
Abstract
Emphysematous cholecystitis is a rapidly progressing, life-threatening condition that warrants immediate surgical intervention following diagnosis. This condition is associated with a high mortality rate; therefore, early detection is essential in order for intervention and treatment to ensure the best possible patient outcome. Visualization of air within the biliary system is the hallmark of emphysematous cholycystitis, and sonography has proven to be a noninvasive, sensitive imaging modality for detection of air within the biliary system. This case study presents a patient with emphysematous cholecystitis and the role that sonographic imaging had in its early detection and diagnosis.
Introduction
Emphysematous cholecystitis is a rare variant of acute cholecystitis, occurring in less than 1% of all cases of acute cholecystitis. 1 Emphysematous cholecystitis is characterized by the presence of bacteria, which creates air within the gallbladder and/or biliary system. 2 This condition is thought to be caused by vascular insufficiency to the gallbladder wall, which results in devitalized tissue, creating an anaerobic atmosphere that allows bacteria to thrive.
Detection and diagnosis of emphysematous cholecystitis relies on demonstrating gas within the gallbladder lumen/wall or within the bile ducts, which can be accomplished by both computed tomography (CT) and sonography. While CT is thought to be the most sensitive imaging modality for identifying air within the gallbladder/biliary system, sonography also has a role when used in conjunction with CT to confirm the presence of air as well as locate gallstones that may be impacted within the biliary tract. 2 Emphysematous cholecystitis has a mortality rate much higher than that of acute cholecystitis, 20% as compared to 1.4%, respectively, because of the increased incidence of gallbladder wall gangrene and perforation; thus, early diagnosis and intervention is imperative.2,3
Case Report
A man in his mid 70s was brought to the emergency room after his neighbor found him on the ground outside of his home. Upon admittance, he was found to have atrial fibrillation with rapid ventricular rate. The patient denied experiencing significant abdominal pain, nausea, or shortness of breath. He stated that he smoked one pack of cigarettes a day but does not consume alcohol. The man was known to have an extensive medical history including diabetes mellitus, hypertension, ischemic cardiomyopathy, coronary artery disease, chronic obstructive pulmonary disease, hyperlipidemia, and chronic kidney disease. Vital signs at the time of admittance were stable with a temperature of 97°F, a pulse rate of 107 beats per minute, and a blood pressure of 124 mmHg systolic and 69 mmHg diastolic. Initial laboratory tests showed significantly elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST). An abdominal CT showed gas throughout the biliary tract, particularly concentrated within the biliary tree, ducts, and gallbladder (Figures 1–3). Based on the CT findings, a complete abdominal sonogram was ordered to better assess the diameter of the common bile duct as well as assess the biliary system for the presence of gallstones. A paraisopropyl iminodiacetic acid (PIPIDA) scan was also done to assess the patency of the common bile duct.
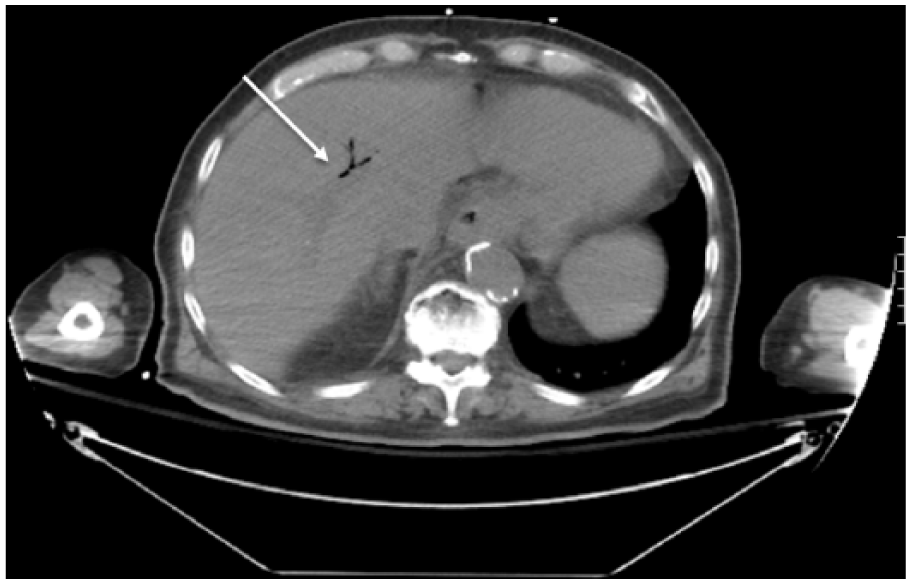
Computed tomogram (CT) showing air within the biliary tree in the axial plane (arrow).
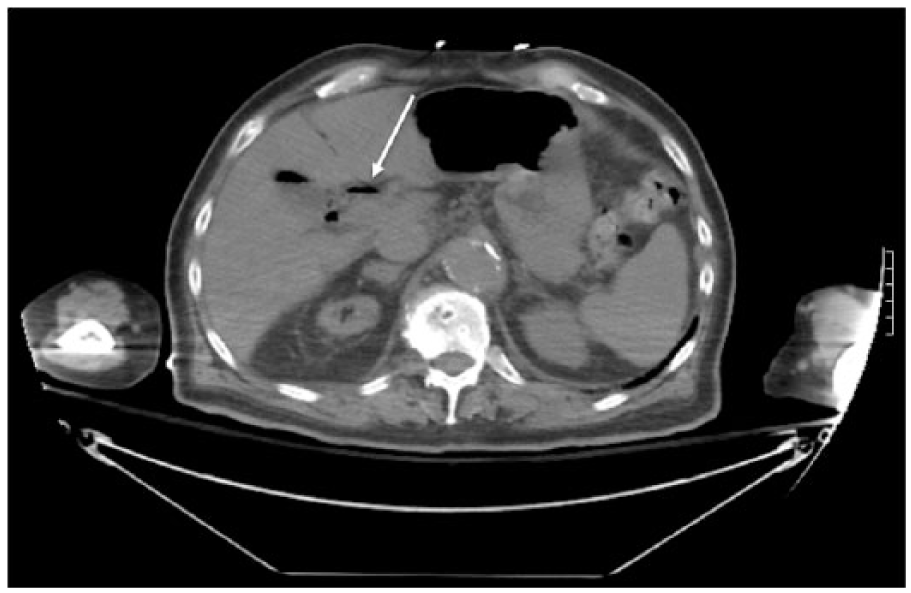
Computed tomogram (CT) showing air within the cystic duct in the axial plane (arrow).
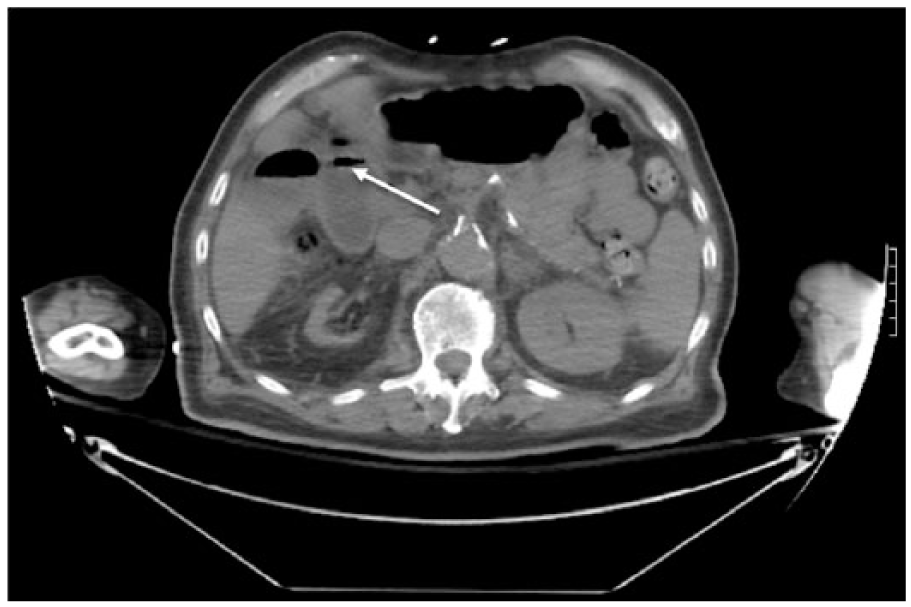
Computed tomogram (CT) showing air within the gallbladder wall in the axial plane (arrow).
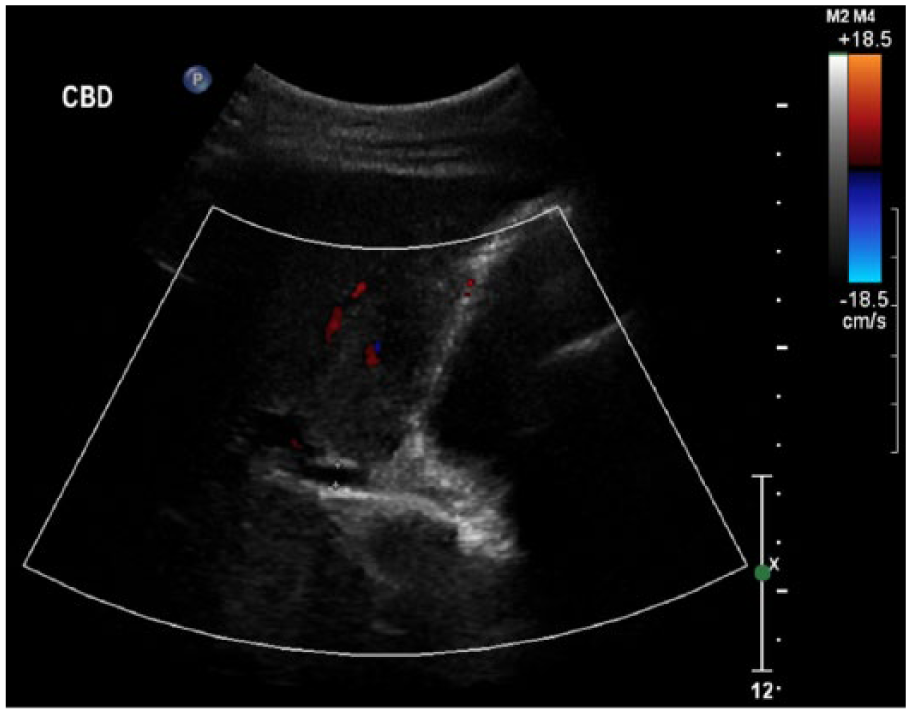
A complete abdominal sonographic examination was performed using a Philips iU22 ultrasound machine (Philips Ultrasound, Bothel, Washington, USA) with a curved array C5-1 transducer. The protocol included complete sonographic evaluation of the aorta, inferior vena cava, pancreas, liver, gallbladder, common bile duct, kidneys, and spleen. The sonographer utilized various patient positions throughout the examination, including supine, left lateral decubitus, and right lateral decubitus positions, to accurately demonstrate dirty shadowing and reverberation artifacts that would help confirm the presence of pathology within the biliary system. Dirty shadowing and reverberation artifacts were noted sonographically within the common bile duct, gallbladder, and gallbladder wall (Figures 4–6), consistent with the presence of air within the biliary system. The gallbladder wall measured 0.299 cm, which was at the upper limits of normal (Figure 7). Trace amounts of pericholecystic fluid were noted (Figure 8). An echogenic focus demonstrating posterior shadowing was visualized within the cystic duct measuring 0.68 cm, likely representing a calculus (Figure 9). The common bile duct diameter was 0.41 cm, within normal limits for the patient (Figure 10). Changing patient positions during the sonographic examination was key in staging the condition and detecting stones within the biliary system, which was suggested but not definitively diagnosed by CT. Computed tomography and sonography complemented one another in this case, and together they were able to determine the stage to which the condition had progressed and detect compounding factors that could influence treatment, such as the calculus seen in the cystic duct by sonography (Figure 9). The patient failed to demonstrate a positive Murphy’s sign. Additionally, the complete abdominal sonogram demonstrated abnormally course echotexture of the liver and renal atrophy, likely resulting from the patient’s known conditions of heart failure and chronic kidney disease, respectively.
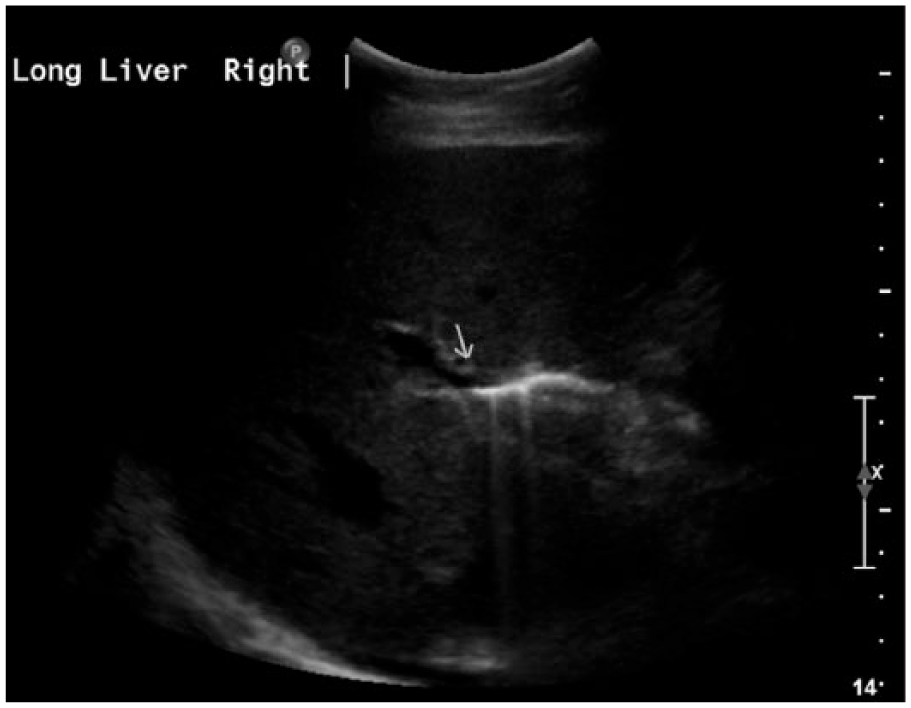
Sonogram showing echogenic air within the common bile duct (arrow) with significant ring-down artifact (dirty shadowing).
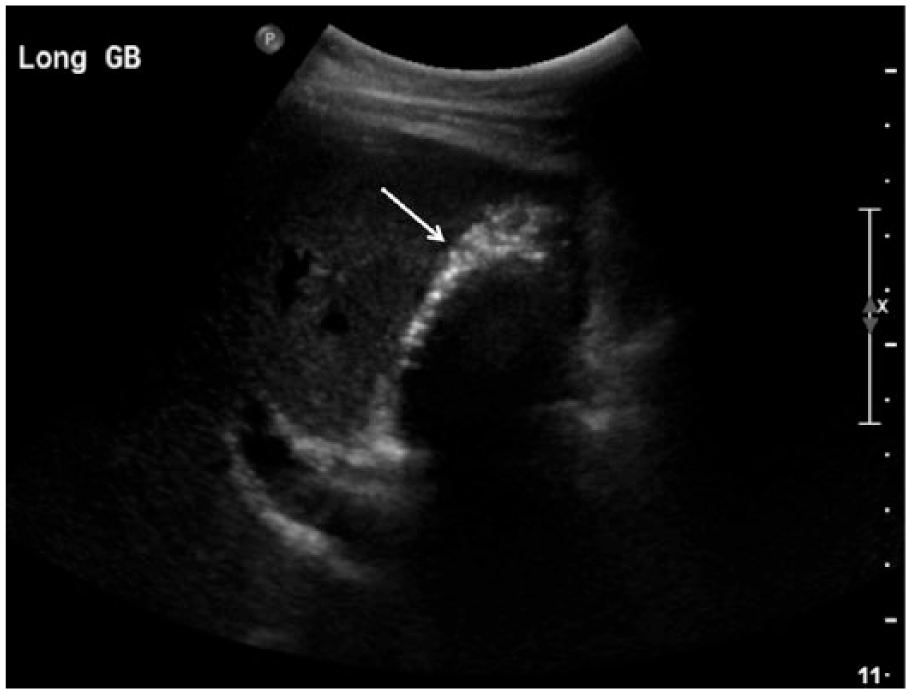
Sonogram showing the long axis of the gallbladder with brightly echogenic air within the gallbladder wall (arrow) and posterior acoustic shadowing.
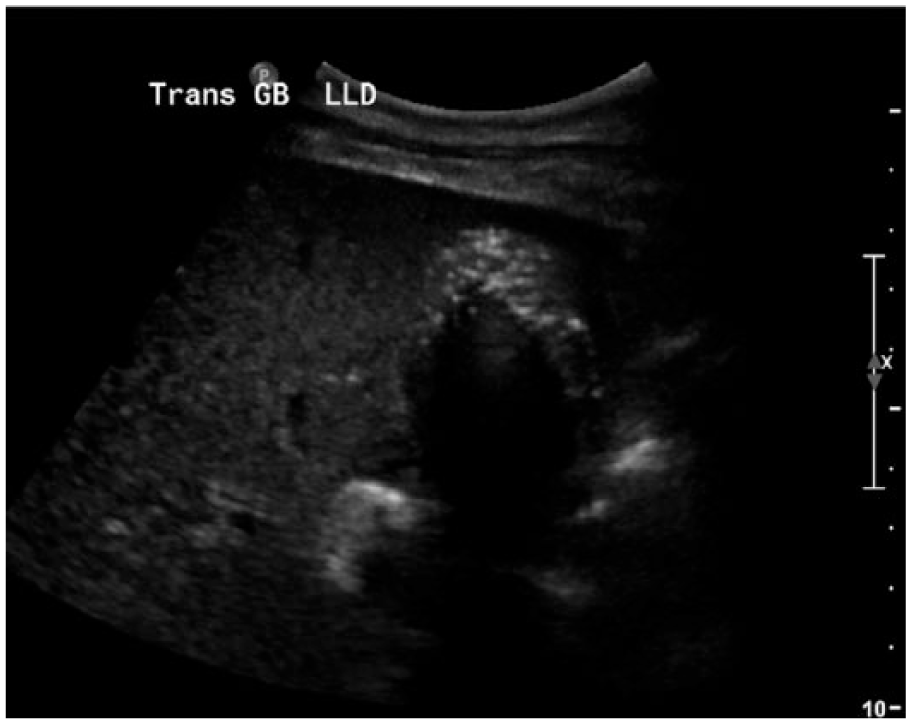
Sonogram showing the transverse axis of the gallbladder with brightly echogenic air within the gallbladder wall and posterior acoustic shadowing.
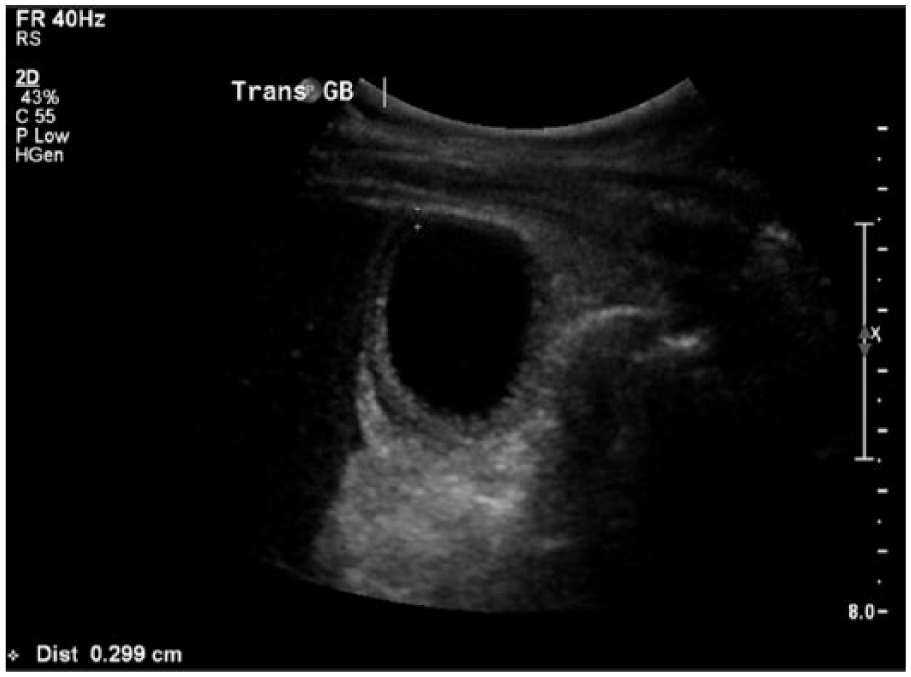
Sonogram showing the transverse axis of the gallbladder, with the anterior-posterior dimension of the gallbladder wall measuring 0.299 cm.

Sonogram showing trace amounts of pericholecystic fluid surrounding the gallbladder (arrow) in the transverse plane.
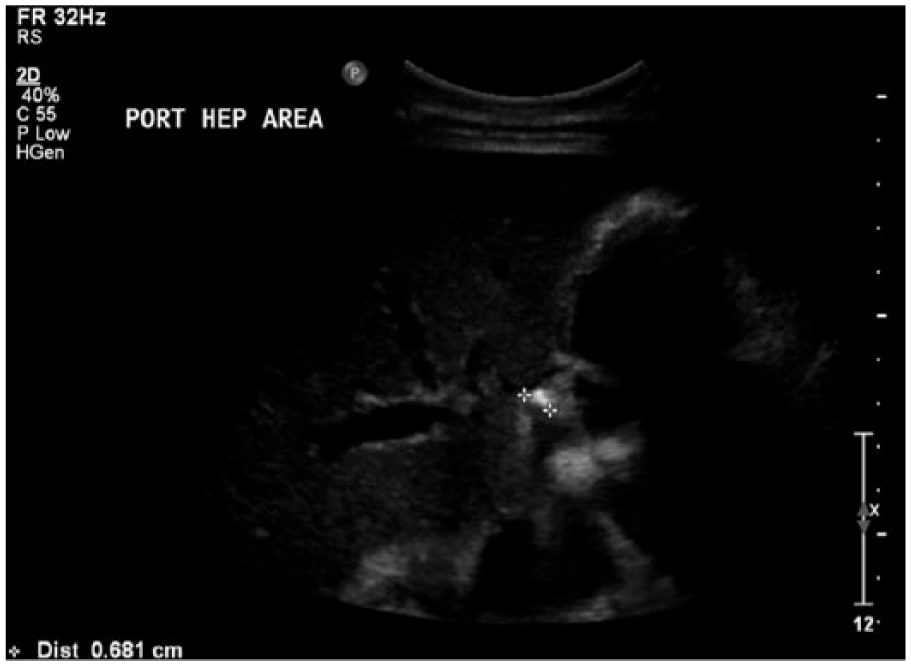
Sonogram showing an echogenic focus with posterior shadowing within the cystic duct, likely representing a calculus.
Sonogram showing the common bile duct with the anterior-posterior dimension measuring 0.41 cm.
The patient was diagnosed with stage three emphysematous cholecystitis, as air was visualized within the common bile duct by both CT and sonography (Figure 4). This late stage of disease prompted immediate intervention and treatment. Typical treatment for emphysematous cholecystitis is emergent surgical removal of the gallbladder, or cholecystectomy, but because of this patient’s multiple comorbidities, he was not considered a candidate for surgical intervention. The patient was instead given antibiotics intravenously, with suggested placement of a cholecystostomy tube if he did not respond to antibiotic treatment; however, this ultimately was not necessary. Following treatment via broad-spectrum antibiotics and improvement in clinical status after one week, the patient became combative and argumentative and stated that he did not wish to undergo further testing. Because his condition was stable, he was discharged from the hospital at that time.
Ten days after his voluntary discharge from the hospital, the patient was again admitted, this time for increasing shortness of breath and atrial fibrillation with rapid ventricular response. His worsening condition was attributed to his multiple comorbidities and not to the previously diagnosed condition of emphysematous cholecystitis. Again, the patient was combative and noncompliant with medical orders and treatment options, and he again expressed that he did not wish to undergo any other procedures or further testing. The doctors discussed the patient’s medical condition at length with his family, and all parties agreed that conservative management was preferred.
Discussion
Emphysematous cholecystitis is caused by gas-forming organisms within the gallbladder, most commonly Clostridia species, Escherichia coli, Klebsiella species, and anaerobic streptococci.4,5 The symptoms of emphysematous cholecystitis are typically vague, such as right upper quadrant pain, low-grade fever, nausea, and vomiting. 6 While these symptoms may be identical to those of acute cholecystitis, the two conditions are pathophysiologically different. Acute and chronic cholecystitis are typically caused by obstruction of the gallbladder neck secondary to cholelithiasis, whereas emphysematous cholecystitis results from ischemic necrosis of the gallbladder wall secondary to occlusion or thrombosis of the cystic artery. 5 For this reason, emphysematous cholecystitis is common in people with high blood pressure because this arteriopathology can lead to vascular insufficiency of the gallbladder. 2 This condition is five times more likely to be seen in men, and as many as half of all cases of emphysematous cholecystitis are seen in patients with diabetes mellitus. 7
While emphysematous cholecystitis is an uncommon condition, it is also a life-threatening one in which swift detection and treatment are important. While CT is the most sensitive imaging modality for diagnosing emphysematous cholecystitis, patients often present with very vague symptoms such as right upper quadrant pain, a symptom typically warranting initial sonographic examination, as it is impractical to perform a CT on any and/or all patients who present with these vague symptoms. 4 The typical sonographic features of emphysematous cholecystitis include visualization of gas within the gallbladder lumen, which appears as a bright echo along the anterior gallbladder wall that causes ring-down or comet-tail artifact directly posterior. 1 Emphysematous cholecystitis typically presents on CT examination as irregular thickening of the gallbladder wall, hypodense foci indicating gallstones, and the presence of air within the biliary tree appreciable as branching regions of air density within the liver. 2 When a sonographic examination is positive for emphysematous cholecystitis, it should be followed by an abdominal CT, which can demonstrate and determine the exact location of air within the gallbladder itself and the biliary system, findings used to stage the condition.5,6
Once diagnosed, this condition is graded or staged based on the distribution of air within the gallbladder and/or biliary system. 2 The condition is said to be in stage one if the air is contained within the gallbladder lumen, stage two if air is in the gallbladder wall, and stage three if the air is seen within the pericholecystic tissue. 2 Because of the high incidence of complications associated with emphysematous cholecystitis, emergency cholecystectomy is the typical treatment. However, surgery is contraindicated in some patients, in which case, alternative treatment options may include intraveneous administration of broad-spectrum antibiotics or percutaneous drainage of the gallbladder via a cholecystostomy tube. 2
The prognosis for emphysematous cholecystitis depends on the stage of the condition at diagnosis. 2 Detection of this condition in stage one has the best prognosis because interventional treatment can be performed prior to complications such as gallbladder wall gangrene and perforation, which can be fatal. 6 The mortality rate for emphysematous cholecystitis is as high as 15% to 20% because of increased incidence of gallbladder wall gangrene and perforation, but early diagnosis and treatment can drastically improve patient outcomes. 5 Sonography and CT have been found to be diagnostically favorable as they have a sensitivity of up to 95% for detection of emphysematous cholecystitis. 2 Sonography offers the most cost-effective and noninvasive imaging approach to detect emphysematous cholecystitis and allows for prompt management. Early detection of this condition significantly lowers the incidence of complications and thus improves patient prognosis.
Conclusion
Emphysematous cholecystitis is a rare yet life-threatening condition that when detected early improves morbidity and mortality rates. Sonography can be utilized as a rapid, noninvasive imaging modality to examine the gallbladder and biliary tree to detect the presence of air within the biliary system and confirm the diagnosis of emphysematous cholecystitis. In the case presented, sonography was used in conjunction with CT to confirm the diagnosis and determine that it was stage three, as air was visualized within the common bile duct. 2 Rapid, accurate diagnosis and staging via sonographic and CT examination allowed for swift treatment, as aggressive as the patient’s comorbidities allowed, via broad-spectrum antibiotics before complications such as gallbladder wall gangrene and perforation occurred. Prompt detection and diagnosis of this condition has been shown to significantly improve patient outcomes and prognosis by allowing appropriate interventional treatment to be done prior to the occurrence of complications that can be fatal.
Footnotes
Acknowledgements
The authors would like to thank Dominique Buckley, RDMS, and the University of Missouri Diagnostic Medical Ultrasound staff for their invaluable assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.