
Abstract
Pilonidal cysts are collections of hair or skin debris located most commonly on or near the natal cleft of the buttocks. These cysts can become infected and cause swelling and bleeding at the site. Once infected, the condition is then termed a pilonidal abscess, and treatment should be followed. Several options are available for treating a pilonidal abscess, depending on the extent of the condition and the patient’s response to antibiotic therapy. This case study of a pilonidal abscess demonstrates the important information that sonography adds to the diagnosis and treatment of this condition.
Pilonidal cysts can present between the digits in the hands or feet but are often found on or around the natal cleft. 1 These cystic collections are usually seen in men between the ages of 16 and 24. 2 In 2004, there were 2604 cases of pilonidal cysts reported in U.S. hospitals. 3 Abscess formation is a possible result of pilonidal cyst infection. Sonography is an important diagnostic tool that is able to visualize superficial structures and can be more cost effective than other imaging modalities. Hand-held sonography provides the freedom to image in whatever plane is necessary at the level above the coccyx and for evaluating a pilonidal cyst.
Case Study
A teenage girl presented to the emergency department after noticing a bleeding wound around her coccyx. The patient reported sudden bleeding and tenderness to the area of inflammation but could not recall any trauma sustained at the site that would have caused the wound. Upon physical examination, a small opening was found at the site with persistent bleeding. Manual compression was performed in an attempt to drain what was assumed to be a fluid collection, but this maneuver yielded no results. The emergency department determined that a sonogram would be the next best step in order to assess the wound.
The soft tissue sonogram was performed using gray-scale, color, and pulsed-wave Doppler on a GE Logiq E9 (GE Healthcare, Milwaukee, WI, USA). The linear ML 6-15 probe was used to image the area, and sterile gel was applied to the area of inflammation. Sagittal images revealed a complex mass measuring 2.97 cm in greatest length (Figure 1). Using color Doppler, the structure appeared to have vascularity (Figure 2). Pulsed-wave Doppler revealed low resistance, arterial blood flow within and surrounding the mass (Figure 3). The interpreting physician described the collection as having decreased echogenicity with edema and hyperemia noted overlying the coccyx in the superficial soft tissues of the back. No focal fluid collection was seen (Figure 4). Skin thickening was considered an accessory finding. The diagnosis was cellulitis with a phlegmon formation, and no drainable abscess was visualized.

Longitudinal image of the mid tailbone showing the greatest length of the sinus.
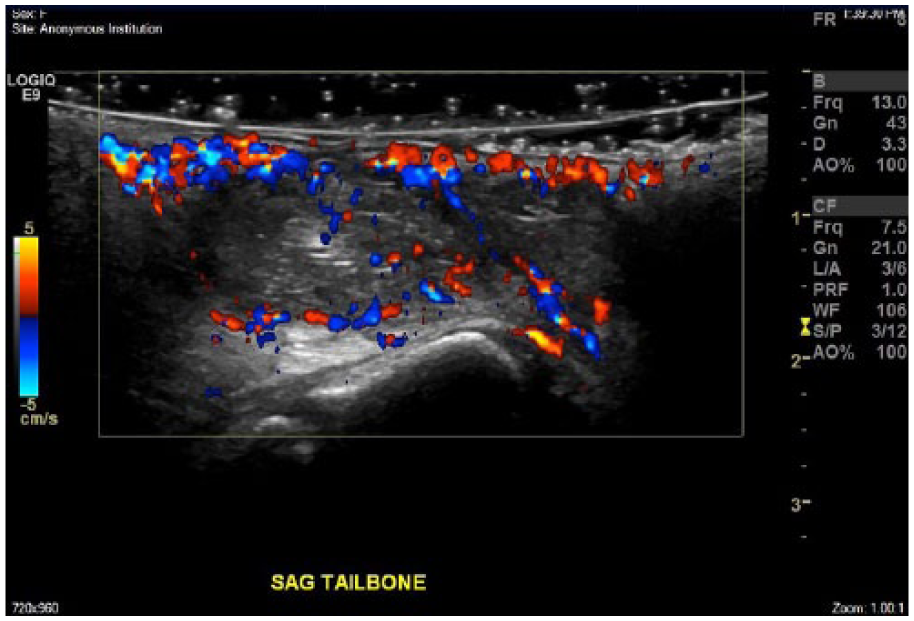
Longitudinal image of the mid tailbone with color Doppler displaying flow within the structure.
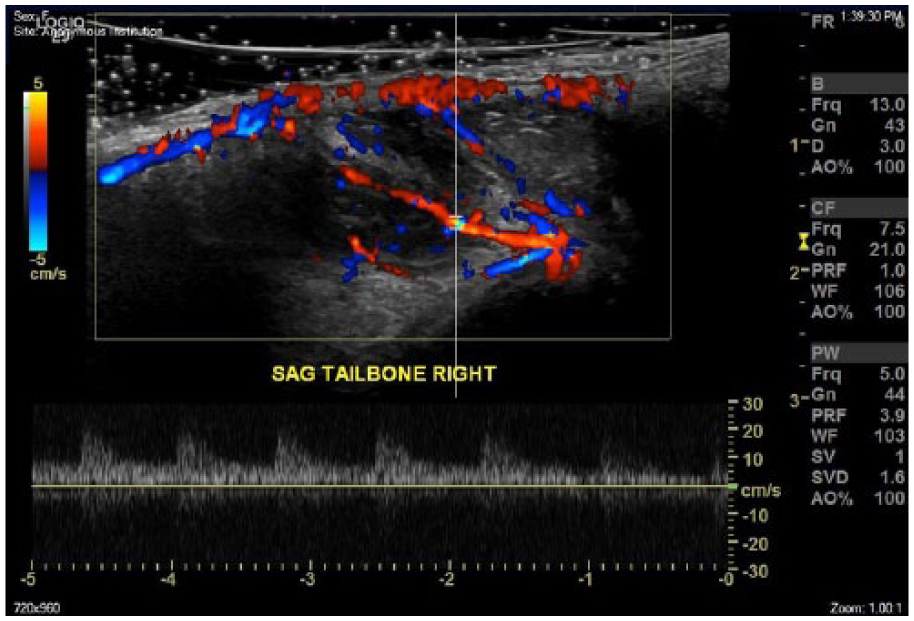
Longitudinal image of the tailbone with color and spectral Doppler revealing a low resistance waveform.
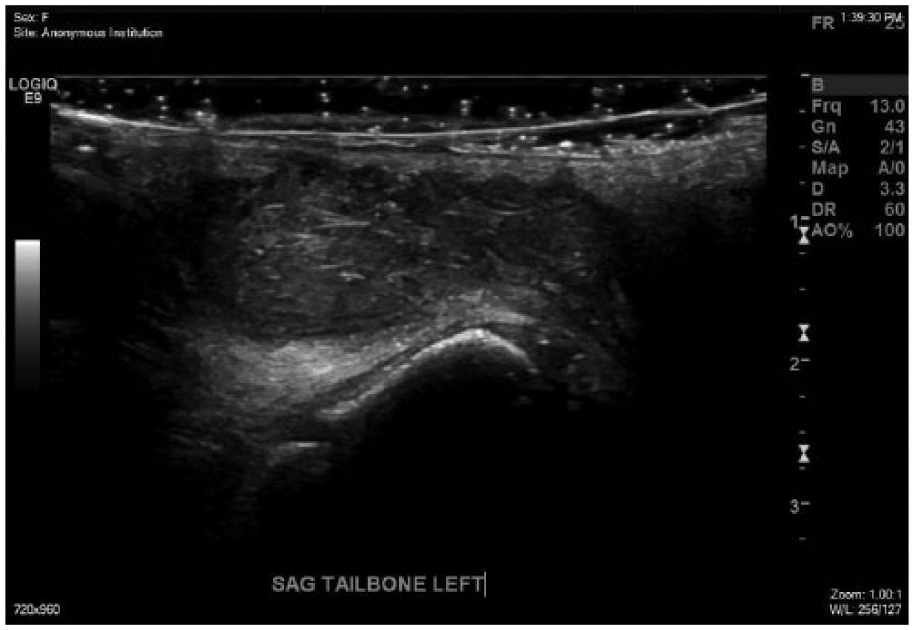
Longitudinal image of the tailbone showing a complex collection without any noticeable cystic areas.
No other examinations or procedures were ordered during the initial visit. The patient was diagnosed with cellulitis, prescribed antibiotics as treatment, and instructed to report to the emergency department the next day for follow-up wound care. At follow-up visit, there were no signs of a worsening condition, so the patient was released and advised to continue antibiotic therapy.
Discussion
Pilonidal cyst, also referred to as a pilonidal sinus, is defined as a fistula or pit in the sacral region, communicating with the exterior, containing loose broken-off hairs that may act as a foreign body producing inflammation. 4 The opening to the sinus appears as a small dimpling of the skin with possible leakage of bloody fluids. The most common site of infection is the natal cleft, but this infection has also been seen in areas such as the clitoris or interdigitally on the hands or feet.1,5 Once the sinus becomes inflamed, is may be referred to as a pilonidal abscess and will require treatment. 6 The infection and resulting inflammation causes painful swelling and chronic drainage of pus from the open wound. Pilonidal cysts usually present between the ages of 16 and 24 and are often reported among patients who are hairdressers or dog groomers. This entity was once considered a very common disease among men in the armed services during World War II. 1 The men would endure long bumpy car rides that could result in an infection at the natal cleft. It was for this reason that pilonidal cysts were nicknamed “jeep disease.” 7 Though it is most often caused by trauma endured after birth, pilonidal cyst can occur prenatally and is a cause of elevated AFP and acetylcholinerase. 8
There are many different forms of treatment for pilonidal abscess. If drainage or antibiotic therapy does not eliminate the disease, surgical options are available to remove the collection. These treatments range from skin flap coverage, such as a fasciocutaneous V-Y advancement flap, to minimally invasive, or scarless, ablation. The ability to perform this minimally invasive procedure in an outpatient facility makes pilonidal sinus ablation an optimal choice over other surgical options. 9 Several studies have been performed on the different treatment options, but no definitive conclusion has been reported.10,11 While some procedures, for instance the V-Y flap or the Limberg flap, claim to have a reduced risk of recurrence, there is still a chance that the natal cleft may become infected again. 10 In a study of 45 fasciocutaneous V-Y advancement flap procedure recipients, the 25-month clinical follow-up showed no signs of recurring pilonidal sinus infection. 10 The risk of recurrence is as high as 40% but can be reduced by early treatment. The treatment options that flatten the natal cleft halve the recurrence rate. 6
Sonography is a useful tool for imaging superficial structures and has an application for this pathologic condition. The utilization of a high frequency linear probe is optimal when performing a soft tissue exam of the natal cleft. Sonography provides color and pulsed-wave Doppler as well as gray-scale images of the affected site. Other imaging modalities that could be utilized include magnetic resonance imaging (MRI) and computed tomography (CT). These tests are both useful for determining size and location of masses and do not involve applying gel or pressure to the affected site. The advantage of performing a CT or MRI as opposed to sonography for evaluating a pilonidal cyst is the ability to image inferior to mass. The location of the sinus can restrict the sonographer’s ability to image the structure due to its proximity to the gluteal muscles that limits transducer accessibility. Though MRI is fully capable of imaging soft tissue structures, the exam requires a longer amount of time to complete than other modalities. Both CT and MRI are optimally performed with the patient supine, which can apply pressure to the affected area with subsequent pain. While the exams can be performed with the patient prone, the position may result in poor images and an increase in patient prep time.
Since pilonidal cysts form directly under the skin, there are a few techniques that should be utilized when scanning in that region. An important factor for every exam is choosing the correct transducer to best display the area of interest. A high frequency transducer is optimal for imaging structures near the skin surface. Sterile gel is not a necessity for imaging a pilonidal sinus but is recommended due to the open condition of the skin. A stand-off pad is helpful but not essential. An increase in the amount of gel will suffice for visualization. Harmonic imaging may help improve the image as well as increase the frequency and the amount of focal zones.8,12
Sonographically, a pilonidal cyst appears as a complex mass located just superior to the sacrum. The depth of the mass is usually less than 4 cm, and the length is variable depending on the spread of infection. The inflammation of the tissue causes the area around the mass to appear vascular under color Doppler interrogation. During the soft tissue sonogram, it is important to document the area affected in transverse and sagittal with and without measurements. Other images that should be included in the study are color Doppler pictures of the mass as well as superior and inferior pictures of the area. Due to the location of the sinus, the inferior area may be difficult to visualize.
Though other imaging modalities, such as MRI, are sufficient to visualize superficial structures, sonography is more time efficient and cost effective. The sonographer scanning should have a basic knowledge of the disease and a consistent scanning protocol. The protocol for a pilonidal cyst should be concise and include enough images for a clear diagnosis. Sonography is important in the diagnosis and treatment of pilonidal cyst.
Differential diagnoses include but are not limited to phlegmon or sacrococcygeal teratoma. A phlegmon is an acute inflammatory process that produces pus and occurs within the subcutaneous collective tissue. 13 A sacrococcygeal teratoma is a fetal neoplasm with a high perinatal morbidity and mortality rate. 14 The location of the mass and age of onset are important factors when diagnosing this condition. Sacrococcygeal teratomas share some similarities with pilonidal cysts, such as location and vascularity, but sacrococcygeal teratomas are vascular throughout the entire mass and are typically diagnosed prenatally. 15 Phlegmon are not specific to the natal cleft and do not create a dimpling in the skin like a pilonidal cyst. All of these pathologies are drainable, but only the pilonidal cyst is likely to contain foreign debris and hair.
Conclusion
There is a chance of recurrence with this condition, so proper patient counseling and care should be taken to reduce the risk of recurrence. Occupations that involve the treatment or cutting of hair are a risk factor for developing a pilonidal sinus. Care should be taken by the patient to refrain from actions that could cause recurrence, such as trauma to the tailbone. Sonography is not the only modality available for imaging this disease but is efficient and easily accessible, which makes it an effective choice. Though treatment options are plentiful and no studies agree on what the best option is, they do share similarities. 16 Common points between previous studies include the alleviation of the patient’s symptoms after the procedure and the chance of recurrence. There are a few other conditions that may appear similar to pilonidal cyst, but the location of the infection and the age of onset help determine the correct diagnosis.
Footnotes
Acknowledgements
The author would like to thank Lynn Schluns, RDMS, RVT, and Wendy Allen, RDMS, RVT, at El Centro College for their help and support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.