
Abstract
Gallbladder perforation is a complication of gallbladder disease. There are high morbidity and mortality rates, and it is believed that this is due to the delay in diagnosis and when the condition is managed conservatively. Sonography combined with computed tomography can be used to identify gallbladder perforation and the presence of hepatic abscesses. Sonographic findings for gallbladder perforation may include the presence of a stone outside of the gallbladder, an obvious defect in the gallbladder wall, and other signs such as distended gallbladder, thickened gallbladder wall, striated appearance of the gallbladder wall, gallstones, debris/sludge, and adjacent abscesses. It is important for a sonographer to recognize these signs so that prompt treatment can be initiated. This case presents the sonographic and computed tomography findings of a type II perforated gallbladder as a result of a large stone that eroded into the liver with the subsequent development of two hepatic abscesses.
Introduction
Gallbladder perforation is a complication of gallbladder disease and is a potentially life-threatening condition. There are three types of perforation, according to Niemeier’s classification, and the case presented is a type II perforation, which involves the formation of hepatic abscesses. 1 The cause of gallbladder perforation can vary and can be attributed to a combination of processes. The signs and symptoms of this complication can be similar to those of uncomplicated acute cholecystitis. Gallbladder perforation can be detected with sonography, but it is important for the sonographer to be familiar with the sonographic signs, such as the presence of hepatic abscesses and a defect in the gallbladder wall, which was detected in this case.
Case Study
A male in his mid-60s presented to the emergency department via emergency medical services complaining of right upper quadrant abdominal pain, fever, nausea, vomiting, and generalized weakness that began earlier that day. A review of the patient’s medical records revealed type 2 diabetes mellitus, chronic kidney disease, and chronic lymphocytic leukemia. Medical records also revealed a history of cholelithiasis without evidence of acute cholecystitis that was diagnosed 4 years prior. On admission to the emergency department, the emergency physician ordered blood tests. The laboratory values demonstrated elevated white blood count and elevated aspartate aminotransferase; however, the values for bilirubin, alanine transaminase, lipase, and alkaline phosphatase were in the normal range. A chest radiography and sonography examination of the gallbladder was also ordered. The chest radiographs showed a small left pleural effusion (Figure 1).
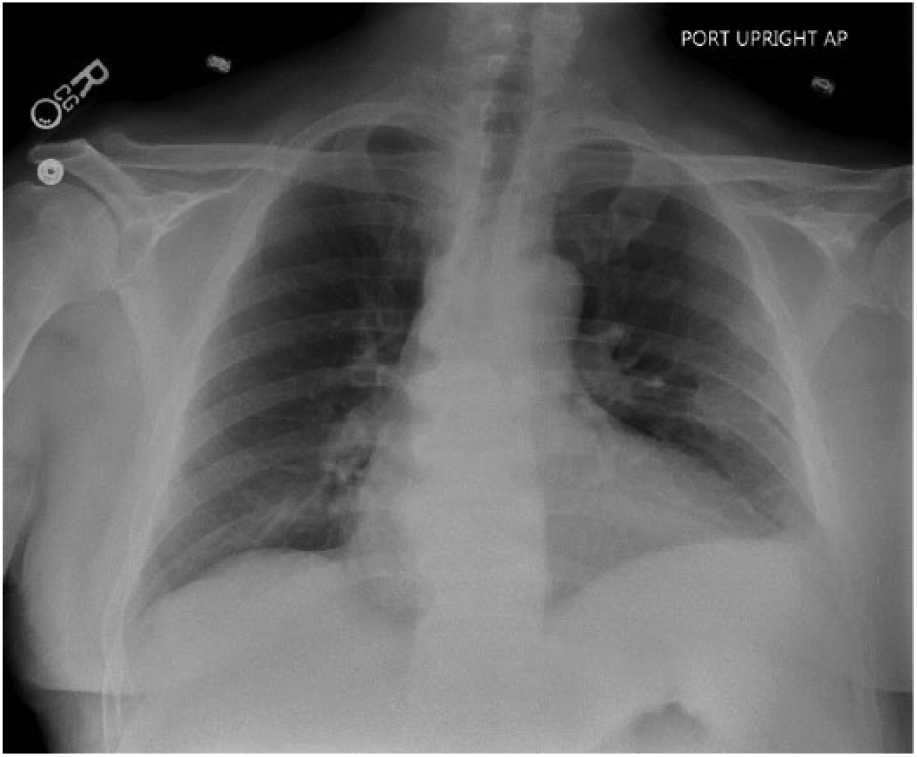
Small left pleural effusion.
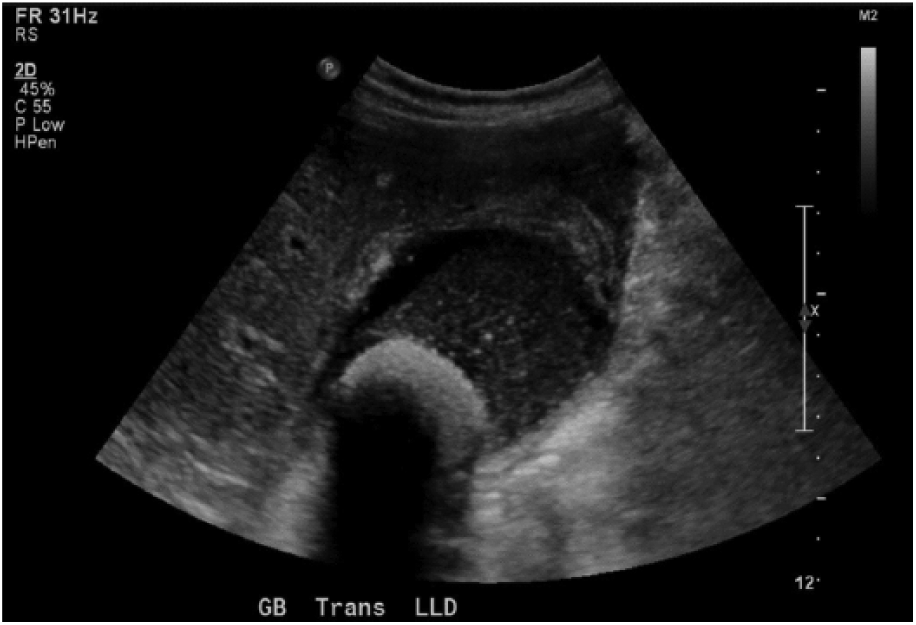
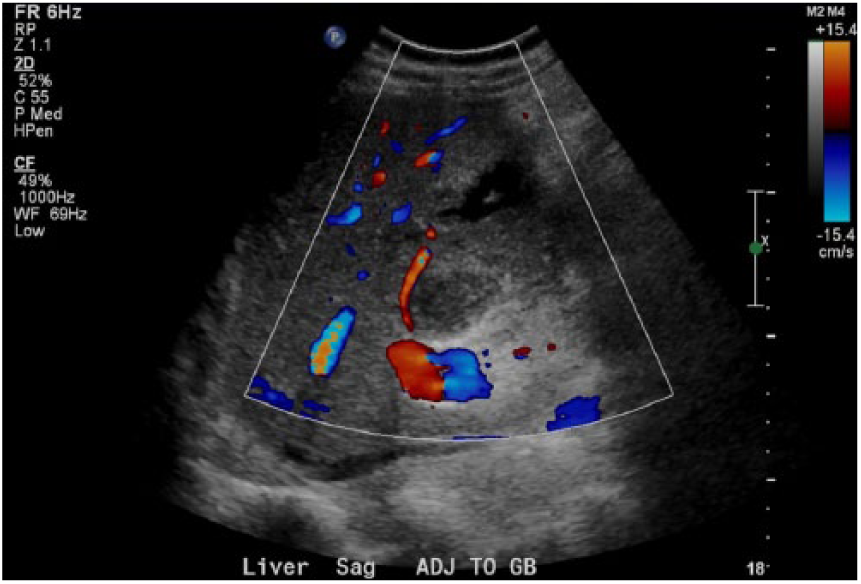
The sonographic evaluation was carried out with a Philips IU22 ultrasound system (Philips North America Corporation, Andover, MA, USA) using a 5 to 1 MHz curved-array transducer. The liver appeared mildly heterogeneous and the common bile duct appeared to be within normal limits (Figure 2). The right kidney appeared normal and the pancreas was not visualized due to overlying bowel gas. There was echogenic material and two large partially mobile and shadowing calculi within the gallbladder lumen (Figures 2-4). The gallbladder wall was not well delineated and appeared significantly thickened, with a measurement approaching 1 cm (Figure 5). There was evidence of surrounding inflammation adjacent to the gallbladder (Figure 6). A positive sonographic Murphy sign was reported.

Liver.
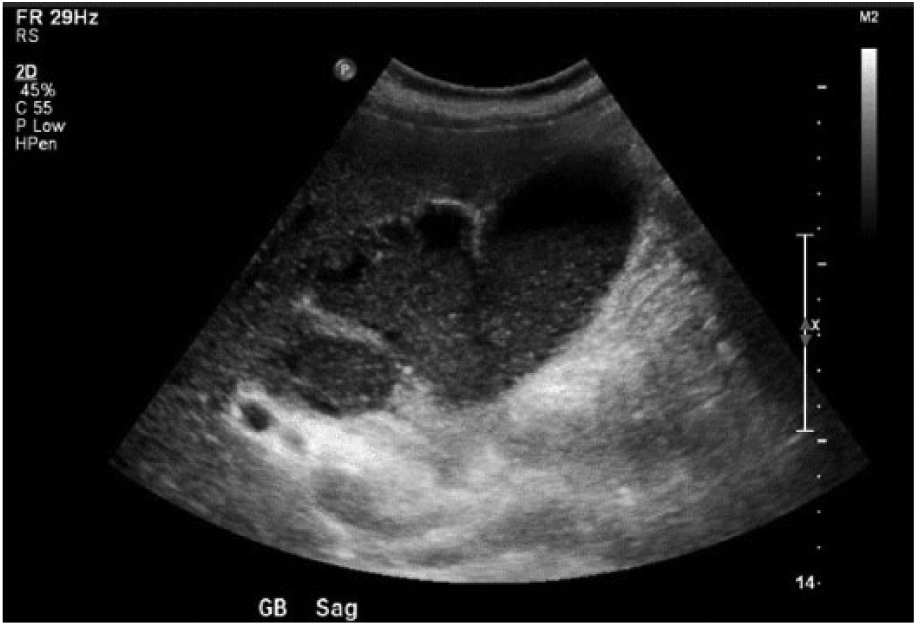
Gallbladder sludge with adjacent fluid collection in liver parenchyma.
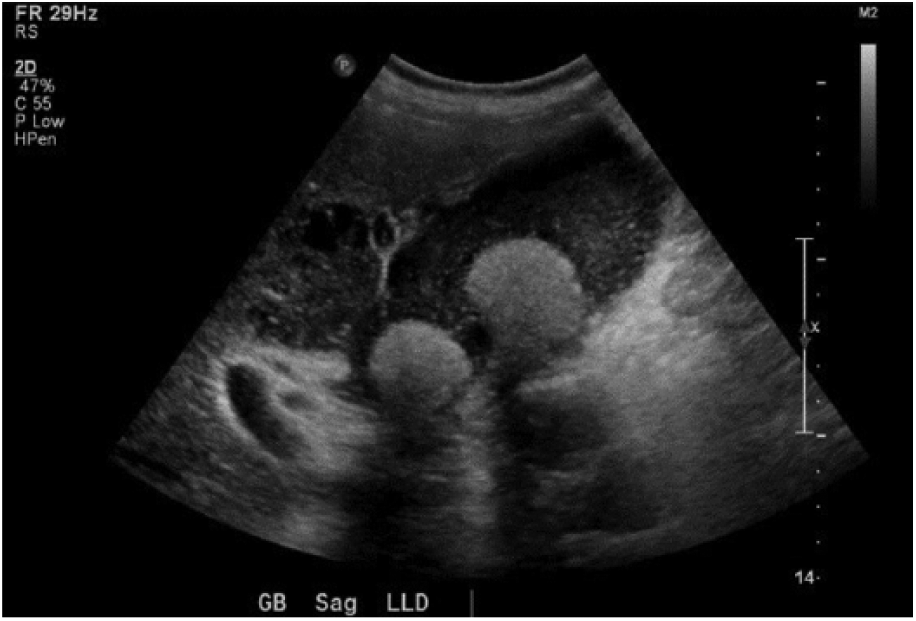
Gallstones, sludge, and adjacent fluid collection.
Thickened gallbladder wall.
Fluid collection posterior to gallbladder.
The patient was admitted to the hospital for further evaluation, and after a review of the patient’s medical history, it was reported that the patient’s type 2 diabetes mellitus, chronic kidney disease, and chronic lymphocytic leukemia appeared to be stable. A noncontrast abdomen and pelvic computed tomography (CT) scan was ordered. The CT scan revealed a prominently distended gallbladder with multiple gallstones, with the largest stone measuring 3.7 cm (Figure 7). The gallbladder wall was thickened with a mild increase in attenuation of the surrounding fat consistent with acute cholecystitis (Figure 8). Also ordered at admission was a nuclear medicine hepatobiliary scan, which revealed a nonvisualized gallbladder both pre- and postmorphine challenge. The radiologist reported that this finding should be viewed with suspicion for acute cholecystitis.
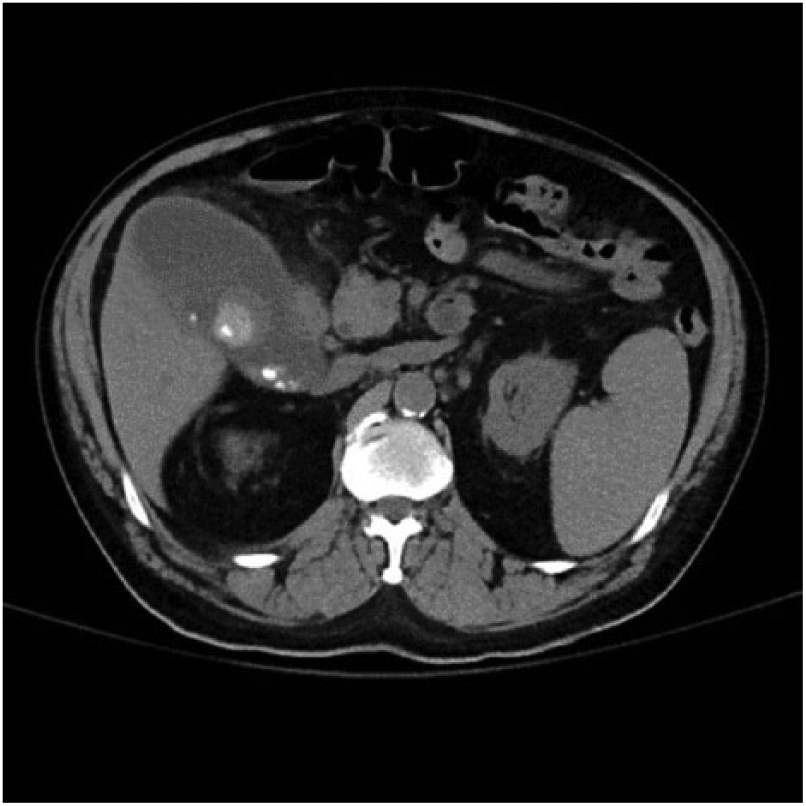
Distended gallbladder with multiple stones.
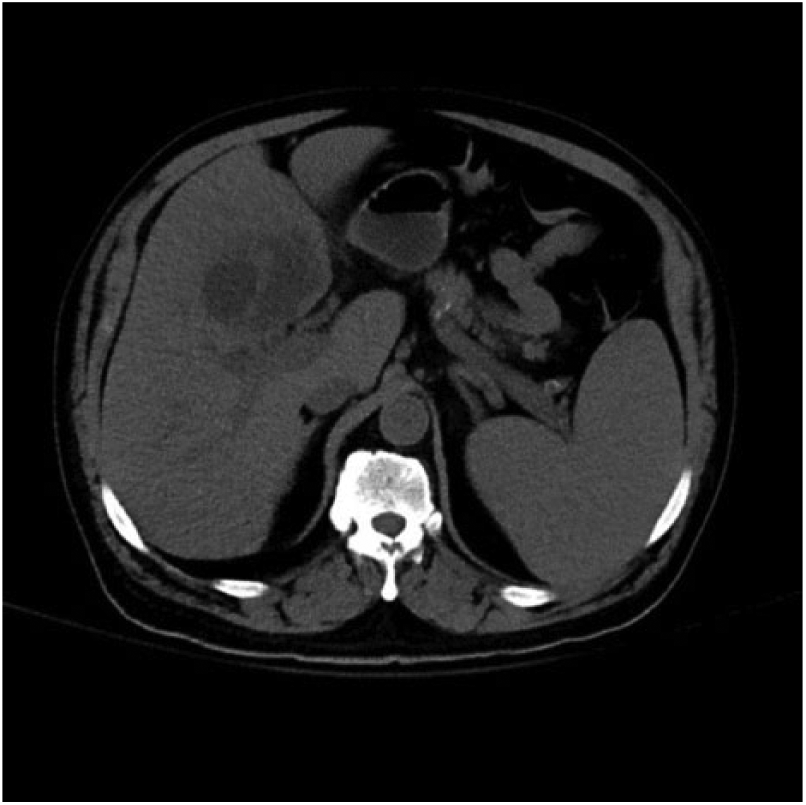
Inflammation of liver parenchyma adjacent to gallbladder.
It was decided that surgical management for cholecystitis was necessary. A cholecystectomy was performed 2 days after the patient presented to the emergency department. Surgical findings were consistent with the gallbladder sonography examination and CT scan. The postoperative diagnosis was acute purulent cholecystitis and two hepatic abscesses: one abscess in the medial left hepatic lobe and the second one at the posterior wall of the gallbladder. The gallbladder was entirely necrotic and a large stone had eroded into the liver with a large abscess close to the porta hepatitis. The gallbladder was found to be adherent to the wall posteriorly. A Jackson-Pratt drain, which is a closed suction bulb and tubing used for drainage of fluid from inside the body, was put in place for drainage of the abscess posterior to the gallbladder.
The surgical pathology report indicated that the gallbladder was surrounded by thick fibrous tissue measuring up to 1.2 cm. Included with the gallbladder specimen were six black-brown stones ranging from 0.3 to 3.0 cm. The gallbladder was grossly disrupted and no intact gallbladder neck could be identified. The mucosal layer had a few areas of hemorrhage.
Subsequently, the patient was sent back to surgery for sphincterotomy and stent placement due to bile leakage. Additional CT imaging status post cholecystectomy showed a loculated complex air- and fluid-filled collection in the gallbladder fossa extending into the right hepatic lobe. There was also suspicion for loculation in the lesser sac and along the right hepatic edge. Due to the persistent abscesses, the patient had a CT abscess drainage and additional catheter placement. Culture sensitivity was positive for Enterococcus, Escherichia coli, and Klebsiella.
The patient was discharged to home health care 17 days after presenting to the emergency department, with intravenous antibiotics and discharge instructions to follow up with the surgeon and primary care physician in 2 weeks. No additional follow-up history was available.
Discussion
The cause of gallbladder perforation varies with each incident and can be a combination of processes. Bacterial infections are thought to reach the gallbladder through the lymphatic system. The presence of bacteria in the gallbladder can result in edema, ulceration, gangrene, and formation of pus, which can eventually lead to gallbladder perforation. 2 It is thought that emphysematous, gangrenous, and hemorrhagic cholecystitis can cause weakening of the gallbladder wall. 3 Also, retention of bile in the gallbladder and increased pressure due to the occlusion of the cystic duct can lead to vascular compromise resulting in necrosis. 4 Another possibility is that infection and dilatation of the Rokitansky-Aschoff sinuses can lead to necrosis of the gallbladder wall. 5 Other factors such as malignancy, trauma, and steroid use can be considered as other possible causes of gallbladder perforation. 6 Patient conditions such as immunocompression, 2 type 2 diabetes mellitus, and atherosclerotic heart disease can contribute to gallbladder perforation. 6
Signs and symptoms of gallbladder disease can be the same as those for uncomplicated acute cholecystitis. These signs can include right upper quadrant pain, generalized abdominal pain, tenderness, abdominal firmness, guarding, nausea, and vomiting. 5 Gallbladder disease is common and can be asymptomatic and remain undiagnosed until complications arise. Complications of gallbladder disease can be acute cholecystitis, biliary obstruction, acute pancreatitis, and cholangitis. Occasionally, more severe complications can occur such as Mirizzi syndrome, fistula formation, gallbladder perforation, and abscess formation. These complications are usually associated with high morbidity and mortality rates. 4 A study by Cheruvu and Eyre-Brook 7 found that almost 30% of patients presenting with acute cholecystitis had experienced complications. The research finds that early surgical intervention during the initial visit can reduce the chance of complications.
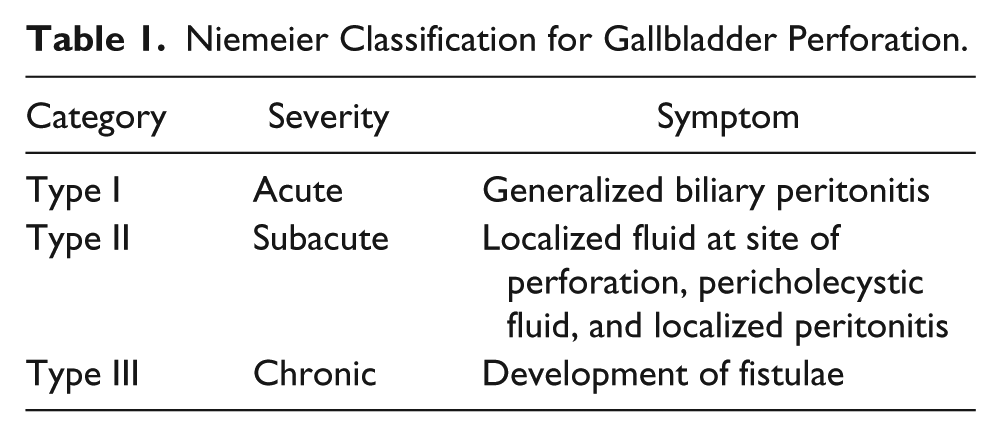
Gallbladder perforation is a severe complication of gallbladder disease and can be life threatening. 6 It is believed that the high morbidity and mortality rates are due to the delay in diagnosis and when the condition is managed conservatively. Also, the severity of this complication can depend on the age of the patient and presence of sepsis. 2 Mortality rates have been reported between 12% and 42%. The presence of gallstones is seen in 86.6% of cases of gallbladder perforation, 8 and 3% to 15% of patients presenting with acute cholecystitis with cholelithiasis result in perforation. 6 The types of gallbladder perforations were categorized by Niemeier in 1934. 1 Type I (acute) is associated with generalized biliary peritonitis. Type II (subacute) consists of localization of fluid at the site of the perforation, pericholecystic abscess, and localized peritonitis. Type III (chronic) is the formation of bilio-biliary or bilio-enteric or external fistulae (Table 1). 1
Niemeier Classification for Gallbladder Perforation.
A review of the literature found only a few cases of perforation that led to the development of intrahepatic abscesses. 9 Hepatic abscesses are defined as cavities of pus caused by bacteria within the liver tissue.10,11 Hepatic abscesses due to cholelithiasis are rare, 9 but hepatic abscesses caused by biliary disease account for approximately 50% to 60% of cases. Clinical signs and symptoms of hepatic abscesses can be abdominal pain, elevated liver enzymes, elevated body temperature, tachycardia, tachypnea, and leukopenia/leukocytosis. These abnormal clinical signs depend on the extent of the abscess and the severity of the sepsis, and the diagnosis is made by imaging. 10
Treatment for type II perforations is often a surgical intervention such as a cholecystectomy, abscess drainage with antibiotics, or drainage of free fluid in the abdomen if it is present. 5
Various conditions of the biliary system can cause acute abdominal pain, and many of these conditions can cause similar symptoms. Sonography can be the most valuable tool for initial evaluation to determine a specific diagnosis by reducing the differential diagnosis. 3 Differential diagnoses for gallbladder perforation include pneumobilia and air within the gallbladder, gas containing gallstones, or abscesses that are caused by carcinoma. 5 Detection of gallbladder perforation is very limited with sonography but can be detected by CT in 50% of patients. 12 However, both modalities are effective at detecting the signs of cholecystitis, such as fluid collection, thickened gallbladder wall, and the presence of stones. 13 To improve detection of gallbladder perforation with sonography, it is important to learn and recognize the signs of perforation. The most specific sign is called the “sonographic-hole” sign and this is where the gallbladder wall defect can be visualized. 12 Another specific sign is the visualization of gallstones outside of the gallbladder. 5 Other sonographic signs can be a distended gallbladder, thickened gallbladder wall, striated appearance of the gallbladder wall, gallstones, debris/sludge, and adjacent abscesses. 12 Gangrenous cholecystitis can have the appearance of microabscesses and hemorrhage in the gallbladder wall and complex fluid collections adjacent to the gallbladder. Also seen are bulging and layering of the gallbladder wall. 14 More than 90% of incidences of hepatic abscesses can be detected by sonography and CT. 10 The sonographic appearance of a hepatic abscess is acoustic enhancement, presence of a wall with hypoechoic border, septations, and internal debris.
Sonography and CT are usually the preferred imaging modalities for evaluation of acute abdominal pain, with sonography being the initial examination. 6 Gallstones are often missed on CT and sonography is more sensitive to the detection of stones. 2 However, CT is excellent at demonstrating gallbladder perforation. 15 Therefore, both imaging modalities can be used to diagnose gallbladder perforation. 6
Conclusion
Sonography is often the initial imaging modality utilized when a patient presents with right upper quadrant pain. Becoming familiar with the signs of gallbladder perforation will assist a sonographer in detecting these cases more often. This will help prevent the delay in treatment. In the case presented, the gallbladder wall defect and adjacent abscesses were identified and laparoscopic cholecystectomy with evacuation and drainage of the hepatic abscesses was performed, which confirmed the sonographic findings of gallbladder perforation.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.