
Abstract
Objective:
The aim of this review was to provide a summary of literature and research on the use of elastography and its effectiveness in diagnosing endometrial pathology.
Materials and Methods:
An online database search produced 16 research articles. Inclusion criteria consisted of ultrasound elastography of benign and malignant endometrial pathology. Priority was given to articles focused on endometrial hyperplasia, polyps, and endometrial carcinoma.
Results:
The difference in stiffness between endometrial carcinoma and benign endometrial pathology, including lesions and hyperplasia, is statistically significant. High rates of sensitivity and specificity are seen in using elastography to determine endometrial carcinoma from a benign endometrial pathology.
Conclusion:
Elastography can provide valuable information to aid in diagnosing endometrial carcinoma. Currently, the standard of care for diagnosing endometrial pathology is 2D ultrasound imaging with tissue sampling and histology. Elastography imaging of the endometrium offers the opportunity to diagnose endometrial pathology without invasive tissue sampling procedures. While this exciting development offers great potential, there must be universal, consistent approaches and studies of subgroups to be considered the standard of care.
Ultrasound elastography measures the stiffness, or elasticity, of tissue by monitoring the response of tissue to acoustic energy.1 –3 When subjected to the same force, softer tissue has more strain than stiffer tissue. 3 Elastography allows for the quantification of tissue properties and can be used in conjunction with conventional sonographic techniques, in the characterization of tissue. 2
Elastography is divided into two methods, strain imaging and shear wave imaging. 1 –3 The strain ratio is measured by targeting a region of interest and comparing it to adjacent normal tissue before and after freehand transducer compression.2,4 In strain elastography, compressive strain is lower in stiffer tissue. 2 Strain wave elastography results are reported as strain ratios, the ratio of the sampled tissue to normal adjacent tissue. 5 Strain elastography comes with some limitations that must be taken into consideration. Strain imaging requires artificial or manual compression, which cannot be quantified, to displace tissue.3,4 Strain imaging is also limited in imaging deep tissue with respect to the transducer that cannot be manually compressed. 4 This makes strain elastography considerably more user-dependent than shear wave elastography.3,4
Shear wave elastography displaces tissue using dynamic, acoustic forces generated by the ultrasound system and is less user-dependent than strain imaging.3,4 The shear wave velocity can qualitatively and quantitatively estimate tissue stiffness. 4 The velocity of the shear wave in the region of interest is converted, and the stiffness of the tissue is reported as E mean and E max values measured in kilopascals (kPa).4,6 Shear wave imaging has the benefit of being able to access and image deeper tissues, up to 8 cm from the transducer, making it more suitable for obstetrics and gynecologic (OB/Gyn) imaging. 4
For the past 2 decades, elastography has gained ground in the detection and diagnosis of disease in other organs. These include fibrosis evaluation, staging, and diagnosis of liver and renal diseases. 1 Elastography is also used to distinguish between benign and malignant breast and thyroid lesions, lymph node malignancies, and inflammatory bowel disease.1,2 Studies are also emerging on the use of elastography in gynecology and musculoskeletal disease. Research in endometrial elastography is focused on the diagnosis of several common endometrial pathologies, including endometrial hyperplasia, benign endometrial polyps, and endometrial carcinoma.
Endometrial Hyperplasia
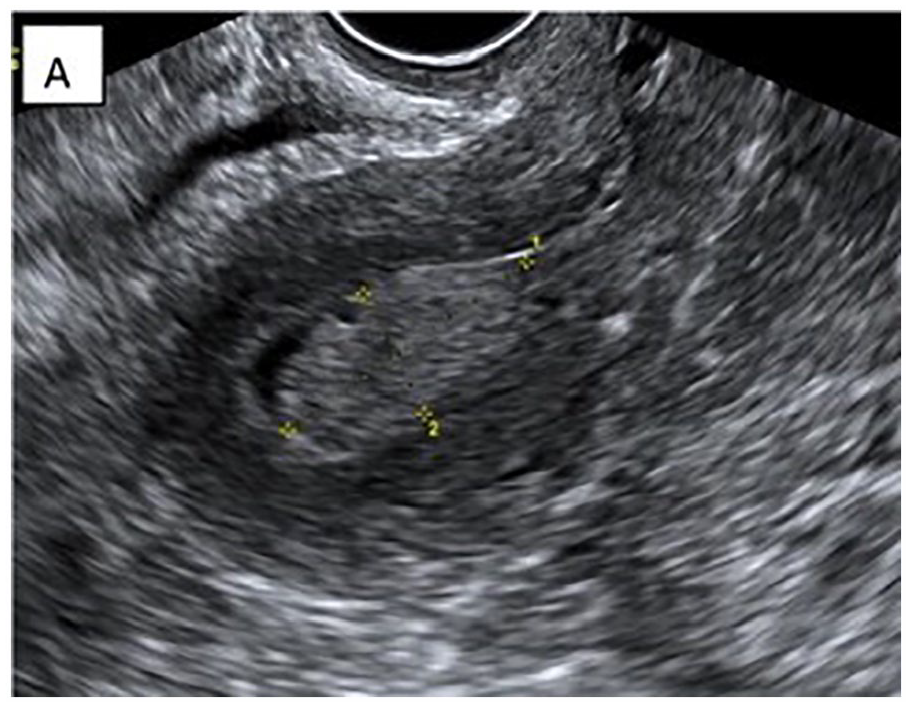
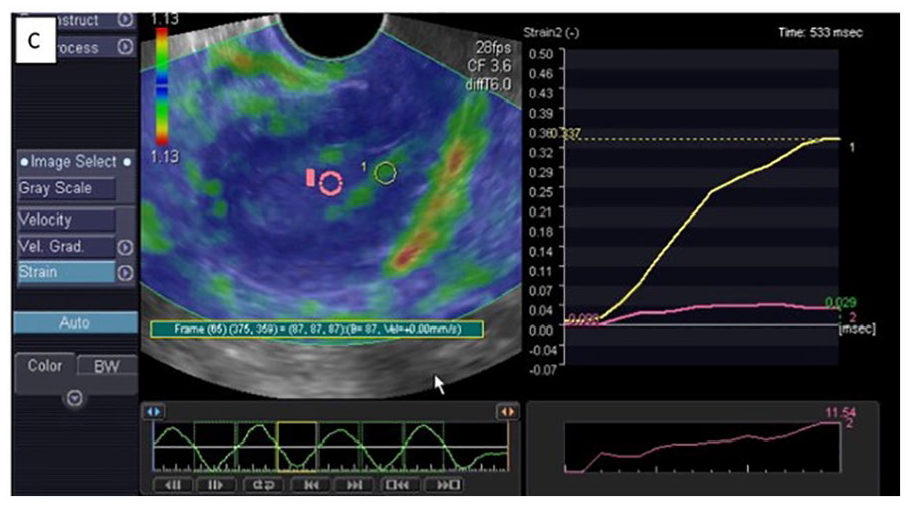
Endometrial hyperplasia (see Figure 1) is believed to occur from an excess of estrogen or the ratio of estrogen relative to progesterone. 7 The most common symptom of endometrial hyperplasia is abnormal uterine bleeding. 8 Endometrial hyperplasia is defined as an endometrium that diffusely or focally measures greater than 5 mm in postmenopausal women and greater than 10–16 mm (depending on the phase of the menstrual cycle) in premenopausal and perimenopausal women on transvaginal sonography. 9 The World Health Organization classifies endometrial hyperplasia into 4 categories, simple, complex, atypical simple, and atypical complex.10,11 Simple and complex endometrial hyperplasia are considered low risk for malignancy, whereas atypical endometrial hyperplasia is at higher risk for endometrial carcinoma. 7 Figure 2 demonstrates the sonographic characteristics of endometrial hyperplasia with elastography. Benign tissue is demonstrated with a similar strain index to normal myometrial tissue resulting in a lower strain ratio.
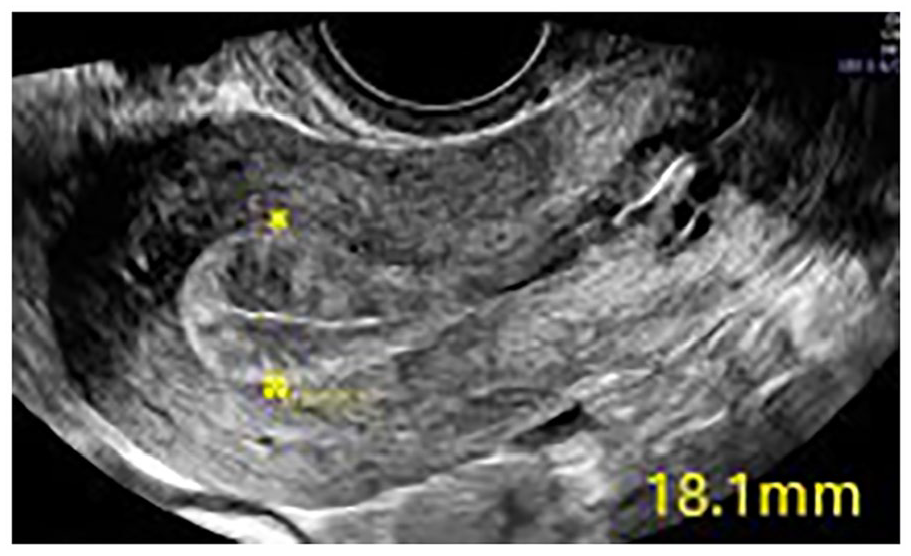
An example of endometrial hyperplasia, as seen on transvaginal sonogram (indicated with the yellow calipers).
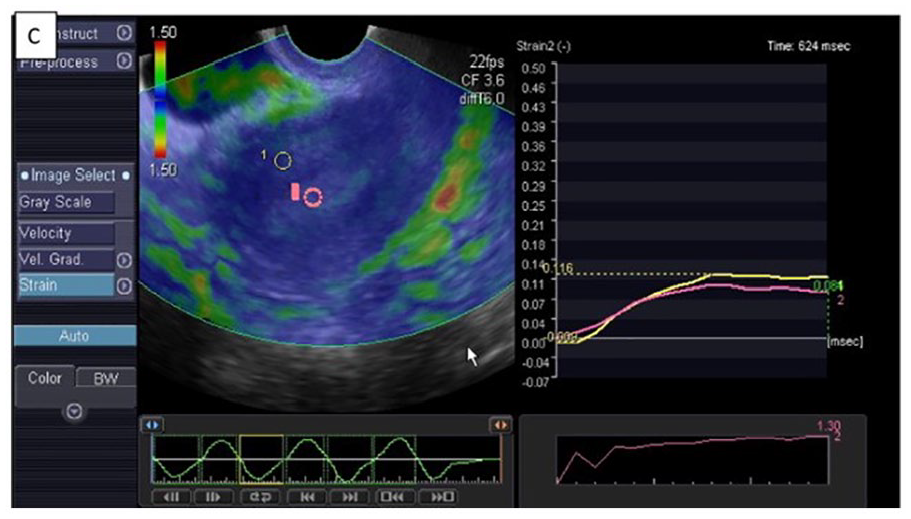
An example of endometrial strain elastography used in a case of endometrial hyperplasia. Endometrial elastography demonstrates a lower strain ratio of benign endometrial hyperplasia (pink) than normal myometrial tissue (yellow). Data adapted from the Egyptian Journal of Radiology and Nuclear Medicine. 12
Endometrial Polyps
Endometrial polyps are relatively common in premenopausal and postmenopausal women. 5 Endometrial polyp prevalence rates of 20% have been reported, with higher rates seen in women of reproductive age. 5 Endometrial polyps are caused by focal hyperplastic growth of endometrial glands, like endometrial hyperplasia, but result in a lesion extending into the endometrium (see Figure 3). Endometrial polyps are rarely malignant. 8 However, of the polyps that are diagnosed as malignant, they present a risk of more aggressive malignancies. 5 Figure 4 demonstrates the sonographic characteristics of a benign endometrial polyp with elastography. The strain index is similar in the polyp to that of the benign tissue resulting in a lower strain ratio.
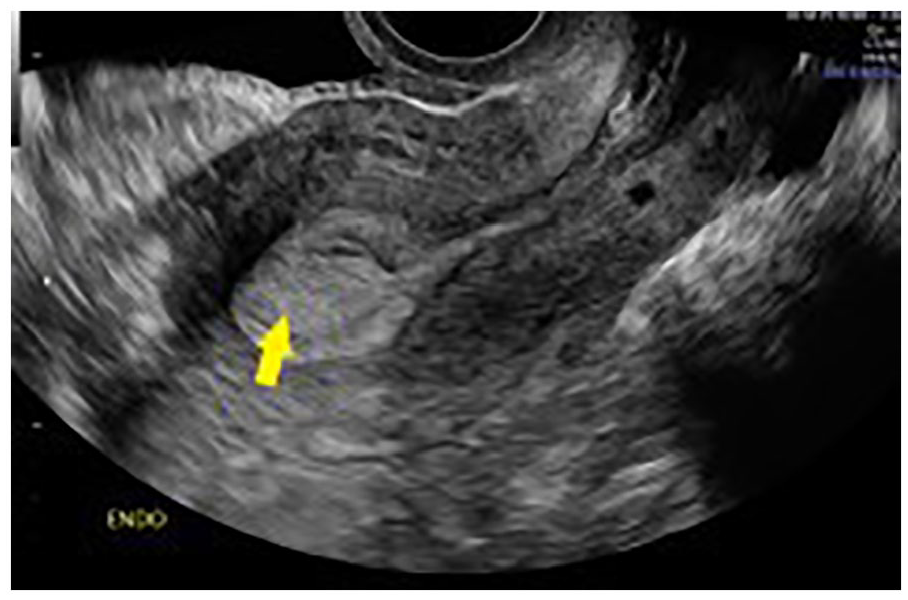
An example of an endometrial polyp, as seen on a transvaginal sonogram (indicated by the yellow arrow).
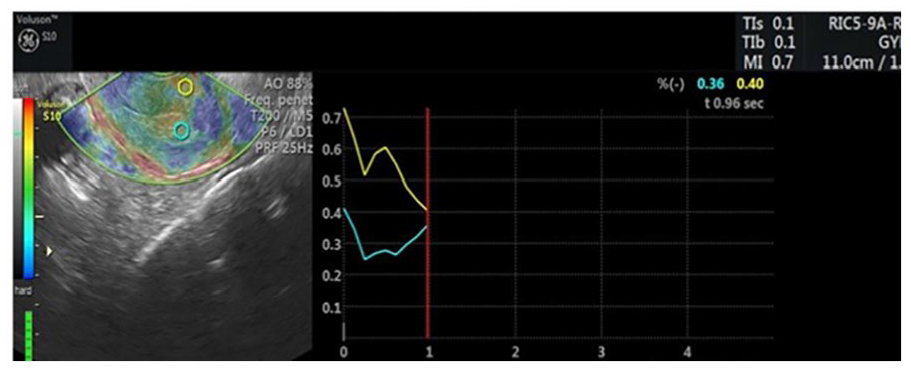
Endometrial strain elastography in the case of an endometrial polyp. Endometrial elastography demonstrates a lower strain ratio of a benign endometrial polyp (blue), compared to normal myometrial tissue (yellow). Data adapted from the WFUMB Ultrasound Open. 13
Endometrial Carcinoma
Endometrial carcinoma (see Figure 5) is the fourth most common malignant neoplasm in women after breast, lung, and colon cancers, occurring most frequently in postmenopausal women. 8 The most common symptom of endometrial carcinoma is abnormal uterine bleeding. 8 The exact cause of endometrial carcinoma is unknown, but several factors have been identified that put women at higher risk of developing endometrial carcinoma. 8 Estrogen therapy, early menarche, late menopause, obesity, chronic anovulation, history of infertility or nulliparity, diabetes, and ovarian cancer are all factors identified with a higher risk of endometrial carcinoma.8,11 There are currently no screening tests for endometrial carcinoma. 8 The current standard of diagnosis is imaging with transvaginal ultrasound with consequent hysteroscopy, endometrial sampling, or dilation and curettage with follow-up histopathology.4,7,8,9,11 Figure 6 demonstrates the sonographic characteristics of endometrial carcinoma with elastography. Malignant tissue is demonstrated with an increased strain index compared to normal myometrial tissue, resulting in a higher strain ratio.
A confirmed case of endometrial carcinoma as seen on a transvaginal sonogram (indicated by the placement of the electronic calipers). Data adapted from the Egyptian Journal of Radiology and Nuclear Medicine. 12
Endometrial strain elastography applied in a case of endometrial carcinoma. An endometrial elastogram demonstrates a high strain ratio of endometrial carcinoma (pink) compared to normal myometrial tissue (yellow). Data adapted from the Egyptian Journal of Radiology and Nuclear Medicine. 12
The purpose of this literature review was to explore the use of elastography in endometrial imaging. The aim was to evaluate the effectiveness of elastography and its potential to diagnose endometrial pathology, without the use of biopsy and histology.
Materials and Methods
Search Strategy
Research for this review was conducted using the University of Missouri library search engine, which includes PubMed, Medline, Clinical Key, Scopus, Wiley Online Library, and Science Direct databases. The author conducted the initial search on June 19, 2023, to include peer-reviewed articles published between 2013 and 2023. The initial keywords searched were ultrasound, elastography, and endometrium. Duplicates were automatically removed by the university search engine at the initial search. All searches and subsequent screenings were conducted by the primary author.
Selection Process
The initial search for this review began using the aforementioned search criteria and keywords ultrasound, elastography, and endometrium, resulting in 331 articles. A secondary search was conducted, eliminating 186 articles due to their involvement with MRI elastography. Seventy-nine articles were eliminated due to their focus on elastography of the cervix in pregnancy. This resulted in 66 titles and abstracts to be screened for inclusion. A total of 40 articles were eliminated due to their focus on elastography in anatomy other than the endometrium. The included 23 articles involved thyroid elastography, 12 involved liver elastography, and 5 involved breast elastography. The remaining 26 full-text articles were selected to be reviewed by the author. Of those 26 articles, 8 articles were eliminated due to their lack of elastography involvement, 4 were eliminated due to their focus on the study of elastography on uterine fibroids and adenomyosis, and 2 articles were not available in English. Twelve articles were included in this literature review.
A flow diagram is provided which illustrates the inclusion and exclusion processes (see Figure 7). The total number of articles included in the literature review was 12.
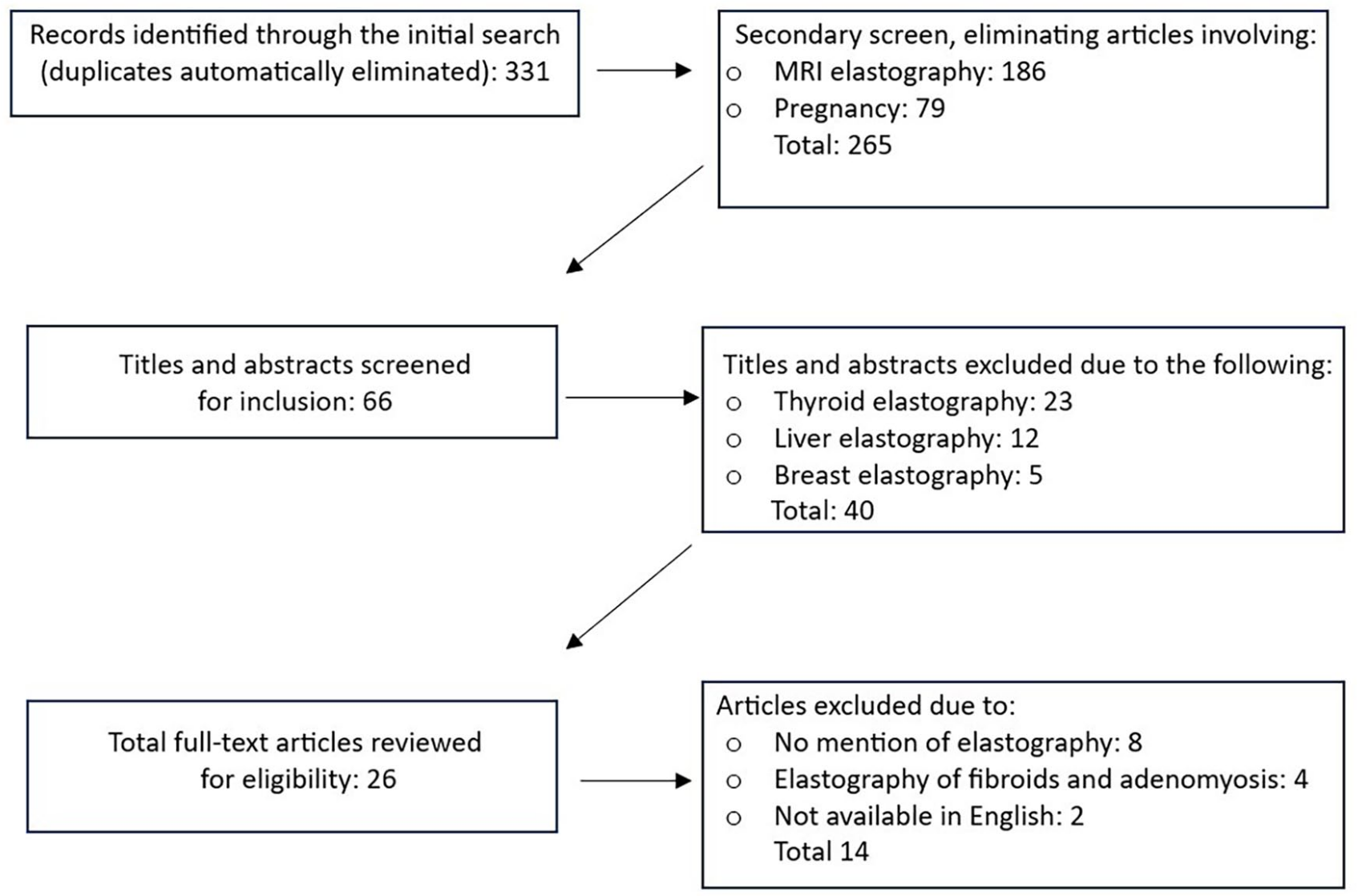
A flow diagram that demonstrates the inclusion and exclusion of peer-reviewed articles for this literature review.
Data Collection
Due to the small number of articles and the detailed study criteria of peer-reviewed articles involving endometrial elastography, the author screened each article for quality based on the study criteria and sample size. All articles were determined to be suitable for this literature review. The data were categorized by the use of shear wave and strain wave elastography. For each study, the specificity and sensitivity data were extracted and compared for shear wave and strain wave capabilities. For each study, the sample size, age, study criteria, and control group status were organized and compared.
Synthesis Methods
Due to the small number of sources for this review, all data were synthesized and charted by the author. Subgroup analysis was not possible due to the small number of articles available, and no data conversions were needed. For each source, the type of elastography was noted. Each study’s sensitivity and specificity data were collected and compared to their corresponding method of elastography. The study sample size, participant age range, study criteria, and use of control group data were extracted, compared, and displayed in tables. Study conclusions were compared to the specific type of elastography used (strain or shear wave).
Results
The results of all studies showed significant differences in the stiffness of benign and malignant tissue. Santos and Cristina, 13 Marfani et al., 14 and Abdel Latif et al., 12 using strain elastography, all found that endometrial hyperplasia and benign polyps produced strain ratios of 1–5 compared to strain ratios of 9–11 in endometrial carcinoma. Du et al. 15 and Ma et al., 6 using shear wave elastography, showed E mean values to be significantly lower in benign tissue with a range of 15.68 kpa–21.20 kpa compared to a range of 38.46 kpa–49.36 kpa in malignant tissue. These studies all showed that malignant tissue is significantly stiffer than benign tissue. Santos and Cristina, 13 Marfani et al., 14 and Gulketin et al. 5 included differentiations between benign endometrial polyps, endometrial hyperplasia, and endometrial carcinoma. However, Marfani et al. 14 and Gultekin et al. 5 both concluded that elastography was not helpful in discriminating between benign endometrial polyps and benign endometrial hyperplasia. See the tables provided for detailed results from the literature pulled.
Discussion
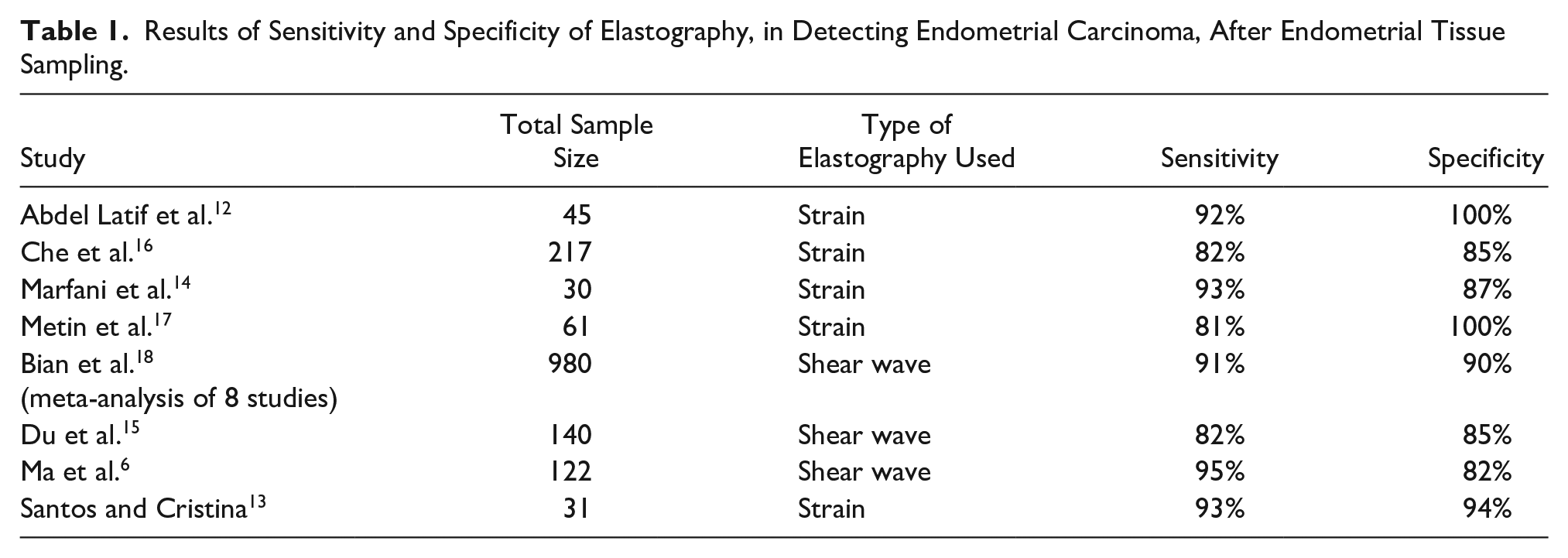
Elastography has not been heavily studied to determine the stiffness of endometrial carcinoma vs benign endometrial pathologies. The goal of each research article and the accessed literature review was to determine the accuracy of detecting endometrial carcinoma with the use of elastography. It appears that all studies conducted on women with increased endometrial thickness or endometrial lesions found statistically significant differences between the stiffness of endometrial carcinoma and benign endometrial pathology when using elastography (see Tables 1 and 2). In addition, all 10 original research studies reported that elastography was excellent in differentiating between endometrial carcinoma and endometrial hyperplasia. The studies included premenopausal and postmenopausal subjects, with only two of the studies using control groups. The study criteria can be found in Table 3, and all results were compared to histology after endometrial tissue sampling.
Results of Sensitivity and Specificity of Elastography, in Detecting Endometrial Carcinoma, After Endometrial Tissue Sampling.
Elastography Results in Studies That Reported Differences in Strain Ratios and Stiffness Results, in Endometrial Carcinoma vs Benign Endometrial Pathology, After Tissue Sampling.
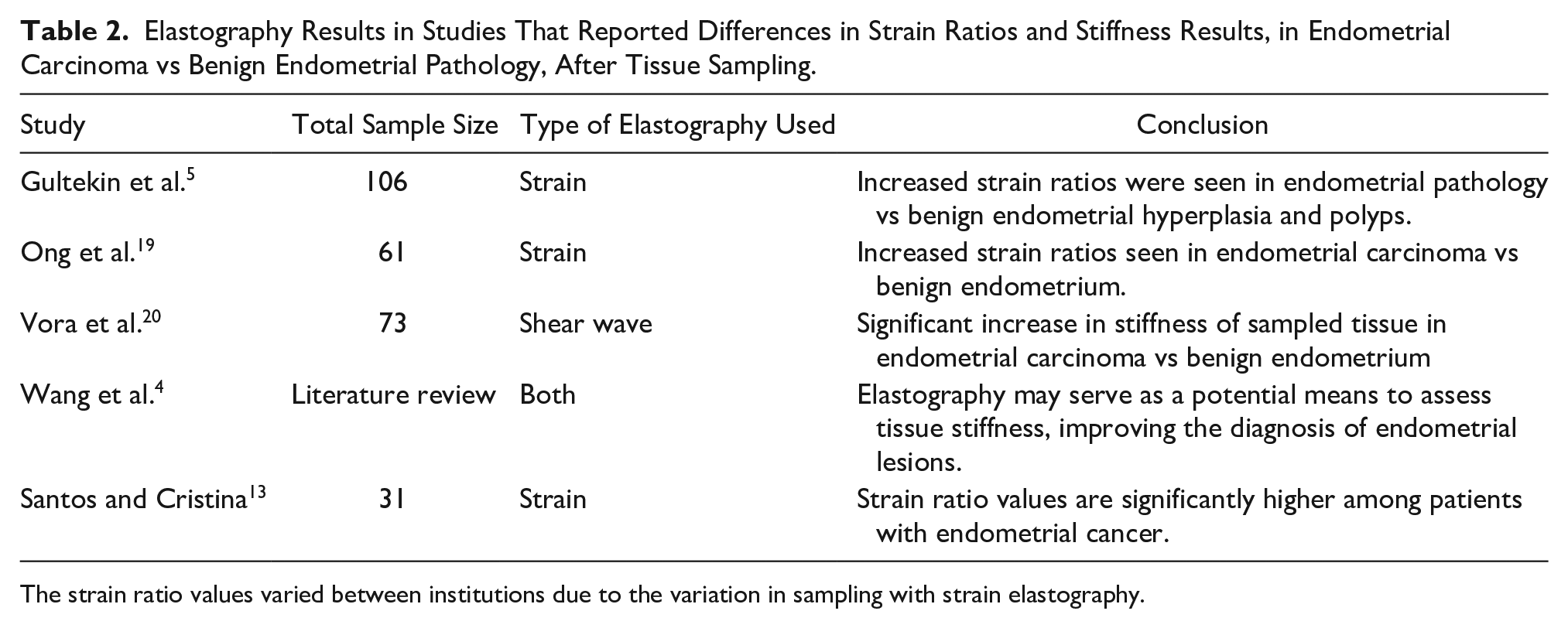
The strain ratio values varied between institutions due to the variation in sampling with strain elastography.
The Research Study Criteria Utilized by Each of the Authors, as Part of the Extracted Data for This Literature Review.
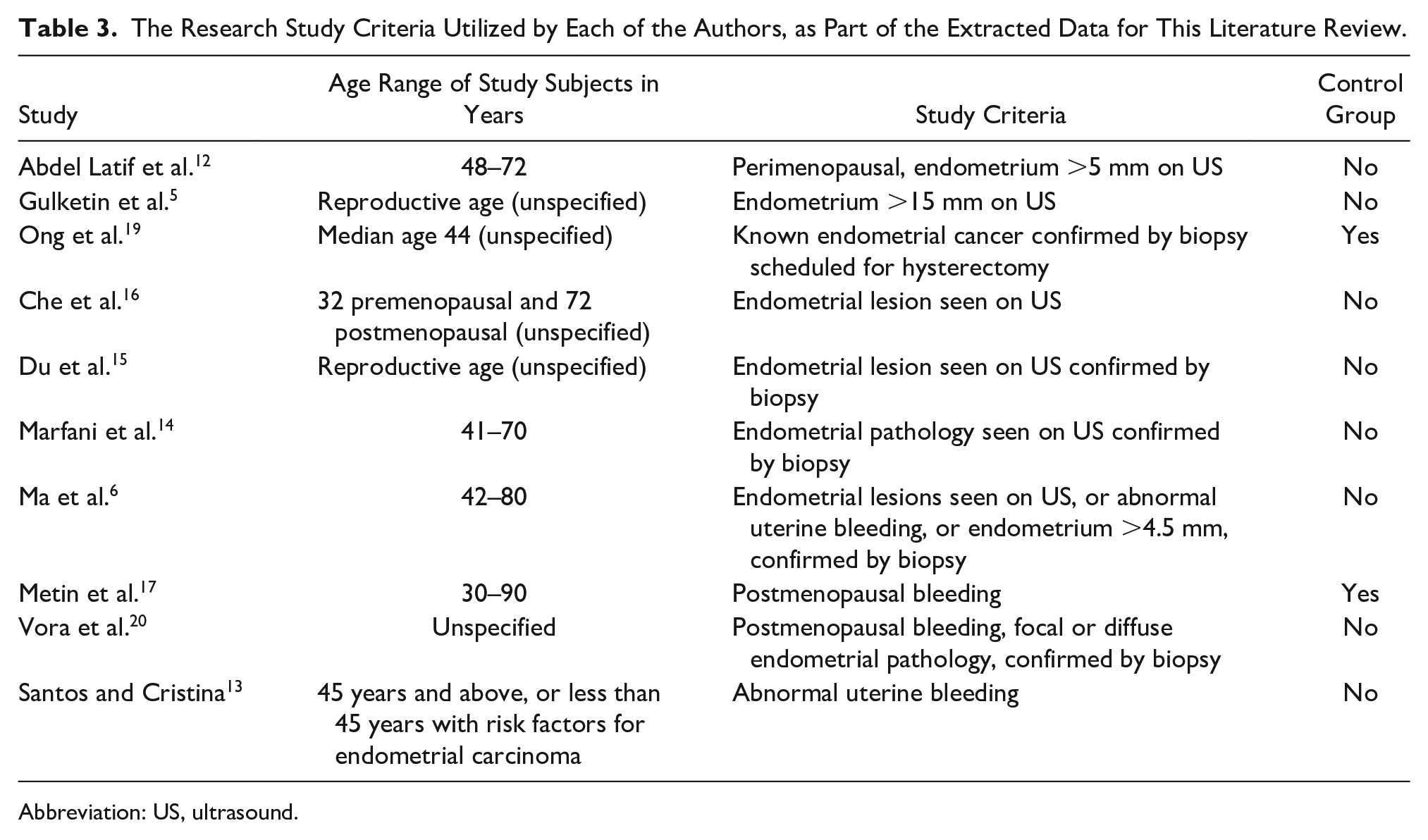
Abbreviation: US, ultrasound.
Two studies determined that elastography is excellent at distinguishing endometrial carcinoma from benign endometrial pathologies but could not distinguish between benign polyps and hyperplasia.5,14 Additional studies are needed in this area to determine if elastography can distinguish between these subgroups and how that affects the detection of early-stage endometrial carcinoma.
Table 1 shows no significant differences in the conclusions between strain and shear wave elastography. Both produce high sensitivity and specificity rates in determining endometrial carcinoma from benign endometrial pathology. However, between the studies that used strain elastography, there was a variance in the strain ratio values. Ong et al. 19 attributed these differences to the user dependence of strain elastography compared to shear wave elastography. While the results were conclusive and comparable across all studies, it is worth noting that shear wave elastography can provide more objective and reproducible measurements than strain elastography. 19
Whether elastography has been seen to reduce the amount of unnecessary invasive procedures remains to be seen. Ma et al. 6 suggested that elastography could not only improve the diagnostic accuracy of endometrial carcinoma but also has the potential to reduce the use of endometrial sampling by determining the nature of tissue without the use of histology. There were no studies found on this topic, but the current literature suggests that elastography could have a significant impact on how endometrial cancer is diagnosed.
Synthesis
Elastography is a promising tool in the diagnosis of endometrial carcinoma. This is a new and emerging application of elastography that has promising results. The high sensitivity and specificity of elastography in determining tissue stiffness have the potential to provide valuable information in endometrial pathology and other uterine pathology, such as adenomyosis. This exciting development offers great potential but needs universal, consistent approaches and studies of subgroups to be used alone without the use of biopsy and histology and be considered the standard of care. Determination of whether elastography can be used to approach early endometrial carcinoma detection needs to be addressed. Expanded research must be carried out on the differentiation of endometrial cancer from benign pathology but also on the ability of elastography to distinguish between benign pathologies. All the studies point to exciting developments for the future; however, there are many unanswered questions in the role of elastography and determining endometrial pathologies and processes.
Limitations
Elastography provides an excellent diagnostic tool for assessing endometrial carcinoma. High sensitivity and specificity were seen in the ability of both strain and shear wave elastography to measure tissue stiffness and distinguish carcinoma from benign endometrial pathology. However, there are issues to consider with the studies reviewed. Strain elastography has been proven to be more user-dependent with the difficulty of reproducing results with different operators. Shear wave imaging is more easily reproduced and objective, making it less user-dependent. Additional studies are needed to determine which of these methods is best with universal guidelines for conducting elastography studies on the endometrium. Consistency and objective measurement guidelines must be established to determine a standard of care with elastography imaging of the endometrium.
Due to the lack of studies found on the topic of elastography use in the endometrium, more studies are needed across a variety of different subgroups. The reviewed studies had small sample sizes ranging from 8 to 217 participants. Additional studies are needed with larger, increasingly diverse sample groups. In their literature review, Wang et al. 4 determined that elastography is helpful in diagnosing endometrial carcinoma but noted the need for further studies.
Most studies used a thick endometrium as the main criterion for inclusion; however, others used a thick endometrium and abnormal vaginal bleeding as criteria for their study. All studies used both premenopausal and postmenopausal women. The wide range of criteria (see Table 3) shows that focused studies within these subgroups are necessary. The lack of control groups in these studies is also concerning. Using only symptomatic women in a research study impacts the ability to draw meaningful conclusions about the study results. Only two of the reviewed studies used control groups to determine whether elastography showed a significant difference in tissue stiffness. Of those two, Metin et al. 17 found no statistical difference between endometrial hyperplasia and a control group.
Conclusion
Elastography is a valuable tool in differentiating between the stiffness of malignant and benign endometrial tissue. This emerging technology has the potential to aid in the diagnosing of endometrial carcinoma without the use of invasive tissue sampling procedures. The use of 2 different types of elastography without objective reproducibility limits how we can use the results of the current studies. Consistent practices and standards are needed for performing elastography to provide more reproducible results. For elastography to gain ground in the field of gynecology and become the standard of care, larger and more diverse studies are needed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.