
Abstract
Emphysematous cholecystitis (EC) is an uncommon form of acute cholecystitis, caused by secondary infection of the gallbladder wall with gas-forming organisms. The mortality rate of EC is as high as 25% due to complications such as gangrene, gallbladder perforation, pericholecystic abscess, and bile peritonitis. Traditionally, prompt emergency surgical intervention with open cholecystectomy is recommended for EC treatment. This case study of EC was diagnosed at an early stage with sonography and computed tomography and successfully treated by antibiotic treatment alone without surgery. With characteristic findings on sonography such as echogenic reflectors with posterior shadowing, EC is an important entity for sonographers to be able to identify. In the future as imaging with sonography and CT affords earlier diagnosis of EC, antibiotic therapy might be considered for some patients, but more evidence is needed to obtain the same outcome as this particular case.
Emphysematous cholecystitis (EC) is an uncommon form of acute cholecystitis, caused by secondary infection of the gallbladder wall with gas-forming organisms. The mortality rate of EC is as high as 25% due to complications such as gangrene, gallbladder perforation, pericholecystic abscess, and bile peritonitis.1,2 Traditionally, prompt emergency surgical intervention with open cholecystectomy is recommended for EC treatment. This case study presents a case of EC that was diagnosed at an early stage with sonography and computed tomography (CT), which was successfully treated with antibiotics treatment and not surgery.
Case Report
A 65-year-old woman with stage IV uterine cancer following total abdominal hysterectomy and bilateral salpingo-oophorectomy, poorly controlled type II diabetes mellitus, morbid obesity, hypertension, and atrial fibrillation on warfarin presented to the emergency department for four days of nausea, vomiting, fatigue, and anorexia.
She denied fevers, chills, chest pain, abdominal pain, diarrhea, constipation, dysuria, hematuria, or suprapubic pain. She also denied any bloody or bilious emesis. Her vital signs were within normal limits, and physical examination was unremarkable. Her abdomen was soft, nontender, and nondistended with positive bowel sounds and no evidence of organomegaly. The patient demonstrated a negative Murphy’s sign and had no reported flank tenderness. The patient provided no history of biliary surgery or biliary interventional procedures.
The patient was noted to have an elevated white blood cell (WBC) count and a urinalysis positive for leukocyte esterase. Blood cultures were negative for bacterial growth. Liver function enzymes and other laboratory values were otherwise normal. The patient was diagnosed with a urinary tract infection (UTI) complicated by renal abscess and admitted to the internal medicine service. Empiric treatment with piperacillin/tazobactum was begun.
During her hospitalization, a CT scan of the abdomen demonstrated left renal enlargement with perinephric stranding and distortion of the renal contour with increased fullness of the interpolar region, suggesting pyelonephritis with a concomitant renal abscess (Figure 1). CT images of the gallbladder showed a gallstone as well as gas seen within the nondependent portions of the gallbladder lumen and also within the common bile duct with no pericholecystic inflammatory changes (Figure 2).

Coronal computed tomography image of the left kidney demonstrating low attenuation area consistent with a renal abscess (arrow).
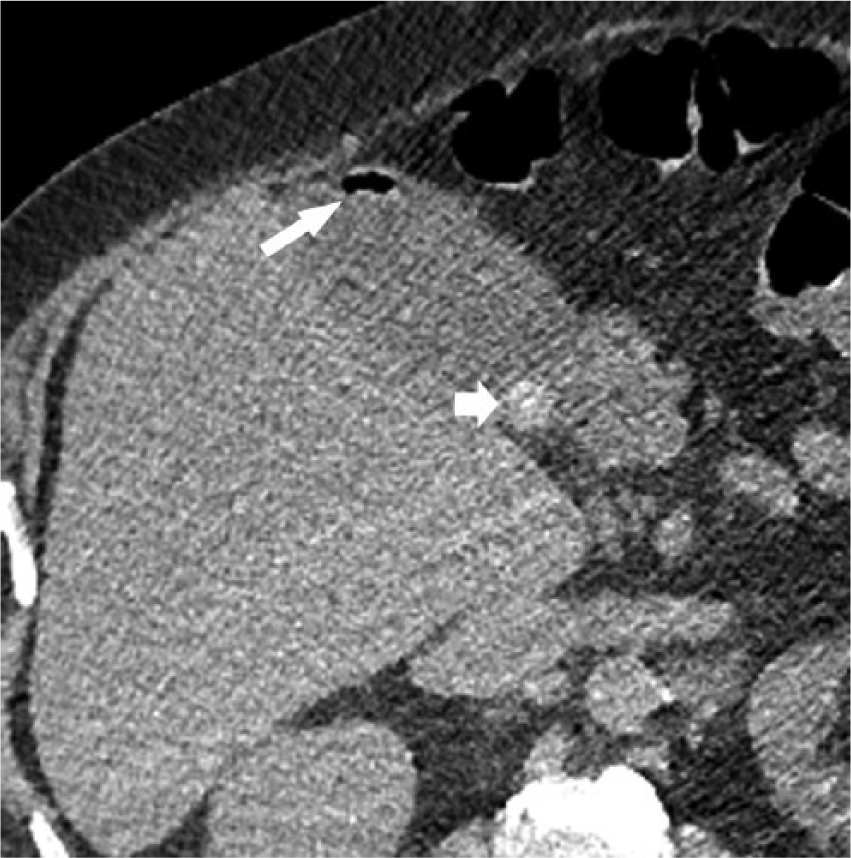
Transverse computed tomography image of the gallbladder demonstrating intraluminal gas (long arrow) and calcified gallstone (short arrow).
Given the CT findings of gas within the gallbladder, an abdominal sonogram was performed for further evaluation. The sonogram was performed using the LOGIQ 9 system with 4-MHz transducers (GE Healthcare, Milwaukee, Wisconsin). The sonogram of the abdomen at that time demonstrated gallbladder sludge, mild gallbladder wall thickening (5 mm), and intraluminal gas within the nondependent portion of the gallbladder, consistent with EC (Figure 3). Given the normal fat planes around the gallbladder and duodenum, considerations such as biliary enteric fistula were felt to be less likely, and a diagnosis of EC was made.
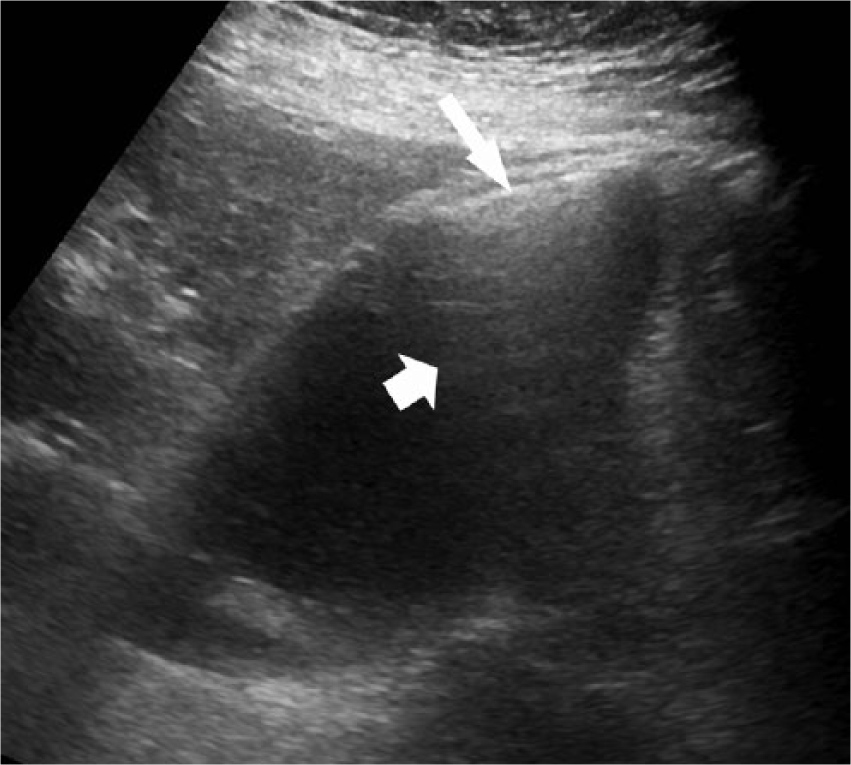
Longitudinal ultrasound scan of the gallbladder showing high-amplitude echoes from intraluminal gas (long arrow) casting distal shadowing (short arrow).
Given the patient’s hemodynamic stability and ability to tolerate antibiotics, an invasive intervention was not recommended by the team of urology physicians. Urine cultures demonstrated Klebsiella and Proteus that were sensitive to ciprofloxacin, so the patient discontinued piperacillin/tazobactam and began ciprofloxacin treatment for 14 days (500 mg bid). A follow-up renal sonogram, two weeks later, demonstrated interval improvement of the left renal abscess and resolution of the gas in the gallbladder.
Discussion
First described by Stolz in 1901, EC is characterized by the presence of gas within the wall or lumen of the gallbladder in the absence of an abnormal biliary-enteric communication.3,4 The pathophysiology is an acute infection caused by gas-producing organisms with gallbladder wall ischemia from microvascular compromise. The most commonly involved organisms are Clostridium species, Escherichia coli, Klebsiella species, and anaerobic streptococci. 2 In addition, it is associated with diabetes mellitus and has a greater incidence in men. 5
In this patient, it is possible that the organisms responsible for the renal abscess (Klebsiella and Proteus) secondarily infected the gallbladder as well, resulting in EC. Blood cultures returned negative for bacterial growth, most likely due to the initiation of prophylactic antibiotics at the time of admission. Initial therapy with piperacillin/tazobactam was effective in treating Klebsiella and Proteus, and the transition to ciprofloxacin similarly provided continued treatment of the culprit organisms.
While EC is an uncommon variant of acute cholecystitis, special attention must be given to patients with this condition, as it carries a high rate of morbidity and mortality due to an increased incidence of gangrene or perforation. In a review of 20 cases of EC, the reported mortality rate was as high as 25%, and the morbidity rate was as high as 50%. 6
The symptoms of EC may be similar to those of acute cholecystitis, including right upper quadrant pain, nausea, vomiting, and low-grade fever. A prompt diagnosis of EC is essential and sonography is often the initial imaging modality of choice. When more complicated variations of acute cholecystitis are suspected such as EC, CT provides a valuable complementary role and is quite sensitive for even minute gas bubbles.7,8
Sonography is less sensitive but highly specific for identifying air in the gallbladder and can be used to diagnose EC early and accurately.9,10 When there is air present in the gallbladder wall or lumen, echogenic foci with posterior dirty shadowing, or reverberation artifact, emanate from the gallbladder wall or lumen. While sonography can be accurately used to evaluate patients with EC, CT is the most specific imaging modality for the diagnosis of EC. General features on CT include air in the gallbladder wall or lumen, intraluminal membranes, irregular or absent gallbladder wall, irregular enhancement, and pericholecystic abscess. The presence of pneumoperitoneum is a surgical emergency, as this suggests gallbladder perforation.11,12
Emergent surgical intervention with open cholecystectomy is the preferred definitive treatment for EC, although alternative techniques such as laparascopic cholecystectomy and percutaneous cholecystostomy with broad-spectrum antibiotics for critically ill patients have been described.4–6,13 However, in the reported cases where percutaneous intervention was used, cholecystectomy was ultimately required.4,5,13
The differential diagnosis for sonographic evidence of gas in the gallbladder includes porcelain gallbladder, adenomyomatosis, and iatrogenic pneumobilia. EC can be differentiated from porcelain gallbladder and adenomyomatosis through changing the patient’s positioning, as the echogenic focus will be mobile only in EC. In addition, EC will demonstrate dirty shadowing due to the presence of air, whereas porcelain gallbladder will have a clean shadow due to the presence of calcifications.10,14 Porcelain gallbladder was previously thought to be a premalignant process, but recent large studies show that the risk for gallbladder carcinoma is approximately 5% to 7%. 15 Currently, no data are available to indicate the value of follow-up or new incidence, but it is estimated to be less than 1%, and current recommendations do not support follow-up in patients with porcelain gallbladder. 15
Adenomyomatosis of the gallbladder can mimic EC with the presence of reverberation artifact, but the sonographic finding of echogenic intramural foci that produce “comet tail” reverberation artifacts is specific for adenomyomatosis.16–18 Adenomyomatosis is a relatively benign finding and no intervention is usually needed, although surgical resection may be considered in symptomatic cases. 16 Iatrogenic pneumobilia is a common finding in patients with biliary stents, and a careful review of the patient history may provide support for this diagnosis. 8
Conclusion
In summary, this case provides a diagnostic workup of EC that was diagnosed early with sonography and responded completely with early antibiotic therapy alone. Of note is the fact that this diabetic patient had no clinical signs indicative of gallbladder disease. The patient’s UTI with renal abscess prompted early broad-spectrum antibiotic treatment, which likely provided incidental early treatment of her EC before more serious complications could develop. While initial CT findings demonstrated small amounts of gas in the nondependent portions of the gallbladder, the findings were not felt to be conclusive for EC, and sonography was able to provide a definitive diagnosis. With characteristic findings on sonography such as echogenic reflectors with posterior shadowing, EC is an important entity for sonographers to be able to identify. Without early identification and prompt treatment of EC, the potential for morbidity and mortality increases due to the development of more serious complications such as gangrene or gallbladder perforation. In the future, as imaging with sonography and CT affords earlier diagnosis of EC, antibiotic therapy may be used more often to avoid the morbidity of surgery in these often high-risk patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.