
Abstract
Decidualized endometriosis is a benign condition associated with ectopic endometrial tissue that has undergone a decidual reaction during pregnancy. A case is presented of a 31-year-old female who presented to an imaging center for a follow-up sonogram after experiencing one episode of vaginal bleeding during pregnancy. A solid, highly vascular mass, with irregular borders, was seen that was not present in the sonogram two weeks prior. The mass was later revealed to be decidualized endometriosis. This is a rare condition that lacks extensive reporting in the literature. The case demonstrates a particularly odd location for this disease, in between the uterus and bladder. With multiple sonograms, it was difficult to ascertain the host of the mass. Due to the extent of vascularity within this structure, malignancy had to be considered, which led to a referral for additional testing.
Keywords
Delineating between uterine tissue, ovarian tissue, and other pelvic structures during a sonographic examination is a challenge that requires education, skill, and clinical judgment. During the course of pregnancy, this process of clinical problem solving, while scanning, can be very difficult. With an influx of hormones, there is expansion of the uterus, development of new tissue, and an inflow of increased vascularity, which accompanies the developing fetus. In nongravid studies of the pelvis, the uterus and ovaries are subject to a variety of pathologies both benign and malignant. At times, some of these abnormalities can mimic each other, making their respective diagnoses a difficult task. During an anatomical evaluation of the fetus throughout the stages of pregnancy, the focus is primarily on the development of the fetus. While the uterine and ovarian structures are routinely evaluated, they often become obscured as the fetus develops and the uterus expands. Yet, it is important for sonographers to make every attempt to survey the pelvis in its entirety. Multiple solid, cystic, and complex structures may emerge, which require sonographers to bring attention to interpreting radiologists and other health care providers. A case is presented, which describes the sonographic presentation (using gray scale, color, and spectral Doppler) of decidualized endometriosis with differential diagnoses.
Case Study
A 31-year-old female, gravida 1, para 0, at 8 weeks gestational age, presented to reassess viability after an episode of vaginal bleeding. During this follow-up study, the patient did not report being symptomatic for pain. Two weeks earlier on a sonogram, the results demonstrated a small size/dates discrepancy. Other than Hashimoto’s thyroiditis, the patient’s chart review did not identify any other past medical history. An exam was completed with General Electric Voluson E8 Expert equipment (GE Healthcare, Wauwatosa, WI). For additional images, an exam was done with General Electric Logiq E9 equipment. A 4C-RS curvilinear 2.0–5.5 MHz transducer was used to obtain transabdominal images, and an E8C-RS intercavity 4.0–10.0 MHz transducer was used for transvaginal images.
The eight-week sonogram demonstrated a normal fundal intrauterine gestation, with a new 4.0 × 2.4 × 4.0 cm solid mass in the anterior lower uterine segment (Figures 1–3). The mass bulged anteriorly into the posterior wall of the urinary bladder (Figure 1). The borders were irregular, and innumerable punctate echogenic foci were distributed throughout the solid mass. The addition of color Doppler demonstrated a richly vascularized mass, with large volumes of venous flow and highly resistive arterial flow (Figure 4). Normal ovaries were demonstrated. No high volume, high velocity, low resistive arterial flow, or arteriovenous shunting was identified in the spectral Doppler patterns (Figure 5–6).
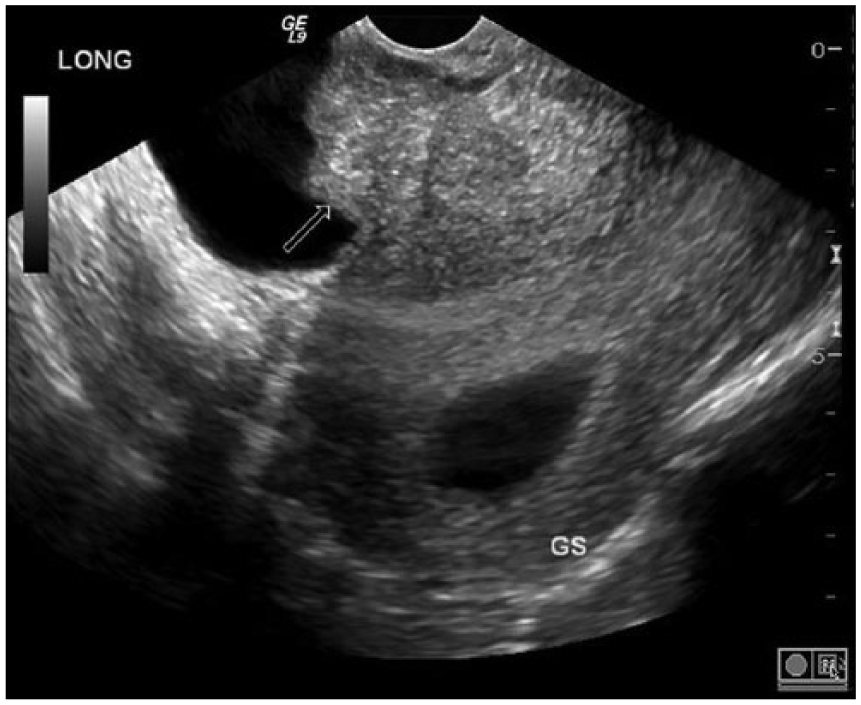
This transvaginal images demonstrates a sagittal view of the uterus, posterior to the bladder, with a solid structure (arrow) protruding into the bladder.
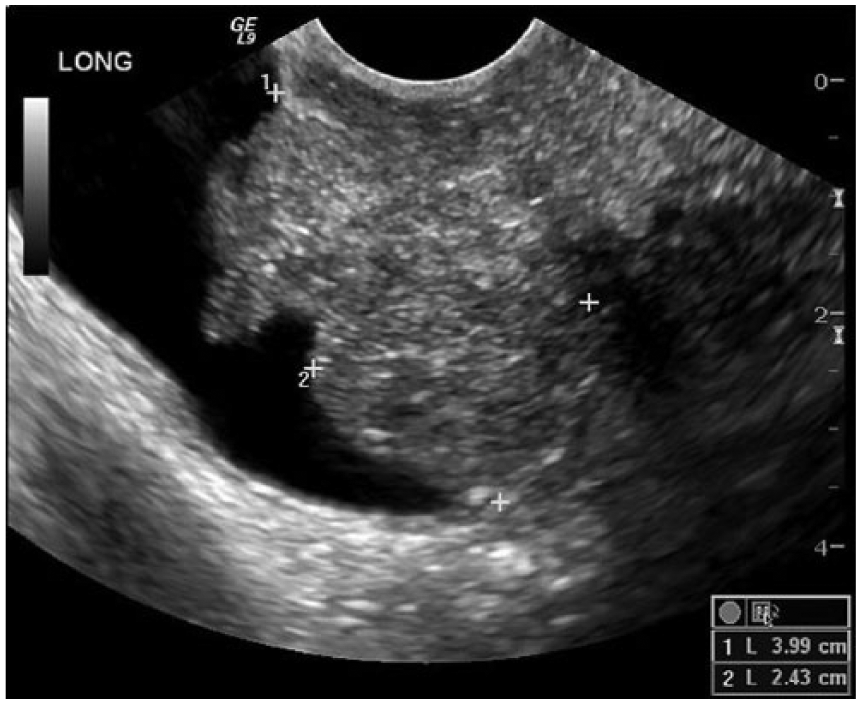
This image represents a sagittal view of the mass with measurements. Innumerable punctate echogenic foci are distributed throughout the mass.
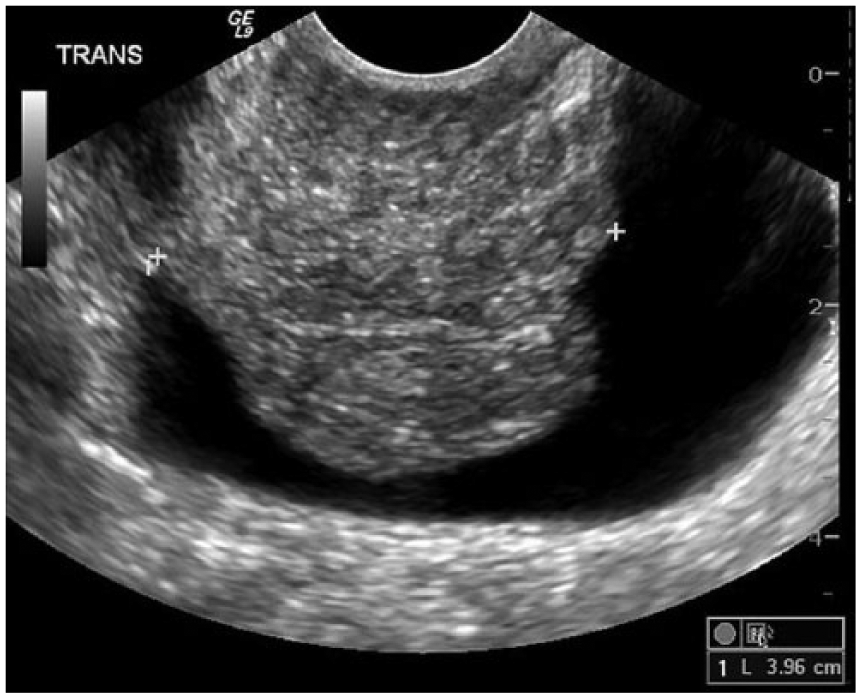
This image represents a transverse view of the mass with measurements.
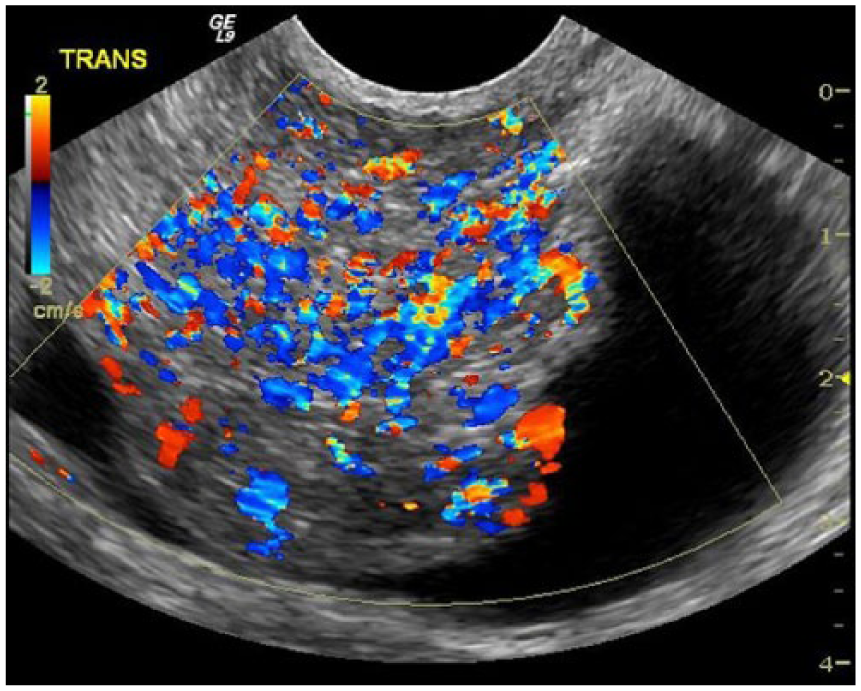
This image represents a transverse image of the mass with color Doppler demonstrating a rich network of vascular channels.
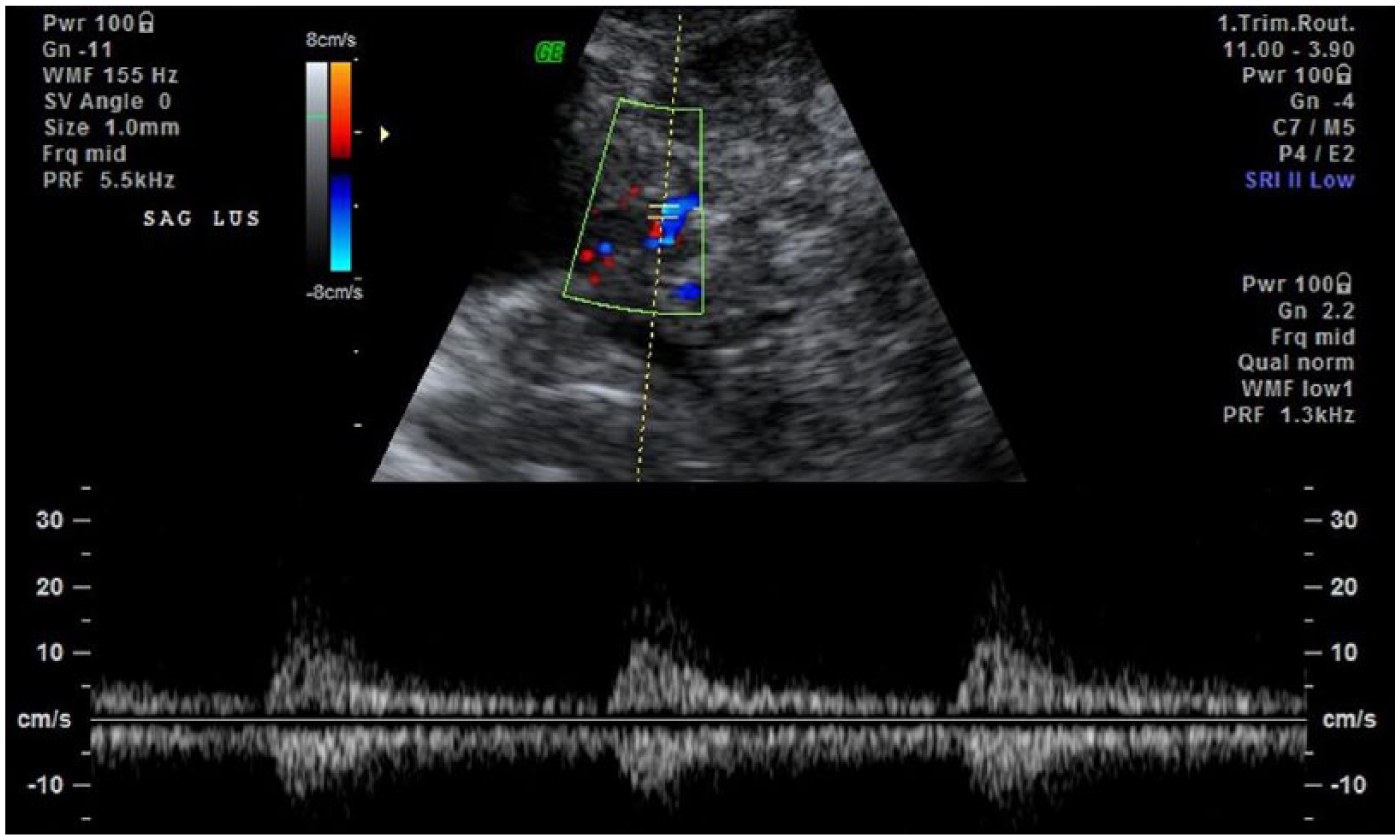
This image demonstrates low resistive arterial blood flow using spectral Doppler analysis.
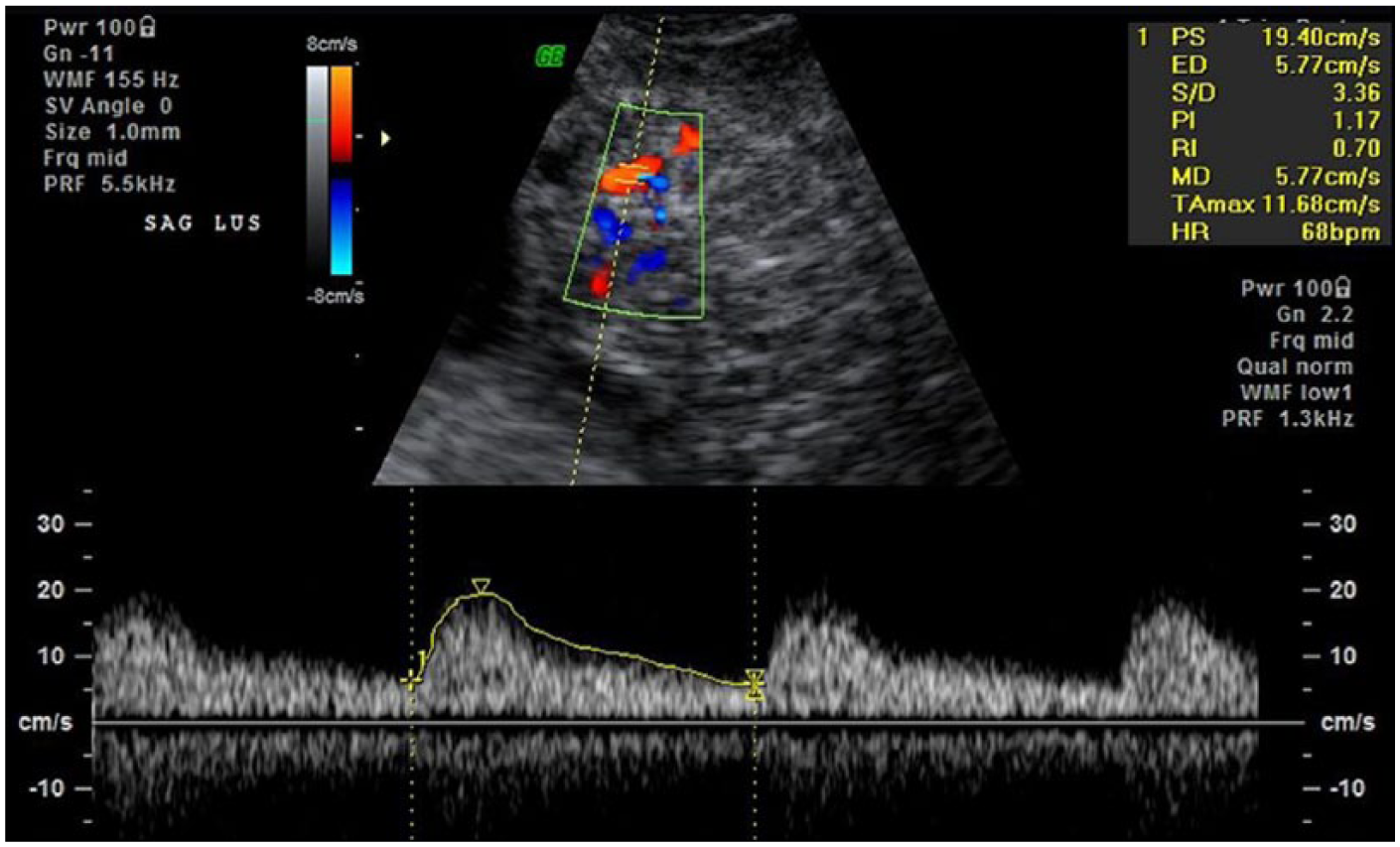
This image demonstrates a pulsatility index (PI) = 1.17 and a resistive index (RI) = 0.70.
Transabdominal and transvaginal sonograms demonstrated preservation of normal endocervical canal without connection between the mass and the decidual tissue of the fundal gestational sac. Use of a transvaginal probe to apply pressure to the cervix was neither effective in separating the mass from the cervix, nor from the urinary bladder. In the patient’s laboratory work, there was no hematuria present. Serial quantitative hCG values were not inordinately elevated to suggest gestational trophoblastic disease (GTD).
Sonography was indefinite as to the anatomical site of the origin for this mass of rapid onset. Possibilities included anterior cervical stroma in the extraperitoneal cervicovesicle space, and the bladder wall and/or bladder mucosa. Decidualized endometriosis was reported as the preferred differential diagnosis over cervical or bladder cancer given the absence of the mass on the 6-week sonogram. Nonetheless, malignancy could not be excluded, based on imaging evidence. The patient then underwent diagnostic cystoscopic biopsy, which demonstrated decidualized endometriosis. The pregnancy proceeded uneventfully. Follow-up studies demonstrated persistent soft tissue fullness between cervix and bladder with diminution of discrete border margins. The patient returned to the imaging center on 2 separate occasions at 14 weeks and again at 18 weeks. Both follow-up sonograms demonstrated normal fetal biometry and an uneventful pregnancy.
While there were several differentials to consider, there were key characteristics in this case study, which led to the ultimate diagnosis. The rapid development of this structure, which was not seen two weeks prior, was a clinical concern. This is characteristic of decidualized endometriosis. While this was also suspicious for either GTD, or a rapid-onset malignancy, there was no indication of these differentials in the patient’s lab findings. In addition, the lack of high volume, high velocity, and low resistive arterial flow within the vascular channels of this mass minimized the probability of malignancy. The location of the mass, anterior to the uterus pressing posteriorly against the urinary bladder, looked somewhat suspicious for a uterine fibroid. Yet, the heterogeneity and hypervascular sonographic appearance gave this structure a unique distinction that was different from typical uterine fibroids (Figure 4).
Discussion
Decidualization is a process in which the endometrial tissue is converted into a specialized lining adequate for development of the gestation in a newly gravid uterus.1–6 This change occurs in early stages of pregnancy due to increased estrogen and progesterone.1,7 The process involves hypertrophy of the endometrial stroma cells, which leads to the development of the decidua from nongravid endometrial tissue. 3 Ectopic decidualized tissue can often go undetected during a sonographic exam. Yet, when they appear, most commonly in the ovaries, these rapid-growing endometriomas have a very deleterious appearance that can easily mimic malignant structures. 1
Decidualized endometriomas have been documented on sonography by a characteristic “ground glass” appearance.1,4 It presents as a solid mass that has growing intracystic vegetations. 1 With the use of color Doppler, it can demonstrate an intensely rich network of vascularity. When spectral Doppler is incorporated into these vascular channels, resistive indices (RI) can be demonstrated within the range of 0.37–0.55.2,3 However, the accuracy of spectral Doppler is somewhat miscellaneous. Jeong et al. 8 reported a sensitivity of 50–100% and a specificity of 46–100%. Therefore, this is not necessarily a finding that would sway an interpreting physician from following up with additional testing. In the context of a solid, rapidly expanding mass, no Doppler indices could be so definitive.
One of the great challenges associated with decidualized endometriosis is that its rapid development is highly suspicious for malignancy. This rapid growth is linked to the hormonal environment that leads to the development of rapid changes within the endometrial canal during the transformation to the decidua in the gravid patient. 3 A diagnostic challenge emerges when decidualized endometriomas present during pregnancy due to their rapid growth and highly vascularized appearance. 2 Whereas a mass with little to no arterial or venous flow would not be so concerning, the abundance of vasculature warrants further evaluation. The type of invasive procedures, that can be required if malignancy is expected, can sometimes lead to early termination of pregnancy. 1
Differentials of decidualized endometriomas can include exophytic leiomyomas, GTD, and malignancies. Leiomyomas are the most common benign tumors seen in the uterus for women of childbearing age. 9 While some vascularity within leiomyomas is common, the detection of hypervascularity may be suspicious for leiomyosarcoma. 10 Yet, in the literature there is not a known prevalence of these malignancies growing so rapidly when compared with decidualized endometriomas. GTD is an abnormal condition that can be seen during pregnancy. This condition is characterized when healthy trophoblastic tissue, arising from the placenta, invades the endometrium.11,12 Similar to decidualized endometriosis, GTD may ultimately present as a hypervascular mass within the uterus. Its key characteristics include a significant rise in human chorionic gonadotrophin (hCG). A rapidly formed mass in the pelvis could point to this potential diagnosis. However, this rise in hCG levels, along with early vaginal bleeding, should differentiate this condition from decidualized endometriosis. 12 Endometrial carcinoma can also present as a vascularized mass seen within the endometrium. Sonographically, endometrial measurements of > 5mm in postmenopausal women can be suspicious for endometrial carcinoma. 13 This is a disease most typical of older, postmenopausal women. 14 Therefore, it is usually not the first diagnosis to consider when evaluating the sonogram of a young, pregnant patient. While decidualized endometriosis may appear sonographically similar to endometrial carcinoma, its location is of great consideration.
Decidualized endometriosis is a rare, yet benign condition. It is an extremely rapid-growing mass, which may lead sonographers and interpreting physicians to be concerned about malignancy. Its irregular appearance, with many vascular channels may further support the concern for malignancy. Therefore it is important to document these masses in multiple scanning planes, and use color or power Doppler to demonstrate the vascular channels. In many cases radiologists may choose to refer to other diagnostic testing to further exclude the possibility of malignancy.
Conclusion
The importance of this case, with regard to the field of sonography, is that sonograms are an essential first line of detection of this complex-appearing pelvic mass. From the perspective of sonographers, awareness of decidulized endometriosis is the first step in its detection as it is a very rare occurrence. Recognition of key characteristics, such as the “ground glass” appearance presenting with intracystic excrescences, abundance of vascular activity, and rapid growth, can help in its detection.1,4 In addition, the literature has demonstrated that these lesions are most often unilateral and, unlike many malignancies, they do not typically present with free fluid. 2 Communication between sonographers and the interpreting physician is germane to its ultimate diagnosis. Attention to sonographic detail and patient history that is salient to the best patient care practices.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.