time severe oligohydramnios or anhydramnios is present with renal anomalies and there is an inability to distinguish distinct lower extremities, especially in the second trimester.
Caudal regression syndrome is a disruption of the distal neural tube or abrupt termination of the lower spine. 10 It is typically associated with normal or increased amniotic fluid volume, 1 and the lower extremities are typically positioned in a cross-legged “Buddha” or “tailor’s position” and movement is not seen from that position. 10 There is an association with maternal diabetes, with 1% of infants born to diabetic mothers being diagnosed with caudal regression syndrome. 10 There are associations with renal disease, genitourinary abnormalities, and congenital heart disease. 10 One article mentioned that the key feature to determine the difference between caudal regression syndrome and sirenomelia is the anatomy of the umbilical artery. 5 Sirenomelia is always documented with a single umbilical artery that arises from the aorta, whereas caudal regression syndrome will have two umbilical arteries. 4
Two types of classifications of sirenomelia have been discussed, one of which categorizes based on the number of feet present and the other of which categorizes based on the presence or absence of lower limb bones.4,9
The first classification, credited to Förster, is dependent on the presence or absence of feet.1,4 Symelia apus is the most common form and is characterized by a single lower extremity with absent or rudimentary feet; on a radiograph, a single femur is identified with either one or two tibia and absent fibula.1,4 In cases of symelia unipus, a single foot is present with up to ten toes visualized, as well as two femora, two tibia, and two fibulae identified.1,4 Symelia dipus is characterized by two distinct feet, typically malrotated and often fused with a fin or flipper-like appearance.1,4
The second classification, credited to Stocker and Heifetz, has seven categories depending on the presence or absence of lower extremity bones.1,4 Type I consists of all lower extremity bones present (two femora, two tibia, two fibulae).1,4 Type II demonstrates a single fibula. 1 Type III is identified by an absent fibula.1,4 Type IV consists of partially fused femora and fused fibulae.1,4 Type V is identified by partially fused femora.1,4 Type VI demonstrates a single femur and single tibia.1,4 Type VII is a single femur and absent tibia.1,4
Clinically, sirenomelia typically presents with merging, malrotation, and dysgenesis of the lower extremities, 1 imperforate anus, and defective or absent external genitalia. 6 There is no known association of chromosomal aneuploidy with sirenomelia. 7 The recurrence risk is the same as the risk in the general population. 4 There are a few theories as to the pathogenesis, but it is still not well understood. The first is a vascular steal theory, hypothesizing that blood flow is diverted from the vitelline remnant, causing distal tissues to be either malformed or absent.3,4,8 A second theory suggests that defects develop during blastogenesis due to an insult to the caudal neuropore. 4
The incidence of sirenomelia has been reported as a range of 1 in 60 000 live births 1 up to 1.5:100 000 to 4.2:100 000 births, 4 with a male predominance of almost three to one.2,4 Multiple sources also state an estimated 100- to 150-fold increase in the incidence of sirenomelia with monozygotic twinning versus a singleton pregnancy.1,4,7 Diabetic mothers are at a 2% increased risk for carrying a fetus with sirenomelia. 4 There are few reports of neonates surviving with sirenomelia, likely attributed to renal agenesis or dysgenesis and associated renal failure 8 with subsequent lung hypoplasia.
Sonographically, sirenomelia is a notoriously difficult diagnosis. The combination of anatomic complexities and severe oligohydramnios or anhydramnios can make this syndrome difficult to image in the second and third trimesters. Several reports noted the importance of first trimester and early second trimester sonogram to evaluate fetal anatomy, before amniotic fluid volume decreases.1,2 Sirenomelia could be suspected any time anhydramnios is identified, especially with renal agenesis or renal dysgenesis or the inability to distinguish separate lower extremities, or if the extremities appear fixed in the same plane and do not move independent from each other. Additional findings of intrauterine growth restriction, a shortened spine, and a single umbilical artery should increase suspicions for sirenomelia.1,10 The use of power or color Doppler can be helpful in evaluating the lower extremity vasculature. Fetuses with sirenomelia commonly present with abnormal vascularity to the lower extremities, including failure of the aorta to branch into the main iliac arteries. 4
However, even with these findings, it is suggested that more than 50% of sirenomelia cases are misdiagnosed prenatally. 10 Magnetic resonance imaging can be useful in any case of anhydramnios and can confirm renal agenesis. 10 In general, MRI provides improved visualization for fetuses with severe oligohydramnios or anhydramnios.
Postnatally, sirenomelia is identified as a single rudimentary lower extremity with imperforate anus and Potter facies. 6 On autopsy, these individuals are noted to have absent or rudimentary internal genitalia, absent or rudimentary rectum and anus, absent or abnormal urinary system (including kidneys and bladder), a single umbilical artery, scoliosis, and other skeletal and spinal abnormalities. 4 Reports have documented that fetuses with sirenomelia lack a normally tapering lumbosacral spine, 10 which could include sacral agenesis, lumbosacral agenesis, and a variety of neural tube defects.1,4,10
Sirenomelia is generally considered a lethal diagnosis, typically due to the associated renal difficulties and subsequent pulmonary hypoplasia. However, if adequate renal function is present, the fetus’s chance of surviving outside the womb increases. 1 There is no data on treatment or long-term outcomes of infants with this diagnosis; there have been fewer than 12 cases reported in the literature surviving past the neonatal period. 4
Conclusion
Sirenomelia is a complex constellation of abnormalities typically diagnosed after birth. The combination of severe oligohydramnios or anhydramnios and abnormal lower extremity configuration makes this specific fetal abnormality difficult to evaluate by sonography. However, the use of first trimester and early second trimester sonogram and MRI in the late-second and third trimesters can assist obstetric staff with diagnosis. Detecting renal abnormalities, anhydramnios, and a single umbilical artery could be the indication that a fetus has a lethal malformation such as sirenomelia.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.